The Gaucher Earlier Diagnosis Consensus point-scoring system for children and young adults: a retrospective and prospective evaluation in Korea
Seung Min Hahn, Minseok Kim, Youna Kim, Jiyoung Oh, Se Hee Kim, Hong Koh, Sung-Eun Kim, Nack-Gyun Chung, Ye Jee Shim, Hawk Kim, Jae Min Lee, Sung-Soo Yoon, Ho Joon Im, Hyoung Jin Kang, Young Rok Do, Chung Mo Nam, Chuhl Joo Lyu

TL;DR
A new scoring system for early detection of Gaucher disease in children and young adults shows high accuracy in Korean patients.
Contribution
The GED-C point-scoring system is validated for early diagnosis of Gaucher disease in pediatric and young adult populations.
Findings
The GED-C PSS achieved high sensitivity (1.0) and specificity (0.97) with a cutoff of 6.5.
Two confirmed Gaucher disease patients had distinct PSS scores from other participants.
The system is applicable across a wide age range (1 month to 40 years).
Abstract
Gaucher disease (GD) is an autosomal recessive condition caused by insufficient glucocerebrosidase activity. The Gaucher Earlier Diagnosis Consensus (GED-C) initiative created a point-scoring system (PSS) to facilitate the early identification of GD based on significant indicators and covariables. This study aimed to evaluate the applicability and utility of the GED-C PSS in pediatric and young adult patients in Korea. This study included both retrospective analysis and prospective recruitment. Subject recruitment involved 14 sites across 13 hospitals in Korea, where patients of any age meeting GED-C criteria were recruited, and blood samples were collected. Data of 513 subjects were analyzed and two patients were confirmed to have GD during prospective enrollment. The median age of participants was 10 years (range: 1 month to 40 years). Receiver operating characteristic analysis…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
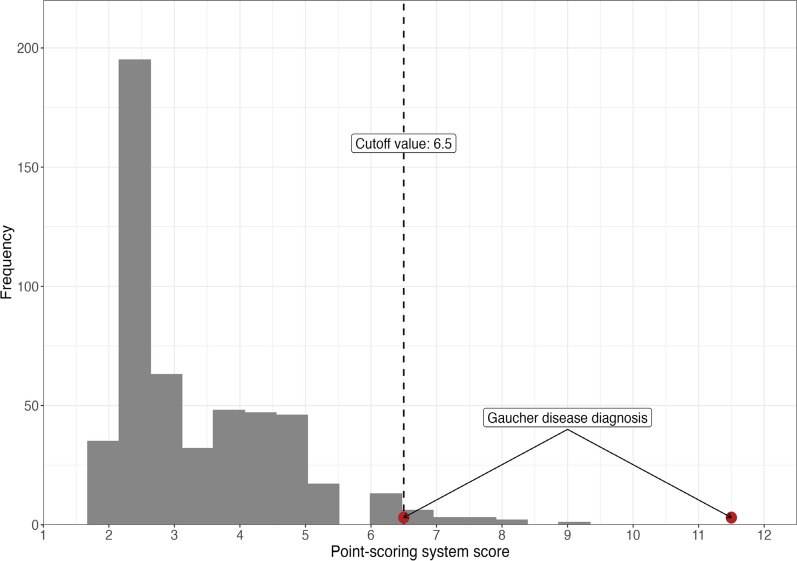 Figure 1
Figure 1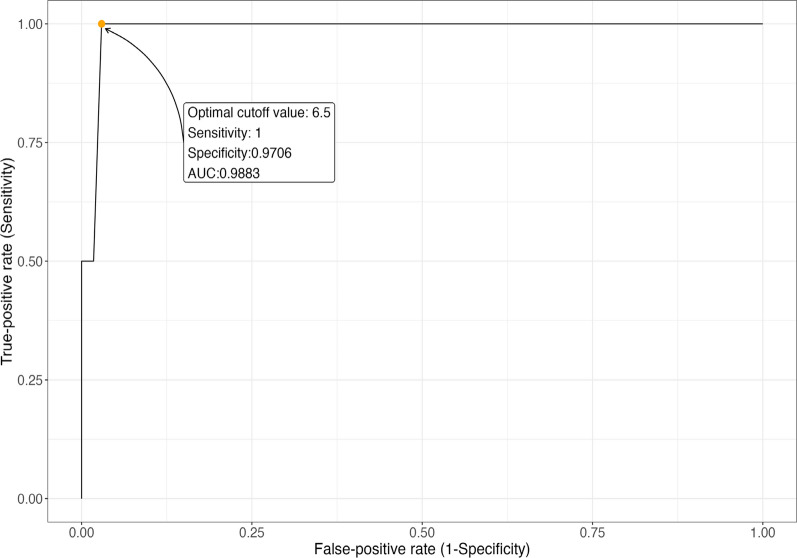 Figure 2
Figure 2- —Takeda Korea
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLysosomal Storage Disorders Research · Genomics and Rare Diseases · Autoimmune and Inflammatory Disorders Research
Background
Gaucher disease (GD) is an autosomal recessive metabolic disorder that impairs glycolipid recycling in cells [1, 2] due to deficient activity of the lysosomal enzyme glucocerebrosidase, leading to the accumulation of glucosylceramide in macrophages [1–3] known as Gaucher cells. This metabolic impairment causes cellular dysfunction and clinical abnormalities, primarily affecting the bone marrow, spleen, and liver, though other organs can also be involved. The enzyme deficiency may also impact cells beyond macrophages, such as hematopoietic progenitor cells, erythrocytes, mesenchymal cells, and hepatocytes, contributing to the diverse presentations of GD [2].
