Intensive community and home-based treatments for eating disorders: a scoping review
Başak İnce, Amelia Austin, Matthew D. Phillips, Elizabeth Fordham, Erica Cini, Ulrike Schmidt

TL;DR
This review explores community and home-based treatments for eating disorders as alternatives to hospital care, finding them promising but needing more rigorous research.
Contribution
The paper provides the first scoping review of intensive community and home-based treatments for eating disorders, highlighting their potential and current research gaps.
Findings
Community and home-based treatments showed improved clinical outcomes, high patient satisfaction, and cost-effectiveness.
Home-based treatments focused on children and adolescents with anorexia nervosa, emphasizing family-based approaches.
Community treatments varied in age groups and diagnoses, often combining cognitive and dialectical behavioral therapies.
Abstract
Intensive community treatment (ICT) and home-based treatment (HBT) have emerged as valuable alternatives to institution-based intensive treatments (inpatient or day patient) for severe mental illnesses. Although potential benefits of ICT and HBT for eating disorders (EDs) have been proposed, this area of research remains largely unexplored. A scoping review was conducted to map the available literature. Four databases (PubMed, PsycInfo, MEDLINE, Web of Science), grey literature, and trial registries were searched. Sources were included if they presented treatments offering more than two planned therapeutic contacts per week for at least part of the program, excluding physical monitoring contacts, for patients diagnosed with any ED across all ages. Forty-six sources met the inclusion criteria (ICT: n = 31; HBT: n = 15), with most studies from Europe (n = 23) and the USA (n = 18). Among…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
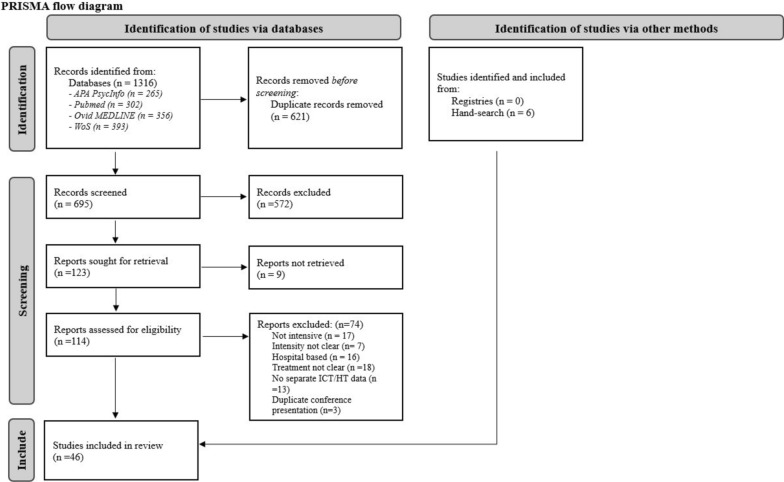 Figure 1
Figure 1- —Medical Research Council/Arts and Humanities Research Council/Economic and Social Research Council Adolescence, Mental Health and the Developing Mind
- —Cumming School of Medicine Postdoctoral Scholar Award
- —National Institute for Health and Care Research (NIHR) Maudsley Biomedical Research Centre (BRC)
- —NIHR Evaluation, Trials and Studies Coordinating Centre (NETSCC)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEating Disorders and Behaviors · Flow Experience in Various Fields · Diversity and Impact of Dance
Introduction
Eating disorders (EDs) are “disabling, deadly, and costly” psychiatric disorders characterized by persistent dysfunctional eating and/or weight-control behaviors [1] (p. 899). When not treated rapidly and effectively, EDs may follow a relapsing or chronic course with reduced likelihood of full recovery. The psychological, social, and economic burdens imposed by EDs are considerable, affecting not only the individual with the illness but also their caregivers and wider society [2].
People from all genders, ages, ethnicities, body types and weights, sexual orientations, and socioeconomic backgrounds are affected by EDs [3]. The prevalence of EDs has been continually rising across all age groups, with estimates in 2019 suggesting that globally about 55.5 million (95% UI, 38.7–75.2) have an ED [4–6]. Accompanying the rise in ED prevalence in the community, the need for hospital admissions is also increasing. For instance, ED-related hospital admissions in England doubled between 1998 and 2020 [7]. The COVID-19 pandemic has further escalated the number of people presenting with ED symptoms in the general population as well as heightening severity among those previously diagnosed with an ED [8, 9]. The impact of the COVID-19 pandemic led to an average increase in ED hospital admissions of 48% internationally [8]. Unsurprisingly, the rise in prevalence and severity of EDs have resulted in growing demand for access to specialist services and different forms of intensive treatments for EDs [4, 9, 10].
ED treatments often follow a stepped-care model, tailoring the intensity of treatment to match symptom severity and presentation. International evidence-based guidelines recommend specialized outpatient treatment as a first option for most, while more intensive treatment options (i.e., day patient/partial hospitalization, inpatient and residential care) are considered in cases where the person has not benefitted from outpatient treatment, or where there is high medical risk [11–15]. This stepped-care approach allows patients to start treatment at a lower intensity, progressing to more intensive care if deemed necessary to achieve recovery. This approach also facilitates transition in the other direction, from intensive institution/hospital-based care to outpatient care.
Higher level institution-based care including inpatient treatment (IPT), residential care (RC), partial hospitalization programs (PHP), and day patient treatments (DPT) are usually provided by multidisciplinary specialist ED services combining medical, psychological and nutritional support. These approaches vary in intensity, with IPT/RC being the most intensive and DPT/PHP often serving as a step-down from inpatient care, usually involving 6–10 h per day, 3–7 days per week. The structure, intensity, and labeling of these programs may vary across healthcare systems and countries. Family and caregiver involvement also often plays a vital role in these treatments across all age groups, enhancing treatment and providing a more comprehensive approach to care. These institution-based traditional intensive treatments have clear benefits, such as promoting recovery in a safe and supportive environment, offering regular meal support, restoring weight and managing medical risks and improving physical health [16–19]. IPT in particular may also provide families with much needed respite. Higher-level institution-based care separates patients from their everyday environments, a separation that is total in inpatient and residential programs and substantial in day patient or partial hospitalization settings. This can lead to notable challenges, such as risk of institutionalization, reduced patient autonomy, strict institutional schedules and routines, geographical inequality and disruptions to daily routines [19–21]. Furthermore, the cost of these treatments and risk of relapse following discharge are high [22–24].
To overcome the challenges of traditional institution-based intensive treatments, intensive community-based (ICT) and home-based treatments (HBT) have been proposed as feasible and potentially cost-effective alternatives. ICT provides treatment, care, and support in community settings (e.g., specialized intensive outpatient settings, schools, primary care), while HBT provides these services directly in the patient’s home, both of which enable patients and families to manage their illness either in their everyday environments or in a non-institutional setting.
The effectiveness of ICTs and HBTs has been investigated across a range of psychiatric disorders, including affective disorders, psychosis, personality disorders, and substance use disorders, and across different age groups. These approaches have been associated with improved clinical outcomes, increased treatment adherence, and reductions in hospital admissions, readmissions, length of stay, and overall treatment costs [25–28]. For instance a pragmatic randomized controlled trial involving 707 adults in need of immediate hospital admission for various mental health crises (e.g., schizoaffective disorder, bipolar disorder, personality disorder) found that home treatment resulted in 30.4% fewer hospital bed days over 24 months compared to standard inpatient care, with comparable clinical and social outcomes and similar levels of patient satisfaction [29]. Furthermore, two recent meta-analytic reviews support the effectiveness of ICTs and HBTs as alternatives to institution-based care: one showed no significant differences in psychosocial and psychopathology outcomes between HBT and inpatient care for children and adolescents with psychiatric disorders [30], and the other found similar reductions in PTSD symptoms between residential and intensive outpatient treatments in military populations [31].
With the growing body of research on alternatives to traditional institution-based intensive treatments for various psychiatric disorders showing encouraging findings, it is timely to assess their potential utility in EDs. Efforts to develop and investigate intensive community-based and home-based treatments, have been supported by recommendations from recent reports by BEAT, the UK's leading charity for ED patients and caregivers [32, 33].
However, despite the proposed advantages of ICT and HBT for the treatment of EDs, which could provide similar outcomes to IPT while reducing healthcare costs and being potentially more acceptable to patients and their families, a comprehensive review of research focusing on these treatments has not yet been conducted. Therefore, we aimed to map the available literature on intensive community and home treatments for EDs by addressing the following research questions:
- What is the extent of the available literature on intensive community and home-based treatments for children, adolescents and adults with EDs?
- How are intensive community and home-based treatments for EDs conceptualized and implemented across the age range?
- What is the available evidence on the efficacy, acceptability, and cost-effectiveness of intensive community and home-based treatments for eating disorders (EDs)?