Over 400 variants of the pathogenic GBA1 gene located on chromosome 1 (1q21) have been identified as causes of GD [4, 5]. The phenotype of GD is variable; based on the extent and age of neurological involvement, three phenotypes have been suggested to classify GD: type 1 (nonneuronopathic), type 2 (acute neuronopathic), and type 3 (chronic neuronopathic). Type 1 is the most prevalent form of GD, typically presenting without neurologic impairment but with various manifestations such as hepatosplenomegaly, cytopenia, bone pain, or pulmonary involvement. Type 2 GD is the rarest form, known as the acute neuropathic type, and typically presents in infancy. Type 3 GD is characterized by a more indolent progression of neurologic impairment [1, 2].
Definitive diagnosis of GD can be confirmed by observing decreased glucocerebrosidase enzyme activity in the presence of a biallelic pathogenic GBA variants. While newborn screening (NBS) programs in various countries have demonstrated the feasibility and benefits of early GD detection and intervention [6–10], NBS for GD may lead to identifying individuals who do not require immediate treatment due to the disease’s variable presentation, as noted by the Delphi expert panel [11].
The Gaucher Earlier Diagnosis Consensus (GED-C) initiative suggested major signs and covariables of relevance in early GD to facilitate diagnosis by Delphi methodology [12]. For type 1 GD, seven major signs (splenomegaly, thrombocytopenia, bone manifestations, anemia, hyperferritinemia, hepatomegaly, and gammopathy) and two major covariables (family history, Ashkenazi-Jewish ancestry) were identified. For type 3 GD, nine major signs (splenomegaly, oculomotor disturbances, thrombocytopenia, epilepsy, anemia, hepatomegaly, bone pain, motor disturbances, and kyphosis) and one major covariable (family history) were identified. These parameters may help non-specialists identify GD and increase their level of suspicion [2, 12]. The proposed prototype point scoring system (PSS) by the GED-C panel effectively distinguished GD patients from those with overlapping symptoms [13–15].
According to rare disease registry data from the Korea Disease Control and Prevention Agency, annual newly diagnosed GD patients were only 1 in 2020, and 4 in 2021. Efforts to implement neonatal screening for lysosomal storage diseases, including GD, have only recently begun, and the disease still appears to be underdiagnosed in South Korea. This study aimed to determine the optimal cutoff value for GED-C PSS based on symptoms and test findings for early GD diagnosis in Korean patients. Additionally, we sought to identify the clinical manifestations of GD in Koreans and assess the utility of GED-C PSS, particularly in pediatric, adolescent, and young adult populations, given the limited research on these groups.