The third question was included to identify study designs, outcomes and gaps in the knowledge base, that together may inform the development of questions for a future systematic review [34].
Method
A scoping review methodology was used in this study to explore the emerging knowledge on intensive community (ICT) and home-based treatments (HBT) for children, adolescents and adults with EDs. Details on the methodology of this review can be found in the published protocol [35]. This study was designed and conducted in compliance with the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocol Extension for Scoping Reviews checklist (PRISMA-ScR) [36] and the Joanna Briggs Institute (JBI) Reviewer’s Manual [37]. The JBI Manual provides comprehensive methodological guidance for conducting scoping reviews, including when such reviews are appropriate, how to systematically extract, analyze, and present data, and how to interpret implications for practice and research. It is aligned with PRISMA-ScR and promotes methodological rigor and transparency, particularly in the assessment and coding of evidence.
Eligibility criteria
The eligibility criteria for this review as outlined in the protocol were: (1) sources on individuals with EDs from all age and gender groups; (2) studies investigating ICT and HBT for EDs that offer more than two planned therapeutic contacts per week for at least a portion of their treatment protocol, excluding physical monitoring contacts; (3) sources using quantitative, qualitative, mixed methods, descriptive and case study methodologies and designs; (4) any type of evidence source, including peer-reviewed articles, book chapters, dissertations, theses, conference abstracts, non-peer-reviewed articles, and trial registries; and (5) publications in English. We made one slight change to the eligibility criteria since the publication of the protocol [35], which was to include studies focused on families/caregivers and healthcare providers (i.e., not just patients) impacted by or working in ICT or HBT. Additionally, the third research question was amended to identify and map the breadth of available evidence on the efficacy, acceptability and cost-effectiveness of ICTs and HBTs for EDs, to better align with scoping review methodology guidance [34, 38].
Exclusion criteria included: (1) sources on mixed psychiatric populations where no separate data for EDs are available; (2) describing non-intensive treatments (i.e., offering two or fewer therapeutic contacts per week); (3) describing institution/hospital-based treatments (i.e., inpatient and day patient); (4) not providing separate outcome for ICT and or HBT (i.e., presenting outcomes combined with other settings) and (5) review articles and meta-analyses.
Search strategy
The search strategy adhered to the protocol [35]. In brief, a systematic literature search was conducted in four main databases (PubMed, PsycInfo, MEDLINE, Web of Science) and six grey literature databases (Scopus, Google Scholar, US ClinicalTrials.gov, WHO International clinical trials registry platform search portal, ISRCTN Registry, and the European Union Clinical Trials Register). An additional hand search was conducted on relevant journals and reference lists of papers in this review. The search terms included variations of “feeding and eating disorders”, “community treatment”, “intensive outpatient”, and “home treatment”. The exact search terms are presented in the supplemental material 1. The cut-off date for the searches in the databases was 13th of January 2025.
Study selection
Identified studies were imported into Endnote citation management software [39] and duplicates were removed. The references were then transferred to Rayyan, a systematic review management software [40], where title, abstract and full-text screening took place. For conference abstracts where no full text was readily available (n = 4), we contacted the corresponding authors to inquire about the full texts. Three responded, and we were able to obtain the full texts from two of these. All titles, abstracts and full texts of identified sources were screened by at least two researchers. Discrepancies between raters were resolved by discussion, and when necessary, a third rater conducted an independent screening.
Data charting, extraction, and analysis
The data charting form was developed by the lead author in consultation with the co-authors (Please see Supplemental material 2). Subsequently, data were extracted and charted into a structured table within an Excel spreadsheet, aligning with the objectives of this review. A minimum of two researchers independently completed data extraction and charting for each source included. Extracted data included study details (authors, year, country, design, setting), participant characteristics (sample size, diagnosis, age, sex, gender, gender identity, race/ethnicity, socioeconomic status), treatment specifics (programs, population, admission criteria, treatment model, meal support, length, intensity, delivery mode, professionals involved, carer/family involvement), ED-related outcomes (e.g., body mass index, changes in symptoms), feasibility, acceptability, cost-effectiveness, and qualitative outcomes.
A narrative synthesis approach was adopted for analysis due to heterogeneity in the methodologies employed across sources. For each included source, we characterized the types of evidence using the JBI Levels of Evidence, which categorize study designs and assess the strength of evidence across domains of (i) effectiveness, (ii) meaningfulness, and (iii) economic evaluations [41].
Results
The results are presented in accordance with the research questions, with a specific focus on mapping the body of literature across different age groups (children and adolescents, adults, and mixed-age populations) to explore similarities and differences in the available research.
Extent of the literature
After removal of duplicates, a total of 695 unique sources were identified for screening from database searches, grey literature, and hand searches. Nine papers were directly excluded during title and abstract screening and were not evaluated for inclusion criteria, as full texts in English were unavailable. Abstracts of these sources are presented in Supplemental material 3. Full text of 114 sources were screened, and among those 46 sources were included in this review (see Fig. 1 for PRISMA flowchart), with 31 of these focusing on intensive community treatments (ICT) and 15 on home-based treatments (HBT). When presenting the treatments, we kept the terminology used by the original sources whenever possible. For programs offering a mixture of ICT and HBT, we categorized them according to the primary treatment setting described.Fig. 1PRISMA flow diagram
Most of the 46 included sources, originated from Europe (n = 23), followed by the USA (n = 18), Canada (n = 3), Colombia (n = 1), and Israel (n = 1). While the majority (12 out of 15) of HBT programs took place in Europe, the distribution of ICT was more geographically diverse. The majority of the included sources were published in peer-reviewed journals (n = 35), while seven were unpublished theses/dissertations, three were conference abstracts, and one was an unpublished paper.
Participants’ baseline sociodemographic characteristics are presented in Table 1. In brief, the studies focusing on children and adolescents (n = 22) and adults (n = 17) were similar in numbers. Fourteen sources included only female participants, while only three reported on inclusion of non-binary and/or transgender individuals. Participants and/or target population in the sources included were primarily diagnosed with anorexia nervosa (AN; n = 16) or a mixture of different EDs (n = 18). Reporting on socioeconomic status (n = 6) and ethnicity/race (n = 15) was limited.Table 1. Details of included sources and sociodemographic characteristics of participantsAuthor(s)CountrySample sizeMean/median age at baselineSex, gender, and gender identity*Race and ethnicitySocioeconomic statusHome-based treatmentsBesse-Flütsch et al. [42]Switzerland90 adolescent patients + parents/caregivers (planned)12–18 (planned)NANANABezance and Holliday [43]UK9 mothers of adolescent patientsPatients: 13–16Mothers: 40–63NRNRNRClark-Stone et al. [44]UK33 adolescent patients + 6 parentsM = 14 years 7 monthsRange: 11 years and 10 months to 17 years and 10 monthsFemale: 100%NRNRDahmen et al. [46]Germany240 patients (planned)12–18 (planned)NANANADaniel et al. [64]France(i) Tube feeding (TF) + CBT: 61(ii) Tube feeding (TF) alone: 57(i) TF + CBT: M(SD) = 26.7 (6.4)(ii) TF alone = 28.6 (6.6)Female: 100%NRNRFlütsch et al. [45]Switzerland45M(SD) = 15.6 (1.8)Range: 10.7–19.6Female: 95.5% (n = 3)Male: 4.5% (n = 2)NRNRGoldschmidt et al. [48]USANA12–18 (planned)NANANAGoldschmidt et al. [47]USANANANANANAHeider et al. [49]Germany21M(SD) = 15.10 (1.16)Range: 12–18Female: 100%NRNRHerpertz-Dahlmann et al. [50]Germany22M(SD) = 