Methods
Point scoring
The GED-C PSS was used to estimate scores for each participant suspected of having GD (Table 1). Score for each factor was stratified (3 points, 2 points, 1 point, and 0.5 points) based on the likelihood of association with GD as determined by GED-C consensus. There is currently no validated threshold for the GED-C PSS score to be used as a screening cutoff. To broaden the range of patients eligible for screening, our research team planned to include all individuals with a GED-C PSS score of 2 points or higher.Table 1. Gaucher Earlier Diagnosis Consensus (GED-C) regarding signs and co-variables with their scores in point-scoring system (PSS). If the total PSS corresponding is 2 or higher, the individual is eligible to enroll in the prospective or retrospective studyScoreSign or co-variableMajor signs and co-variables 3 pointsSplenomegaly (≥ 3 × normal)Disturbed oculomotor function (slow horizontal saccades with unimpaired vision) 2 pointsThrombocytopenia, mild or moderate: 50 × 10^3^/μL ≤ platelet count < 150 × 10^3^/μLBone issues, including pain, crises, avascular necrosis and fracturesFamily history of Gaucher diseaseAnemia, mild or moderate: 1 ≤ age < 2: 8.0 g/dL ≤ hemoglobin < 10.5 g/dL 2 ≤ age < 12: 8.0 g/dL ≤ hemoglobin < 11.5 g/dL 12 ≤ age < 19: 8.0 g/dL ≤ hemoglobin < 12.0 g/dL 19 ≤ age: 8.5 g/dL ≤ hemoglobin < 12.0 g/dL)Hyperferritinemia, mild or moderate: 300 ng/mL ≤ serum ferritin < 1000 ng/mLJewish ancestryDisturbed motor function (impairment of primary motor development)Hepatomegaly, mild or moderate (≤ 3 × normal)Myoclonus epilepsyKyphosisGammopathy—monoclonal or polyclonal 1 pointAnemia, severe: 1 ≤ age < 19: hemoglobin < 8.0 g/dL19 ≤ age: hemoglobin < 8.5 g/dLHyperferritinemia, severe: Serum ferritin ≥ 1000 ng/mL)Hepatomegaly, severe (> 3 × normal)Thrombocytopenia, severe: Platelet count < 50 × 103/μL)Minor signs and co-variables 0.5 pointsGallstonesBleeding, bruising or coagulopathyLeukopeniaCognitive deficitLow bone mineral densityGrowth retardation including low body weightAstheniaCardiovascular calcificationDyslipidemiaElevated ACE levelsFatiguePulmonary infiltratesAge < 19 yearsFamily history of Parkinson’s diseaseBlood relative who died of fetal hydrops and/or with diagnosis of neonatal sepsis of uncertain etiology
Patients and data collection
This study involved both retrospective data analysis and prospective patient recruitment. The data collection and patient enrollment were performed between May 2019 and November 2023. Individuals already diagnosed with GD were excluded from the study.
In the retrospective study, data from patients below 19 years of age who visited Severance Hospital within the 5 years prior to study approval month (Visit 0) were reviewed. Patients exhibiting symptoms suggestive of GD and meeting GED-C criteria (Table 1) were included. If the total PSS corresponding was 2 or higher, the individual was eligible to enroll in the study. When these patients subsequently visited the outpatient clinic (Visit 1), approximately 3 mL of venous blood was drawn using a syringe for a dry blood smear test to confirm GD. Blood was smeared on a filter card and sent to a central laboratory.
For the prospective study, 14 sites across 13 hospitals in Korea recruited patients. Since the GED-C criteria may not be familiar to all clinicians, we provided thorough education and training to the investigators at the start of the study to ensure a clear understanding of the criteria. This training was repeated as necessary to maintain consistent application of the criteria. Additionally, we implemented a process of data verification during data collection to ensure accuracy and consistency. Patients of pediatric age and young adults who visited outpatient clinics or were hospitalized and exhibited symptoms suggestive of GD and met the GED-C criteria (Table 1) were recruited and scored. Subjects with PSS 2 or higher were eligible to enroll in the study. During their visit (Visit 1), blood was drawn and tested.