15.06 (1.15)Range: 13.17- 17.03Female: 100%NRNRLatzer et al. [51]Israel3Ages: 13; 15; 16.5Female: 100%NRNRMayr et al. [52]Switzerland61M(SD) = 15.6 years (1.8) Range: 10.7–19.6 yearsFemale: 95.1% 58 (n = 58)Male: 4.9% (n = 3)NRNRMorón-Nozaleda et al. [53]Spain59M (SD) = 14.69 (1.67)Female: 100%NRNRPauli et al. [54]Switzerland(i) HBT + FBT: 45(ii) FBT only: 22(i) HBT + FBT: M(SD) = 15.6 (1.8)(ii) FBT only: M(SD) = 15.6 (1.8)Female: 95.5% (n = 63)Male: 4.5% (n = 3)NRNRTsiaka and Bletsos [81]Greece1014–35 yearsNRNRNRCommunity-based treatmentsBlalock et al. [82]USA57 patientsM(SD) = 29.91 (11.91)Female: 96% (n = 53)White-Caucasian: n = 44 (80%)Other: n = 13 (20%)NRChiumiento [55]USA205 patients + 289 parentsM(SD) = 15 (1.6)Range: 11–19Female: 92% (n = 266)Male: 8% (n = 23)NRNRCrenshaw [65]USA10Median = 39Range: 27–59Female: 100%White-Caucasian: n = 8 (80%)Jewish-Caucasian: n = 1 (10%)Black: n = 1 (10%)1 identified as lower middle class, 7 as middle class and 2 as upper middle classDeumens et al. [66]Netherlands182M(SD) = 35.1 (8.5)Range: 18–57Female: 100%NRNRDoyle et al. [56]USA44Range: 10–18Female: 100%NRNRFederici et al. [67]USANANANANANAHannon et al. [68]UK5Range: 23–30Female: 100%100% White-CaucasianSocio-economic status is reflected by the Cairstairs Index, used to describe levels of deprivation in the Scottish population (Carstairs & Morris, 1991). This generates five categories ranging from 1 (most deprived) to 5 (least deprived). Two participants were in category 2, two in category 3 and one in category 5Johnston et al. [57]USA51M(SD) = 14.8 (1.5)Range: 12–17.5Female: 100%NRNRKim [58]USA36M(SD) = 14.57 (1.93)Range: 12–19Female: 94.4% (n = 34)Male: 5.6% (n = 2)91.7% White (n = 33)5.5 Asian (n = 2)2.8% Other (n = 1)NRKomarova [59]UK5 cliniciansNANANANAKuang et al. [60]UK32M (SD) = 13.6 (0.3)Range: 11–17Female: 90.6% (n = 29)Male: 9.4% (n = 3)50% White (n = 16)34.4% Asian/Asian British (n = 11)9.4% Mixed (n = 3)6.3% Other (n = 2)Average household income by local area£26 k-31 k: 18.8% (n = 6)£31 k-36 k: 37.5% (n = 12)£36 k-43 k: 31.3% (n = 10)£43 k-67 k: 12.5% (n = 4)Lammers et al. [71]Netherlands431M(SD) = 36.38 (9.35)Range: 18–60Female: 92.6% (n = 399)Male: 7.4% (n = 32)NRNRLammers et al. [70]Netherlands(i) CBT + : 33(ii) DBT-BED: 41M(SD) = 37.3 (11.8)Range: 18–67Female: 89.2% (n = 66)Male: 10.8% (n = 8)NRNRLammers et al. [69]Netherlands(i) CBT + : 133(ii) DBT-BED: 42(i) CBT + : M(SD) = 33.46 (10.75)(ii) DBT-BED: M(SD) = 39.40 (10.22)(i) CBT + Female: 88.7%(ii) DBT-BED Female: 90.5%NRNRLevinson et al. [72]USA(i) In-person: 60(ii) Telehealth: 33(i) In-person: M(SD) = 25.07 (7.88)(ii) Telehealth: M(SD) = 24.52 (9.27)(i) In-person: Female: 91.67% (n = 55)(ii) Telehealth: Female: 90.91% (n = 30)(i) In-person98.33% White1.67% Black(ii) Telehealth90.91% White3.03% Black3.03% Asian3.03% Multiracial/biracialNRLowe et al. [83]USANARange: 14–55Female: 100%NRNRLui [73]USA135Female: 100%Latina AmericanNRMacDonald et al. [75]Canada(i) IOP Group: 103(ii) Individual CBT: 118(i) IOP group: M(SD) = 28.4 (9.2)(ii) Individual CBT: M(SD) = 28.6 (8.6)(i) IOP GroupFemale: 97.1%Male: 1.9%Transgender Individuals: 1.0%(ii) Individual CBT GroupFemale: 94.1%Male: 5.9%(i) IOP Group85.4% White Caucasian2.9% African-Canadian/Black4.9% Asian1.0% Latinx2.9% Mixed2.9% Other(ii) Individual CBT Group76.4% White2.7% African-Canadian/Black5.5% Asian0.0% Latino/a6.4% Mixed 9.1% OtherNRMacDonald et al. [74]Canada(i) IPT + IOP: 9(ii) IPT + individual therapy: 6(iii) IOP alone: 3(iii) Individual therapy alone: 12M (SD) = 26.0 (6.9)Range: 17- 48Cisgender Female: 61.9% (n = 26)Cisgender Male: 21.4% (n = 9)Transgender/non-binary/other gender identity: 16.7% (n = 7)White: 65.9% (n = 27)Asian: 7.3% (n = 3)Indigenous: 4.9% (n = 2)Black, middle eastern or other: 17.1 (n = 7)Biracial/multiracial: 4.9% (n = 2)Financial support (n = 39)Self-supporting 23.1% 9Partially self-supporting 33.3% 13Completely dependent (on partner, family, or government) 43.6% 17Educational attainment (n = 41)Below high school 22.0% 9High school 41.5% 17College diploma 14.6% 6Undergraduate degree 14.6% 6Professional or graduate degree 7.3% 3Monk [61]USA137M(SD) = 14.8 (1.83)Range: 10–19Female: 89.1% (n = 122)Male: 10.9% (n = 15)88.3% White-Caucasian1.5% Caucasian + Latino0.7% Caucasian + African American2.2% Latino2.2% Asian0.7% African American3.6% OtherMedian annual household income ranged from 180,607, with a mean of undefined50,000, 35.3% between 80,000–100,000, 11.8% between $100,000–150,000 and 14.7% > 150,000Wolfe et al. [87]USA38NRNRNRNRThe wordings used in the table are directly taken from the included sourcesBED: binge eating disorder; CBT: cognitive behavioral therapy; DBT: dialectical behavior therapy; HBT: home-based treatment; IOP: intensive outpatient program; IPT: inpatient treatment; M (SD): mean (standard deviation); NA: not available; NR: not reported; PHP: partial hospitalization program; TF: tube feeding; UK: United Kingdom; USA: United States of America
The methodologies and designs were diverse (Table 2). Out of the 46 sources included, nine did not present any outcome data due to being protocol papers (n = 4), service descriptions (n = 3), or descriptive reports (n = 2). Among the remaining 37 studies, the majority employed quantitative methods (n = 28), with study designs primarily consisting of pilot studies, naturalistic studies and case reports/series. Most (n = 28) included patient data only. A few incorporated perspectives from both patients and family/caregivers (n = 5) or patients and healthcare professionals (n = 1), while one study included all three groups. Additionally, one study focused solely on healthcare professionals, and another on mothers’ experiences. Sample sizes varied widely, ranging from 3 to 118 in HBT studies and 1 to 431 in ICT studies.Table 2. Overview of study designs, settings, and levels of evidenceAuthor(s)SettingStudy designData typeLevels of evidence for effectivenessLevels of evidence for meaningfulnessLevels of evidence for economic evaluationBesse-Flütsch et al. [42]HBTRCT (protocol)QuantitativeNANANABezance and Holliday [43]HBTNaturalistic study (retrospective)QualitativeNA3NABlalock et al. [82]ICTNaturalistic pilot feasibility studyQuantitative3eNANAChiumiento 2016 [55]ICTSecondary analyses of archival dataQuantitative4bNANAClark-Stone et al. [44]HBTService evaluationMixed3e3NACrenshaw [65]ICTNaturalistic Study (retrospective)QualitativeNA3NADahmen et al. [46]HBTRCT (protocol)QuantitativeNANANADaniel et al. [64]HBTOpen prospective studyQuantitative3cNANADeumens et al. [66]ICTNaturalistic studyQuantitative3eNANADoyle et al. [56]ICTSecondary analyses of archival dataQuantitative3cNANAFederici et al. [67]ICTService descriptionNANANANAFlütsch et al. [45]HBTCase series/pilot studyQuantitative3dNANAGoldschmidt et al. [48]HBTPilot study (protocol)MixedNANANAGoldschmidt et al. [47]HBTService development/descriptionDescriptive4dNANAHannon et al. [68]ICTNaturalistic StudyQualitativeNA3NAHeider et al. [49]HBTSingle-centre, non-randomised, open-label pilot studyQuantitative3eNANAHerpertz-Dahlmann et al. [50]HBTSingle-centre, non-randomised, open-label pilot studyQuantitative3eNA6Johnston et al. [57]ICTNaturalistic pilot studyQuantitative3eNANAKim [58]ICTSecondary analyses of archival dataQuantitative3eNANAKomarova [59]ICTService evaluationQualitativeNA3NAKuang et al. [60]ICTService evaluationQuantitative3eNANALammers et al. [71]ICTNaturalistic studyQuantitative3eNANALammers et al. [70]ICTOpen, quasi-randomized, controlled trialQuantitative1dNANALammers et al. [69]ICTOpen, quasi-randomized, controlled trialQuantitative2cNANALatzer et al. [51]HBTCase seriesDescriptive4dNANALevinson et al. [72]ICTNonrandomized control trialQuantitative2dNANALowe et al. [83]ICTService descriptionNANANANALui [73]ICTCase studyQuantitative4dNANAMacDonald et al. [75]ICTSequential cohort studyQuantitative2dNANAMacDonald et al. [74]ICTRetrospectiveQuantitative3cNANAMayr et al. [52]HBTNon‐randomized pilot studyQuantitative2cNA6Monk [61]ICTSecondary analyses of archival dataQuantitative4bNANAMorón-Nozaleda et al. [53]HBTRetrospective feasibility studyQuantitative3e36Munro et al. [77]ICTService descriptionMixed4b36Munro et al. [76]ICTNaturalistic studyQuantitative3eNANANovack et al. [62]ICTNaturalistic study (protocol)QuantitativeNANANAPauli et al. [54]HBTWaiting list control design pilot studyQuantitative2cNANARienecke et al. [84]ICTNaturalistic studyQuantitative4bNANARodríguez Guarin et al. [85]ICTCross-sectional descriptive observational studyQualitativeNA3NASaeidi et al. [78]ICTService evaluationMixed4c36Tsiaka and Bletsos [81]HBTService descriptionNANANANAVan Huysse et al. [63]ICTNaturalistic cohort studyQuantitative2dNA6Vroling et al. [79]ICTNaturalistic cohort study (secondary analysis)Quantitative4bNANAWalker et al. [86]ICTNaturalistic studyQuantitative3eNANAWilkes [80]ICTNaturalistic feasibility studyQuantitative3eNANAWolfe et al. [87]ICTSecondary analyses of dataQualitativeNA3NAICT: intensive community treatment; HBT: home based treatment; NA: not applicable: RCT: randomized controlled trialEvidence levels are based on the JBI Levels of Evidence. For effectiveness, Level 1 includes experimental designs (e.g., 1a: high-quality RCTs or systematic reviews), Level 2 quasi-experimental designs, Level 3 observational-analytic designs, Level 4 observational-descriptive studies, and Level 5 expert opinion and bench research. Sublevels (e.g., 1a, 2c) indicate further differentiation within a category based on study design or quality. For meaningfulness, levels range from 1 (highest) to 5 (lowest), and for economic evaluations, from 1 (highest) to 7 (lowest)