Statistical analysis
A receiver operating characteristic (ROC) curve was used to summarize diagnostic performance in terms of sensitivity and specificity of various PSS cutoff values for distinguishing between GD and non-GD cases. The area under the ROC curve (AUC) and the corresponding 95% confidence interval (CI) were calculated using the bootstrapping method. The Youden index (sensitivity + specificity—1) was used to determine the statistically derived optimal cutoff on the ROC curve for diagnosing GD [16]. All statistical analyses were performed using R (version 4.3.0).
Results
Of the 518 registered participants, 513 were analyzed after excluding five due to dropouts and duplicates. The retrospective and prospective groups comprised 162 and 351 participants, respectively. The median age of participants was 10 years (range: 1 month to 40 years). Of the total number of patients, 478 visited for hematologic concerns, and 35 were referred from other specialties for consultation. Most common hematologic abnormalities were thrombocytopenia (55%), anemia (67%), and leukopenia (99%) (Table 2). Two patients were confirmed to have GD.Table 2. Patients’ characteristics and demographics according to Gaucher early diagnosis consensus, point-scoring systemCharacteristicScoreNon-Gaucher (N = 511)Gaucher (N = 2)Cohort Prospective349 (68%)2 (100%) Retrospective162 (32%)0 (0%)Overall PSS score Mean (SD)3.47 (1.26)9.00 (3.54) Range2.00, 9.006.50, 11.50 Median (IQR)3.00 (2.50, 4.50)9.00 (7.75, 10.25)Assessed GED-C PSS sign or co-variablesSplenomegaly (≥ 3 × normal) Yes3 points17 (3.3%)1 (50%) No472 (92%)1 (50%) Unknown22 (4.3%)0 (0%)Disturbed oculomotor function (slow horizontal saccades with unimpaired vision) Yes3 points2 (0.4%)0 (0%) No507 (99%)2 (100%) Unknown2 (0.4%)0 (0%)Thrombocytopenia Mild or Moderate2 points173 (34%)1 (50%) Severe1 points108 (21%)1 (50%) No225 (44%)0 (0%) Unknown5 (1.0%)0 (0%)Anaemia Mild or Moderate2 points285 (56%)0 (0%) Severe1 points58 (11%)0 (0%) No163 (32%)2 (100%) Unknown5 (1.0%)0 (0%)Leukopenia Yes0.5 points160 (31%)1 (50%) No346 (68%)1 (50%) Unknown5 (1.0%)0 (0%)Hyperferritinaemia Mild or Moderate2 points40 (7.8%)1 (50%) Severe1 points25 (4.9%)0 (0%) No207 (41%)1 (50%) Unknown239 (47%)0 (0%)Hepatomegaly Mild or Moderate2 points59 (12%)1 (50%) Severe1 points2 (0.4%)0 (0%) No426 (83%)1 (50%) Unknown24 (4.7%)0 (0%)Dyslipidemia Yes0.5 points13 (2.5%)0 (0%) No437 (86%)1 (50%) Unknown61 (12%)1 (50%)Elevated angiotensin-converting enzyme levels Yes0.5 points2 (0.4%)0 (0%) No68 (13%)0 (0%) Unknown441 (86%)2 (100%)Family history of Gaucher disease Yes2 points0 (0%)0 (0%) No505 (99%)2 (100%) Unknown6 (1.2%)0 (0%)Disturbed motor function (impairment of primary motor development) Yes2 points1 (0.2%)2 (100%) No509 (100%)0 (0%) Unknown1 (0.2%)0 (0%)Myoclonus epilepsy Yes2 points13 (2.5%)1 (50%) No496 (97%)1 (50%) Unknown2 (0.4%)0 (0%)Cognitive deficit Yes0.5 points5 (1.0%)1 (50%) No500 (98%)0 (0%) Unknown6 (1.2%)1 (50%)Gammopathy—monoclonal or polyclonal Yes2 points3 (0.6%)0 (0%) No94 (18%)1 (50%) Unknown414 (81%)1 (50%)Bone issues, including pain, crises, avascular necrosis, and fractures Yes2 points6 (1.2%)0 (0%) No492 (96%)2 (100%) Unknown13 (2.5%)0 (0%)Kyphosis Yes2 points0 (0%)0 (0%) No505 (99%)2 (100%) Unknown6 (1.2%)0 (0%)Low bone mineral density Yes0.5 points3 (0.6%)0 (0%) No77 (15%)1 (50%) Unknown431 (84%)1 (50%)Jewish ancestry Yes2 points0 (0%)0 (0%) No505 (99%)2 (100%) Unknown6 (1.2%)0 (0%)Gallstones Yes0.5 points5 (1.0%)0 (0%) No215 (42%)2 (100%) Unknown291 (57%)0 (0%)Bleeding, bruising, or coagulopathy