Conceptualization and implementation of the treatment programs
Details of the programs are presented in Table 3.Table 3. Overview of treatment programsTreatment programs and author(s)Treated populationAdmission criteriaUnderlying treatment model(s)Meal support/supervised mealLength and intensityDelivery modeProfessional(s) delivering the interventionCareer/family involvementPrograms for children and adolescentsHome-based treatments Department of Child and Adolescent Psychiatry, University of Zürich [Zürich, Switzerland] Flütsch et al. [45], Pauli et al. [54], Besse-Flütsch et al. [42], Mayr et al. [52]AdolescentsAN and AN atypicalFlütsch et al. [45], Pauli et al. [54], Mayr et al. 2024: Symptoms consistent with ICD-10 AN or atypical ANBesse-Flütsch et al. [42]: (1) Living with at least one adult caregiver(2) Willingness and ability to engage in family therapy(3) Being medically stable for outpatient treatment, as determined by a physician(4) Lack of comorbidities that contraindicate psychotherapy (e.g., psychosis)(5) An IQ greater than 75 (as determined by testing/clinical impression by a professional)(6) Adequate German language skill(7) Residency within the Canton of Zurich(i) HBT + FBT(ii) FBT only(iii) FBT-MBSR (Besse-Flütsch et al. [42] only)Yes (e.g., food preparation, serving, avoidance of discussion about portions)(i) HBT + FBT: 1–4 × 60 min sessions per week + additional regular outpatient treatment(ii) FBT only: 1 × 60 min per week(iii) MBSR: 2 × 30-min per week (Besse-Flütsch et al. [42] only)A period of 12 weeksIn person & familyFlütsch et al. [45];Pauli et al. [54], Mayr et al. 2024: Nurses (specialized in adolescent clinical healthcare) supervised by FBT ED clinicianBesse-Flütsch et al. [42]: Graduate nurses or social workers with graduate professional degrees and experience in treatment of adolescent EDsYes (vital)To provide advice on overcoming key issues between the patient and parents, especially during mealtimes (e.g., food preparation, serving, and avoiding discussions about portions)To support refeeding efforts and foster family resilience in everyday social activities like hobbies and friendships North Buckinghamshire Child and Adolescent Mental Health Service [Aylesbury, UK] Bezance and Holliday [43]AdolescentsAN & AN atypical(1) Adolescent must have been referred from CAMHS to HBT(2) Adolescent had a primary diagnosis of AN or EDNOS-ANFBTYes (supervision of meals at home)3–5 contacts per week of around 60 minApproximately 8 weeks (varied from 2 to 12 weeks)In person & family + additional individual supportA multidisciplinary team consisting of psychiatric nurses, occupational therapists, and clinical psychologists with psychiatry inputYes (vital)To equip parents with the skills to support mealtimes at home, including supervision and practical supportTo provide emotional support to parents, helping them restore their resources and regain control Child and Adolescent Home Treatment Team [Gloucestershire, UK] Clark-Stone et al. [44]Children and adolescentsAny EDs(1) Young people under the age of 18 with severe EDs who are at risk of being admitted to a specialist inpatient unit, or who are returning home from hospital OR Parents are struggling to implement key principles of FBT(2) Young person does not attend school(3) Start of FBT at least a few weeks before referral to HBTFBT + CRT + motivational exercisesYes (modelling & supporting meals at home)Starting with 10 home visits spread over 5 days a week and gradually reducingA period of 6 weeksIn person & familyNurse/clinicianYes (vital)To model how to support the young person during meal and snack times, showing parents how to manage their child’s eating and weight gainTo guide parents on being empathetic yet firm, challenging disordered behaviors, and maintaining motivation during meals [Pittsburgh -Pennsylvania; Providence & Pawtucket, Rhode Island, USA] Goldschmidt et al. [48], Goldschmidt et al. [47]AdolescentsAN & AN atypicalStudy inclusion criteria:(1) Eligible for home-based treatment in a community-based clinic(2) Living with at least one adult caregiver who is willing and able to engage in family treatment(3) Medically stable for outpatient treatment per physician assessment(4) Free of comorbid conditions contraindicating psychotherapy or affecting weight or appetite(5) Not pregnant or lactating(i) Manualized FBT + distress tolerance and emotion regulation skills(ii) TAU (supportive family therapy approach including psychoeducation and elements of CBT + DBT)Yes (clinician assistance preparing and supervising meals with the adolescent meal planning, and grocery shopping)(i) Manualized FBT: 3–6 h of weekly care, over 10–16 weeks(ii) TAU: 1–2 h sessions occurring at least 2 × per weekAcross Rhode Island and Pittsburgh sites: 3–6 h of therapy per week. In Rhode Island sites, treatment is generally 6–12 weeks, and in Pittsburgh families are eligible for up to 32 weeksIn person & familyClinicians—not specifiedYes (vital)To model meal planning, preparation, and supervision, empowering caregivers in their refeeding efforts Department of Child and Adolescent Psychiatry, Psychosomatics and Psychotherapy of the RWTH Aachen [Aachen, Germany] Herpertz-Dahlmann et al. [50], Heider et al. [49], Dahmen et al. [46]AdolescentsAN & AN atypical(1) A diagnosis of AN or atypical AN according to DSM-5(2) Age ≥ 12 years and ≤ 18 years(3) First or second admission for AN(4) Living with at least one carer within a commute of 60 min(5) Informed consent/assent of carers and patientsCBT + FBTInitial IPT: YesHerpertz-Dahlmann et al. 2020 & Heider et al. 2021HBT: NRDahmen et al. 2024: HBT: nutritional therapyDuring the first two months, 3–4 × visits per week, over the third and 4th month 1–2 × visit per week, including a weekly AN-focused group psychotherapy session and family sessionHBT: A period of 4 months with an average duration of M (SD) = 15.5 (1.2) weeksInitial IP admission—minimum of 4 weeks*In person & family + group + individualA multidisciplinary team of an experienced nurse, a nutritional therapist, an occupational therapist and their individual therapist (psychotherapist or child and adolescent psychiatrist)Yes (vital)To support parental management of food intake and eating disorder symptoms, facilitating weight gain Mayanei HaYeshua Medical Center [Bnei Brak, Israel] Latzer et al. [51]AdolescentsANNRPsychodynamic Psychotherapy + CBTYesA weekly online meeting of the entire team staff with the patient and parents; daily monitoring to track pharmacotherapy, physiological and emotional condition, everyday functioning, and emerging difficulties; twice-weekly nutritional counselling; twice-weekly individual psychotherapy and once-weekly family therapy or parental guidance; a once-weekly psychiatric evaluation; group treatment; daily schooling by the educational staff for adolescent patients and continued rehabilitative care for young -adult patients by the occupational therapist and the social workerLength not reportedVirtual & individual + familyA child and adolescent psychiatrist, an adult psychiatrist, a pediatrician, psychotherapists, nursing staff, clinical nutritionists, school staff, occupational therapists, spiritual therapists and support staff for the supervision of eatingYes (vital) Hospital Infantil Universitario Niño Jesús [Madrid, Spain]Morón-Nozaleda et al. [53]AdolescentsAny EDsInclusion criteria:* (1) Diagnosis of an ED according to DSM-5 in patients who met severity criteria indicating hospitalization(2) Patient commitment to follow the program instructions(3) 24/7 availability for home care by at least one caregiver(4) A commute of ≤ 30 min from home to hospital(5) Acceptance to participate by the patient and legal guardiansCBT + FBTYes (supervised meals directly in the home)Daily home visits from Monday to Friday approximately 30–60 min + 2 programmed calls per dayMean stay of 39.14 days (SD = 14.47)In person & family + groupA multidisciplinary team of experts in ED, including a child and adolescent psychiatrist, clinical psychologist, nursing team, and pediatriciansYes (vital)To provide psychoeducation, reinforcing the parental role and offering written instructions on meal planning, rest, and supervisionTo train parents in communication techniques and problem-solving strategies to help reduce anxiety Community-based treatments The Walden Adolescent Intensive Outpatient Program [MA, USA] Chiumiento [55], Doyle [56], Johston et al. [57], Kim [58], Monk [61]AdolescentsAny EDs(1) Aged between 12 and 17 years(2) Be medically stable(3) Have at least one parent able to commit to program attendanceFBT (Maudsley Approach) + CBT + DBTYes (supervised Multifamily dinner)3 × 3-h group therapy sessions per weekA period of 8 weeks, or 24-day periodIn person & group + familyClinicians—not specifiedYes (vital)To focus family sessions on enabling parents to take control of their child’s food intake, providing nutritional guidance and coaching during meal preparationTo teach parents core DBT concepts and skills, focusing on family dynamics and communication Eating Disorder Intensive Pathway—East London Foundation Trust [London, UK] Komarova [59]; Kuang et al. [60]Children and adolescentsAny EDsAdmission criteria for patients: (1) Aged under 18 years(2) Diagnosed with an ED(3) Live and have a GP within the three boroughs that EDIP operates across(4) Lack of progress in the current ED treatment and/or high risk of requiring admission to specialist eating disorder units(5) 'In-reach' to facilitate earlier dischargeStudy inclusion criteria for clinicians: (1) Healthcare professionals who work directly with patients in the EDIPFT-ED (Maudsley Approach) + distress tolerance + CBTMainly IOP but may also include HT and outreachYesAn average of 5 h per week; a maximum of 24 contacts per weekA period of 6 to 8 weeksIn-person ± virtual ± hybridPediatric and mental health nurses, pediatricians, psychiatrists, psychologists, support workers and dietitiansYes (vital) Intensive Ambulatory Care Program [Quebec, Canada] Novack et al. [62]AdolescentsAny EDsStudy eligibility: (1) Aged between 12 and 18 years(2) Have a diagnosed ED according to the DSM-5(3) Have received medical treatment in the hospital or ambulatory setting at the specialized ED clinic(4) Must be available to participate in all aspects of the proposed interventionFBT + CBT + DBT + motivational and psychoeducational approachesYes3 to 4-h sessions per weekA period of 6 to 8 weeksHybrid (web-based and in-person) & individual + groupDoctors, psychologists, social workers, etcYes (vital)To invite parents to participate in interventions addressing physical and psychological aspects of the disorder, including meal accompaniment, stress management, and family lifeTo offer meetings both in-person and online for parental support Michigan Medicine Comprehensive Eating Disorders Program[Michigan, USA] Van Huysse et al. [63]AdolescentsAny EDs(1) Moderate to severe ED symptoms + functional impairment(2) Caregiver available to participate in treatment(3) Have had an unsuccessful trial of outpatient treatment and/or an acuity suggesting that outpatient is unsafe or unsuccessful, and/or unable to access appropriate outpatient treatmentFBT (primary) + CBT + DBTYes (only in PHP)(i) PHP: 6 h per day for 5 days a weekCalendar days from treatment initiation to discharge: 38.67 days (17.19)(ii) vIOP: 3 × 3 h virtual group session + 1 day per week attend medical and psychiatric appointments per weekCalendar days from treatment initiation to discharge: 50.83 (13.83)(i) PHP: In person & group + family(ii) vIOP: Virtual & group + familyNRYes (vital)To provide twice-weekly psychoeducational support groups focused on enhancing parental self-efficacyPrograms for adultsHome-based treatments Eating Disorder and Nutrition Unit, CHU Le Bocage [Dijon, France] Daniel et al. [64]Adults BN(1) 5 BP episodes/week(2) BN duration > 2 years(3) Poor improvement (< 20% decrease in BP frequency) despite 3-month psychotherapy and/or use of antidepressant drug(i) Tube feeding(ii) Tube feeding + CBTNoA period of 3 months (mean duration of home-TF was 2.83 ± 2.28 months)In person (nasogastric tube)NRNRCommunity-Based Treatments Ladder to the Moon Program [Atlanta-Georgia, USA] Crenshaw [65]AdultsAny EDsStudy inclusion criteria: (1) Women 18 years old or older(2) Diagnosis of AN or BN according to the DSM-IV(3) Completion of the intensive outpatient program for EDs at Ladder to the Moon(4) Not currently a psychotherapy patient of the researcherFeminist ConsciousnessNo3 × 3-h group therapy sessions per weekA period of 3 weeks to 6 months with the average length of stay being 2 to 3 monthsIn person & groupNRNR Amarum Expertise Centre for Eating Disorders [Netherlands] Deumens et al. [66], Lammers et al. [71], Vroling et al. [79], Lammers et al. [70], Lammers et al. [69]Adults BEDDeumens et al. [66]; Lammers et al. [71]; Vroling et al. 2016: NRLammers et al. [70]—Study inclusion criteria:(1) Patients with a BMI ≥ 30(2) An above average urge to eat in response to negative emotions (score ≥ 2.38 on the DEBQ subscale Emotional Eating)Lammers et al. [69]—Study inclusion criteria: (1) Individuals with BED (DSM-5) or with subthreshold BED (those with BED of low frequency and those with subjective binge eating episodes)(i) CBT + psychomotor therapy(ii) DBT-BED (only in Lammers et al. [70]; Lammers et al. [69])No(i) CBT + : 1-day group intervention per week containing 3 blocks (each 75 min)(ii) DBT-BED: 20 × 2-h group-sessions (only in Lammers et al. 2020; Lammers et al. 2022)A period of 20 weeksIn person & group(i) CBT + : A psychologist, a psychiatric nurse and a psychomotor therapist(ii) DBT-BED: Trained psychologists/psychotherapists (only in Lammers et al. 2020; Lammers et al. 2022)Yes (additional in CBT +)To offer six group meetings (90 min each) for patients and their partners, aimed at enhancing mutual understanding and support during the process of change Anorexia Nervosa Intensive Treatment Team (ANITT) [Lothian region, UK] Munro et al. [77]; Hannon et al. [68]; Munro et al. [76]Adults AN(1) BMI < 13 kg/m2 OR > 15 kg/m2 and losing weight (more than 1 kg per week)Schema TherapyYesContact varies from 2 to 10 contacts a week, depending on progress and the stage of treatmentA period of 18 months with 6 month period of reduced-intensity treatment (progress reviews)In-person & individualConsultant psychiatrist in psychotherapy, consultant clinical psychologist, clinical psychologists, clinical associate in applied psychology, dieticians, nurse, assistant psychologistsNR Behavioral Wellness Clinic/Louisville Center for Eating Disorders [Louisville, KY, USA] Levinson et al. [72]Adults any EDs(1) A diagnosis of an ED(2) Medical stability (determined via a medical provider)(3) BMI > 16.5(4) Need for more intense care than outpatient aloneCBT-E + FBT + Exposure therapy + DBTYes3 h daily for 5 days per weekLengh of stay (weeks)(i) Telehealth: M(SD) = 11.07 (6.3)(ii) In-person: M(SD) = 12 (8.03)(i) In person group + individual(ii) Virtual group + individualTherapist, dietitian, and prescriberNR Lui [73][USA]Adult BN, alcohol and cocaine use disorders, and bipolar I disorderNRindividual: integrative cognitive affective therapy group: narrative therapy + ACT + DBTYes15 × 1 h individual therapy + 3 × 3 h group therapy sessions per weekLength NRIn person & individual + groupTherapist, dietician, psychiatristNR Centre for Mental Health, University Health Network [Toronto, Canada] MacDonald et al. [75]AdultsAny EDsStudy inclusion criteria: (1) Had pre-IPT/DPT symptoms meeting criteria for DSM-5 diagnoses of: AN-R; AN-BP; BN; or PD(2) Achieved partial remission or better following IPT/DPT(3) Participated in ≥ 4 weeks of maintenance treatment(4) Participated in follow-up assessment at 6 and/or 12-months after IPT/ DPTCBTYes(i) IOP Group: 6 to 14 h per week up to 16 weeks(ii) Individual CBT: 16 sessions over 14 weeks(i) In person & group(ii) In person & individualNRNR Centre for Mental Health, University Health Network [Toronto, Canada] MacDonald et al. [74]Adults ARFIDEligible participants: (1) Had a DSM-5 diagnosis of ARFID(2) Started treatment at the University Health Network’s Eating Disorder Program between April 2020 and March 2023CBT-AR + CBT + DBTYesCBT-AR: 2 × per week for the first 16 sessions and 1 × per week for the final 4 sessionsGroup: one clinician-supported meal and one psychotherapy group per day, from Monday to FridayA period of 12 weeksIn person & individual + groupA multidisciplinary care team (i.e., psychologists, psychiatrists, nurse practitioners and nurses, social workers, registered dietitians, occupational therapists, and registered psychotherapists)NR Yorkshire Centre for Eating Disorders [Leeds, UK] Saeidi et al. [78]Adults ANStudy inclusion criteria—participants had to meet at least two of the following:(1) DSM-IV diagnostic criteria for AN for minimum of four years(2) BMI of 12 and above(3) Several admissions to specialist EDs services(4) Lack of response to long-term individual or group therapy(5) Aged 18 years and aboveNRNR2 to 7.5 h per week, up to five visits per weekLength NRIn-person, telephone or textHealth support workers, dietitian, consultant psychiatrist, nurseNR Bright Heart Health[23 states in USA] Wilkes [80]Adults Any EDsStudy inclusion(1) Willingness to provide demographic and insurance information(2) Willingness to complete various assessment(3) Commitment to pay for services and participate(4) Access to internet(5) Ongoing medical assessments with consent to release information to treatment teamCBT + DBT + experiential therapy somatic therapyYes (where patients eat a meal online once a week and psychoeducation on meal planning and nutrition)11-h per weekAverage period of 10 weeksVirtual & individual + groupMarriage and family therapists, clinical social workers, psychologists, dieticians, and a psychiatristYesTo provide family sessions and support groups, equipping family members with the tools to support their loved ones during treatment Cleveland Center for Eating Disorders [Cleveland—Ohio, USA] Federici et al. [67]Adults Any EDs(1) Experienced repeated treatment failures from standard day treatment, residential, and/or inpatient settings OR participated in standard EDs programming for a minimum of 28 days without a decrease in symptoms(2) One or more of the following criteria: (i) Presenting as Mult diagnostic, as evidenced by an additional co-occurring Axis I disorder/s and/or Axis II disorder/s(ii) Struggle with pervasive emotion regulation deficits that commonly lead to symptoms, as evidenced by an inability to adaptively regulate, communicate, or tolerate affect(iii) Historically have been unable to generalize skills outside of standard treatment, as evidenced by relapse in symptoms posttreatment or during treatment(iv) Present with considerable therapy-interfering behavior(s) such that they cannot remain in standard treatment for eating disorders without significant adverse consequences to the therapy milieuDBT + CBT componentsYes (meal planning)DPT: 6 h per day for 5 days/week or IOP: 3 h per day for 3–5 days/weekA period of 6 monthsIn person & individual + groupDBT therapist, nutritionists and psychiatristsNRPrograms for all ageHome-based treatments Hellenic Center for Eating Disorders [Nea Kifisia, Greece] Tsiaka and Bletsos [81]Adolescents and adults AN(1) 13 + years old(2) Low weight, need for refeeding and meal support BMI < 15BMI > 15 medically stable or with unstable biochemistry(3) Meet the diagnostic criteria for severe or enduring AN and related conditions(4) Prescribed specialist treatment recommended to reduce risk of relapse and move to discharge from medical servicesMANTRA + Cognitive Interpersonal Maintenance ModelYes (providing a model for healthy eating, meal plan, cooking sessions)4–6 h per day for everydayA period of 18 weeksIn person & familyMedical Doctors: Pathologist, Cardiologist, Endocrinologist, PediatricianTreatment Team: Psychiatrist, psychologists, family therapists, nutritionist/dietician, occupational therapist, psychiatric nurseYes (vital)To provide staff-supported family mealsTo provide family therapyCommunity-based treatments Eating Recovery Center [USA] Blalock et al. [82]; Rienecke et al. [84]Children, adolescents and adultsAny EDsBlalock et al. [82]: (1) Qualify for IOP level of care(2) Have insurance (patients were not charged for VIOP, but were required to have insurance in case a step up to higher level of care was needed)(3) Have a reliable internet connection at home as well as access to a computer, web camera, and headphones(4) Receive medical clearance from an in-person local medical providerRienecke et al. [84]: NRDBT + CBT + ACTFor C&A service: + EFFTYes (meal support group -feedback over video from therapists or dietitians on portions and nutrition + eating meals together with therapists or dietitians and peers)3 × 3-h group therapy sessions weekly, 1 h of individual or family therapy weekly, one biweekly appointment with a registered dietitianBlalock et al. [82]: A biweekly in-person meeting with the patient's local medical providerRienecke et al. [84]: Medical monitoring collected by remote medical devicesBlalock et al. [82]: A period of 6 weeks with an average of M (SD) = 5.85 (1.72) weeksRienecke et al. [84]: The average number of days treatment for adults was 62.41 days (SD = 29.90) and for children/adolescents was 79.48 days (SD = 37.04)Blalock et al. [82]: In person & virtual & group + individual or familyRienecke et al. [84]: Virtual & group + individual or familyA licensed psychotherapist, a registered dietitian and a consulting psychiatrist (on-hand for support)YesTo replace individual therapy with family therapy when clinically indicated, focusing on meal planning and problem-solvingTo offer optional emotion-focused family therapy EFFT training sessions for parents or guardians Rodríguez Guarin et al. [85]Adolescents and adults Any EDsAbsence of medical or psychiatric life-threatening riskCBT + Psychodynamic psychotherapy + DBT + Expressive therapy + Art therapyYes (nutritional rehabilitation, daily therapeutic meals) ~ 19 h per week (2 individual sessions + 1 Psychiatry follow-up session + 2 daily group sessions + 1 weekly nutrition workshop + multi-family and single-family support sessions)Length not clear – at least 8 weeksVirtual & individual + groupPsychiatrists, psychologists and two healthcare professionals working in nutritionYesTo train and to support parents and caregivers (e.g., modelling for how to proceed at mealtimes)[Northeastern USA] Walker et al. [86]Adolescents and adultsAny EDsNRCBT-E + DBTYes4-h per day, 3 days per week from 2013 to 2015 and up to 4 days per week from 2015 to 2017Average of 15.82 (SD = 13.38) weeksIn person & groupA licensed masters or doctoral level clinician or by a graduate student under the direct supervision of a licensed clinician (not specified)NR The Renfrew Center [USA] Lowe et al. [83]Adolescents and adultsAny EDsNRCBTYes3 × 3 h per weekLength NRIn person & individual + groupCase manager, registered dietitian, psychiatrist, master's level clinicians—not specified)Yes (optional) family therapy—details not specified Within Health [USA] Wolfe et al. [87]Adolescents and adultsAny EDsNRIntegrative treatment model: ACT, CBT, DBT, interpersonal with experiential modalities (e.g., art therapy, movement) (indicated based on patient presentation)Yes (meal support group + meal planning check-ins + nutrition counseling)At least 3 h per day; 3–5 days per weekLength NRVirtual & individual + groupA multidisciplinary team of professionals, including a psychotherapist, registered dietitian, registered nurse, psychiatric provider, and clinical support staff (e.g., care partner, food specialist)Yes (where indicated)To address couples/family-related issues including increasing understanding of EDs, working on communication, and cultivating supportive relationshipsACT: acceptance and commitment therapy; AN: anorexia nervosa; AN-BP: anorexia nervosa, binge-purge type; AN-R: anorexia nervosa, restricting type; ARFID: avoidant/restrictive food intake disorder; BED: binge eating disorder; BMI: body mass index; BN: bulimia nervosa; CAMHS: Child and adolescent mental health services; C&A: children and adolescents; CBT: cognitive behavioral therapy; CBT-AR: cognitive-behavioral therapy for avoidant/restrictive food intake; CBT-E: enhanced cognitive behavioral therapy; CRT: cognitive remediation therapy; DBT: dialectical behavior therapy; DEBQ: Dutch eating behavior questionnaire; DPT: day patient treatment; DSM: Diagnostic and Statistical Manual of Mental Disorders; ED: eating disorders; EDNOS: eating disorder not otherwise specified; EDIP: Eating Disorder Intensive Pathway; EFFT: emotion-focused family therapy; FBT: family based treatment; FT-ED: family therapy for eating disorders; HT: home treatment; ICD: International Classification of Diseases; IOP: intensive outpatient program; IPT: inpatient treatment; MANTRA: Maudsley anorexia nervosa treatment for adults; MBSR: mindfulness-based stress reduction; M (SD): mean(standard deviation); NR: not reported; PHP: partial hospitalization; TAU: treatment as usual; UK: United Kingdom; USA: United States of America; VIOP: virtual intensive outpatient program
Programs for children and adolescents
Home-based treatments
Seven HBT programs for children and adolescents were identified which were presented in 13 distinct papers [15, 42–54]. These HBT programs were predominantly designed to treat AN and atypical AN, except two providing treatment/care for any type of ED [44, 53]. Family-Based Treatment (FBT) was the most common psychotherapeutic approach, either as a stand-alone treatment or combined with Cognitive Behavior Therapy (CBT). In all HBT programs, family/carer involvement was reported as a vital part of treatment, mainly focusing on providing psychoeducation about EDs and guidance on managing eating behaviors and stress. Furthermore, these programs provided meal support and/or supervised meals, except one program [49, 50] that offered supervised meals during the initial inpatient admission period, but for which the provision of such support during the home treatment phase was not clearly indicated.