Yes0.5 points55 (11%)0 (0%) No453 (89%)2 (100%) Unknown3 (0.6%)0 (0%)Growth retardation including low body weight Yes0.5 points10 (2.0%)1 (50%) No500 (98%)1 (50%) Unknown1 (0.2%)0 (0%)Asthenia Yes0.5 points4 (0.8%)0 (0%) No504 (99%)2 (100%) Unknown3 (0.6%)0 (0%)Cardiovascular calcification Yes0.5 points0 (0%)0 (0%) No109 (21%)1 (50%) Unknown402 (79%)1 (50%)Fatigue Yes0.5 points17 (3.3%)0 (0%) No488 (95%)1 (50%) Unknown6 (1.2%)1 (50%)Pulmonary infiltrates Yes0.5 points0 (0%)0 (0%) No179 (35%)1 (50%) Unknown332 (65%)1 (50%)Age ≤ 18 years Yes0.5 points448 (88%)1 (50%) No63 (12%)1 (50%) Unknown0 (0%)0 (0%)Family history of Parkinson disease Yes0.5 points0 (0%)0 (0%) No499 (98%)2 (100%) Unknown12 (2.3%)0 (0%)Blood relative who died of fetal hydrops and/or with diagnosis of neonatal sepsis of uncertain etiology Yes0.5 points0 (0%)0 (0%) No501 (98%)2 (100%) Unknown10 (2.0%)0 (0%)GED-C, Gaucher Early Diagnosis Consensus; PSS, point-scoring system
ROC analysis and PSS cutoff value
The ROC curve and cutoff value for the GD PSS score were derived from analyzing 513 participants. A histogram showed that the PSS scores of the two GD patients were distinct from those of other participants (Fig. 1). The cutoff point was identified as 6.5, with an AUC of 0.9883 (95% CI: 0.9677-1). The sensitivity and specificity at this cutoff were 1.0 and 0.9706, respectively (Fig. 2).Fig. 1. Histogram of proto-type point scoring systemFig. 2Receiver-operating characteristic (ROC) curve
Prospective diagnosis of GD in two patients
Two patients were diagnosed with GD during prospective enrollment. The PSS scores were clearly distinct between GD and non-GD patients, as described in Table 3. Among the two confirmed cases, the first patient was a 23-year-old male with mild thrombocytopenia, disturbed motor function, myoclonic epilepsy, and cognitive deficit, yielding a PSS score of 6.5. The second was a 7-month-old infant with severe splenomegaly, thrombocytopenia, leukopenia, mild hyperferritinemia, hepatomegaly, disturbed motor function, and growth retardation, resulting in a PSS score of 11.5.Table 3. Comparison between non-Gaucher patients with Gaucher disease patientsCharacteristicNon-Gaucher (N = 511)Gaucher (N = 2)Cohort Prospective349 (68%)2 (100%) Retrospective162 (32%)0 (0%)Overall PSS score Mean (SD)3.47 (1.26)9.00 (3.54) Range2.00, 9.006.50, 11.50 Median (IQR)3.00 (2.50, 4.50)9.00 (7.75, 10.25)Assessed GED-C PSS sign or co-variables Splenomegaly (≥ 3 × normal)17 (3.3%)1 (50%) Disturbed oculomotor function (slow horizontal saccades with unimpaired vision)2 (0.4%)0 (0%) Thrombocytopenia281 (55%)2 (100%) Anaemia343 (67%)0 (0%) Leukopenia160 (31%)1 (50%) Hyperferritinaemia65 (13%)1 (50%) Hepatomegaly61 (12%)1 (50%) Dyslipidemia13 (2.5%)0 (0%) Elevated angiotensin-converting enzyme levels2 (0.4%)0 (0%) Family history of Gaucher disease0 (0%)0 (0%) Disturbed motor function (impairment of primary motor development)1 (0.2%)2 (100%) Myoclonus epilepsy13 (2.5%)1 (50%) Cognitive deficit5 (1.0%)1 (50%) Gammopathy—monoclonal or polyclonal3 (0.6%)0 (0%) Bone issues, including pain, crises, avascular necrosis, and fractures6 (1.2%)0 (0%) Kyphosis0 (0%)0 (0%) Low bone mineral density3 (0.6%)0 (0%) Jewish ancestry0 (0%)0 (0%) Gallstones5 (1.0%)0 (0%) Bleeding, bruising, or coagulopathy55 (11%)0 (0%) Growth retardation including low body weight10 (2.0%)1 (50%) Asthenia4 (0.8%)0 (0%) Cardiovascular calcification0 (0%)0 (0%) Fatigue17 (3.3%)0 (0%) Pulmonary infiltrates0 (0%)0 (0%) Age ≤ 18 years448 (88%)1 (50%) Family history of Parkinson disease0 (0%)0 (0%) Blood relative who died of fetal hydrops and/or with diagnosis of neonatal sepsis of uncertain etiology0 (0%)0 (0%)GED-C, Gaucher Early Diagnosis Consensus; PSS, point-scoring system