All treatments were designed to include visits to patients’ homes, yet one case study described virtual treatment due to the COVID-19 pandemic [51]. While the treatments were delivered by multidisciplinary teams in most of the HBT programs, two programs used nurses as the main healthcare professionals delivering the treatment [44, 45, 52, 54].
The duration and intensity of HBT programs appeared to vary, mostly depending on clinical severity and healthcare systems. The minimum duration was six weeks [44] and the maximum duration was reported as 16 weeks with an option to go up to 32 weeks based on available insurance coverage [47, 48]. Contact intensity varied significantly across different programs with the most intensive ones providing daily home visits (Monday–Friday) of 30–60 min each [53] or up to 10 home visits per week (Monday- to Friday; [44]. The least intensive treatment included one to four sessions per week each lasting for approximately 60 min, with an average of 1.8 sessions [45, 52, 54].
Information on HBT admission criteria was not always clearly presented. Several papers listed “inclusion criteria” for the research component instead of precisely outlining admission criteria for HBT programs. Among the specified eligibility and/or inclusion criteria, availability of a caregiver for involvement in treatment and distance to the hospital (e.g., less than 30 min commute from home to hospital) were common requirements.
Intensive community treatments
Four ICT programs for children and adolescents were identified, which were presented in nine papers [55–63]. These offered care for any type of ED. However, one of these programs, also offered HBT-support and outreach when deemed necessary [59, 60]. Treatments involved combinations of psychotherapeutic approaches such as FBT, CBT and Dialectical Behavior Therapy (DBT) as well as meal support and/or supervised meals, except for one virtual program [63] which did not offer meal support. Family/carer involvement was a vital component across the programs with a focus on providing parents with psychoeducation about EDs, guidance on managing eating behaviors and empowering them.
Of these programs, only one delivered treatment in-person [55–58, 61]. One program offered virtual treatment [63], and two had a hybrid format [59, 60, 62]. Furthermore, while two programs were delivered by multidisciplinary teams [59, 60, 62], two did not specify the healthcare professionals involved [55–58, 61, 63]. The duration of ICT programs for this age group were mostly around eight weeks, and the intensity ranged from three-four hours/week [62] to 10 h/week [63]. Other than being under 18 years old and having an ED diagnosis, there were no common eligibility or inclusion criteria.
Overall, neither the discharge criteria nor the post-treatment procedure were explicitly outlined for any of the ICT or HBT programs for children and adolescents.
Programs for adults
Home-based treatments
Only one HBT program for adults was identified: this focused on bulimia nervosa (BN) [64]. The treatment involved tube feeding delivered at home for a period of 3 months. This treatment program did not provide information regarding the involvement of professionals delivering the intervention, nor the involvement of families or caregivers.
Intensive community treatments
ICT programs for adults were more diverse, with 10 programs offering treatment presented in 16 distinctive sources [65–80]. The majority of these (n = 5) provided treatment for patients with any type of ED. Two programs offered treatment for AN only [68, 76–78], one for binge eating disorder (BED) [66, 69–71, 79], one for BN [73], and one for avoidant/restrictive food intake disorder (ARFID) [74].
ICT programs for adults primarily offered a combination of psychotherapeutic approaches, such as CBT and DBT. One program used on Schema Therapy [68, 76, 77], while another used a ‘Feminist Consciousness’ approach [65]. The majority of these programs provided meal support and/or supervised meals, except for three programs [65, 66, 69–71, 78, 79]. Only one program had family/carer involvement as a core component, providing tools to help family members support their loved one during treatment [80]. Another program offered family involvement as an additional component with the goal of improving understanding and support amongst parents and partners during the process of change [66, 69–71, 79].
These programs offered treatment in-person, except for two virtual programs [72, 80]. Multidisciplinary treatment teams commonly delivered these programs, although two programs did not report this information [31, 65]. Regarding the duration of programs, the Anorexia Nervosa Intensive Treatment Team (ANITT) in the UK was the longest with a duration of up to 18 months and an additional 6-month period of reduced-intensity treatment. This program focused on very severe and persistent AN only [68, 76, 77]. The shortest reported treatment duration was 3 weeks, with the average treatment duration typically ranging from 2 to 3 months [65].The treatment programs typically involved several hours per week, combining group and individual sessions. Contact hours ranged from three 75-min blocks of a weekly group intervention all delivered on one day [66, 69–71, 79] to 15 h per week [72].
The eligibility and/or study inclusion criteria for these treatment programs were diverse, reflecting a range of approaches and criteria. Commonly reported criteria included diagnostic aspects and specific body mass index (BMI) levels. Discharge criteria were mentioned in only one ICT program [80] as follows: no ED behaviors for two weeks and completing 90% of the meal plan at least 90% of the time.
Programs for all age populations
Home-based treatments
One was a HBT program providing care for adolescents and adults with AN [81]. This program offered The Maudsley Anorexia Nervosa Treatment for Adults (MANTRA) as its main psychotherapeutic modality combined with meal support and/or supervised meals daily over a period of 18 weeks. Family/carer involvement was seen as integral to this program, with a focus on family therapy and supporting families during mealtimes. Treatment was delivered by a multidisciplinary team.
Intensive community treatments
Five ICT programs provided treatment for any type of ED for all age populations [82–87]. These programs offered meal support and/or supervised meals. While one employed CBT as a stand-alone approach [83], others used CBT combined with other psychotherapeutic approaches such as DBT or Acceptance and Commitment Therapy (ACT) [82, 84–87]. While family/carer involvement was offered in three programs as needed [82–84, 87], itwas a main component in one program [85] and was not reported in another [86]. Four programs described the treatment team as involving professionals from various backgrounds (e.g., psychiatrist, dietitian) [82–85, 87], whereas one paper did not specify the professional roles beyond licensed clinicians or supervised graduate students [86]. The duration of treatment was not reported for two program [83, 87] and it was not clear for one (i.e., at least eight weeks; [85]), while two other programs reported an average duration of about 16 weeks [82, 84, 86]. The weekly intensity was similar across programs, ranging from nine to 19 h/week.
Admission criteria were only specified for the HBT program [81] and in one paper describing an ICT program [82]. Discharge criteria were not mentioned for any of the programs.