Discussion
The GED-C PSS was first validated in the UK with 25 patients [13] and in a biobank study of Finland [14]. The UK study found that the mean PSS score (divided by the number of factors included) in GD patients was 1.08 (standard deviation, 0.25) compared to 0.58 (standard deviation, 0.31) in non-GD individuals, while a PSS score of 0.82 distinguished GD with a sensitivity of 100% and a specificity of 71% [13]. The Finland study, utilizing both retrospective data from 170,000 adults in collaboration with the Finland Biobank and prospective data from new patients, discovered an indicative PPS of 6–18.5 for confirmed GD patients [14].
In contrast to the other two earlier studies, this Korean study differed in that most data were collected prospectively based on physicians’ suspicions. The number of GD patients diagnosed was low, with only two confirmed cases. The global incidence of type I GD is 1 in 1,000 in Ashkenazi Jews, generally 1 in 30,000 to 40,000 among other ethnicities, and types 2 and 3 occur even less frequently [1, 2]. Considering the low incidence rate, statistically, it is possible that no patients would have been diagnosed with GD in the study. However, this study demonstrated that when clinically suspected patients are screened, the diagnosis can be made at a much higher rate. This suggests that the real-world implementation of GED-C PPS allows for determining a diagnosing threshold, as demonstrated in previous studies.
One pediatric patient with type 2 GD and one adult with type 3 GD were diagnosed in the study. We observed that the PSS of these two GD patients deviated significantly from that of the non-GD group. As the diverse phenotypes of type 3 GD may hinder a timely diagnosis if not properly suspected, GED-C PSS could be used as a tool to assist diagnosis.
This study was also unique in that most of the participants were pediatric patients, demonstrating the applicability of GED-C PSS in this age group. Globally, while some countries have included Gaucher disease (GD) in their newborn screening programs, the majority have not. In such settings, it is crucial for clinicians to actively suspect and diagnose GD. Therefore, the significance of our study lies in demonstrating that the GED-C PSS can serve as a helpful tool in identifying and diagnosing this rare condition in real-world clinical practice.
This study has several limitations. First, we established age-specific hemoglobin criteria for anemia, distinct from the original GED-C consensus, in order to diagnose anemia in pediatric patients. Second, the potential for variability in the results could have arisen due to differences in the screening items used among the various physicians involved. However, in real-world clinical practice, this approach can be reflective of it. Lastly, including more patients would have resulted in the identification of more cases and thus more reliable results.
Conclusions
This study with over five hundred patients was the first of its kind to investigate the clinical use of GED-C PSS prospectively, as opposed to earlier studies. Approaches including newborn screening, diagnostic algorithms, and scoring-based screening as used in this study, should be considered for timely GD diagnosis given its prevalence and available resources. This study provides direct evidence that GED-C scoring can be used for diagnosing GD in both children and adults.