Efficacy, acceptability and cost-effectiveness of the treatment programs
Table 4 presents a summary of the quantitative outcomes and Table 5 provides a summary of the qualitative outcomes. To map the types of evidence and study designs, the included papers were classified according to the JBI Levels of Evidence classification system which is a hierarchical framework that ranks quality of evidence from Level 1 (strongest) to Level 5 (weakest) based on study design and methodological rigor.Table 4. Summary of quantitative outcomes: ED-related outcomes, feasibility and acceptability, and cost-effectivenessTreatment programs and author(s)NDesignDistribution of participants by diagnosisBrief treatment descriptionEDs related outcomes (e.g., BMI, symptoms)Feasibility and acceptability outcomesCost-effectiveness outcomesPrograms for children and adolescentsHome-based treatments Department of Child and Adolescent Psychiatry, University of Zürich [Zürich, Switzerland] Flütsch et al. [45]45Case Series/Pilot StudyAN: n = 31 (69%)AN atypical: n = 14 (31%)FBT at home1–4 × 1 h sessions per week + additional regular OPA period of 12 weeksBMI: A significant improvement with a large effect sizeEDE: A significant improvement with a medium effect sizeEDI-2: A significant improvement with a large effect size(1) Good treatment retention with no premature dropouts during the study period(2) Treatment was well accepted by the majority of patients and parents, rating their treatment satisfaction as good or very goodNR Department of Child and Adolescent Psychiatry, University of Zürich [Zürich, Switzerland] Pauli et al. [54]HBT + FBT: 45 FBT only: 22Waiting List Control Design Pilot StudyAN: n = 52 (77.6%)AN atypical: n = 15 (22.4%)(i) FBT only: at least 1 × 1 h per week(ii) HBT + FBT: 1–4 × 1 h sessions per week + additional regular OPA period of 12 weeksBMI: A significantly higher increase in the HT + FBT group compared to the FBT‐only group 3 months after the beginning of treatmentEDE: Both groups showed a significant improvement from pre treatment to 3 months after the beginning of treatment without a significant group differenceEDI‐2: Both groups showed a significant improvement from pre treatment to 3 months after the beginning of treatment without a significant group differenceOver‐exercising: Both groups showed a significant improvement from pre treatment to 3 months after the beginning of treatment without a significant group differenceNo patients in either group dropped out of the treatment and the study during the study periodNR Department of Child and Adolescent Psychiatry, University of Zürich [Zürich, Switzerland]Mayr et al. [52]HBT + FBT: 40 FBT only: 21AN: n = 52 (85.2%)AN atypical: 9 (14.8%)Same as Pauli et al. [54]EBW: In the HBT + FBT group 70% of patients reached > 85% of their EBW within 3 months, whereas in the FBT‐only group this was achieved by only 52% of patientsThe average cost per subject in theHBT + FBT group was 5770 SFr. (Swiss francs), nearly half thecost of 10,710 SFr. per subject in the FBT‐only groupInpatient treatment comprised 86% of the total costfaced by the FBT‐only group Child and Adolescent Home Treatment Team [Gloucestershire, UK] Clark-Stone et al. [44]33Service EvaluationAN: 87.88% (n = 29)BN: 6.06% (n = 2)OSFED: 6.06% (n = 2)FBTStarting with 10 contacts per week by gradually reducingA period of 6 weeksOf the 31 patients, 70.97% of them had an increased BMI compared to 29.03% who had BMI decreasesNRNR Department of Child and Adolescent Psychiatry, Psychosomatics and Psychotherapy of the RWTH Aachen [Aachen, Germany] Herpertz-Dahlmann et al. [50]Patients: 22Carers: 22Single-centre, non-randomized, open-label pilot studyAN: 100%AN atypical: n = 3 (13.6%)FBT + CBTStarting 3–4 × visits per week (1st and 2nd month), then 1–2 × visit per week (3rd and 4th month)A period of 4 monthsBMI: Significant improvement at the end of HT and 1-year follow-upWeight: Highest weight gain was achieved between IP admission and beginning of HT. Weight continued to increase during HT, and between the end of HT and the 1-year follow-up, weight gain was maintainedEDI-2: Significant improvement from beginning of HT to end of HT. This improvement was maintained for the 1-year follow-upBoth patients and carers reported high treatment satisfactionHT reduced cost around 25% Department of Child and Adolescent Psychiatry, Psychosomatics and Psychotherapy of the RWTH Aachen [Aachen, Germany] Heider et al. [49]21Single-centre, non-randomized, open-label pilot studyAN: n = 18 (85.7%)AN atypical: n = 3 (14.3%)FBT + CBTStarting 3–4 × visits per week (1st and 2nd month), then 1–2 × visit per week (3rd and 4th month)A period of 4 monthsSame as Herpertz-Dahlmann et al. 2020Same as Herpertz-Dahlmann et al. 2020Same as Herpertz-Dahlmann et al. 2020 Hospital Infantil Universitario Niño Jesús [Madrid, Spain] Morón-Nozaleda et al. [53]Patients: 57Carers: 43Retrospective Feasibility StudyAN (restrictive type): n = 30 (50.8%)AN atypical: n = 7 (11.8%)AN (purging type): n = 3 (5.1%)BN: n = 5 (8.5%)ARFID: n = 3 (5.1%)OSFED: n = 11 (18.6%)CBT + FBTDaily home visits from Monday to Friday approximately 30–60 min + 2 programmed calls per dayMean stay of 39.14 days (SD* = 14.47)NR(1) 91.5% of the patients complied with the complete protocol(2) The overall family satisfaction was high(3) All caregivers perceived the program as “very safe.”In its first year of operation, the program avoided a total of 2016.03 inpatient hospital stays (saving a total of 1,762,292.46 euros compared to conventional inpatient treatment)Community-Based Treatments The Walden Adolescent Intensive Outpatient Program [MA, USA] Chiumiento [55]272Secondary Analyses of Archival DataAN: n = 117 (41.2%)EDNOS: n = 155 (54.6%)BN: n = 8 (2.8%)ARFID: n = 4 (1.4%)Parent DBT SkillsGroup vs Parent Support Group vs Multi-Family Group1 × per weekA period of 8 weeks, or 24-day periodNRNo significant differences between satisfaction rating of program components (DBT parenting skills group, parent support group, MFT group)NR The Walden Adolescent Intensive Outpatient Program [MA, USA] Doyle [56]Children: 14Adolescents: 30Secondary Analyses of Archival DataAN: n = 15 (34%)EDNOS: n = 28 (64%)BN: n = 1 (2.2%)FBT(Maudsley Approach) + CBT + DBT3 × 3-h group therapy sessions per weekA period of 8 weeks, or 24-day periodBMI/IBW: Both age groups showed significant improvements from pre- to post-treatment and to 6-month follow-upEDE-Q total: Both age groups showed significant improvements from pre- to post-treatment and to 6-month follow-upNRNR The Walden Adolescent Intensive Outpatient Program [MA, USA] Johston et al. [57]51Pilot studyAN: n = 17 (33%)BN: n = 6 (12%)EDNOS: n = 28 (55%)FBT(Maudsley Approach) + CBT + DBT3 × 3-h group therapy sessions per weekA period of 8 weeks, or 24-day periodBMI: Statistically significant increase from admission to discharge, discharge to 3 month follow-up, and 6 month and 1 year follow-upsEDE-Q: Statistically significant improvement from admission to discharge, and continued to improve at 6 months and were similar at 1 year follow-upBinge–purge behaviors: Frequency decreased over the course of treatment, but not significantly(1) 36/51 patients (71%) completed the full program(2) Overall treatment attrition rate was 29%NR The Walden Adolescent Intensive Outpatient Program[MA, USA] Kim [58]36Secondary Analyses of Archival DataAN: n = 18 (50%)BN: n = 1 (2.8%)EDNOS: n = 17 (47.2%)FBT(Maudsley Approach) + CBT + DBT3 × 3-h group therapy sessions per weekA period of 8 weeks, or 24-day periodBMI/IBW: Statistically significant improvement from admission to discharge, and continued to increase at 3 months to 6-month follow-upsBinge–purge behaviors: No statistically significant differenceEDE-Q total: Statistically significant improvement from admission to discharge, and continued to improve from discharge to 1 year follow-upNRNR Eating Disorder Intensive Pathway—East London Foundation Trust [London, UK] Kuang et al. [60]32Service EvaluationAN: n = 25 (78.1%)OSFED: n = 6 (18.8%)BN: n = 1 (3.1%)FT-ED (Maudsley Approach) + distress tolerance + CBTAn average of 5 h per week; a maximum of 24 contacts per weekA period of 6 to 8 weeksW4H: Statistically significant improvement from pre- to post-treatmentCGAS: Statistically significant improvement from pre- to post-treatmentEDE-Q: No statistically significant differenceNRNR The Walden Adolescent Intensive Outpatient Program [MA, USA] Monk [61]137Secondary Analyses of Archival DataAN: n = 52 (38.2%)EDNOS: n = 82 (60.3%)BN: n = 2 (1.5%)FBT (Maudsley Approach) + CBT + DBT3 × 3-h group therapy sessions per weekA period of 8 weeks, or 24-day periodNRNRNR Michigan Medicine Comprehensive Eating Disorders Program [Michigan, USA] Van Huysse et al. [63](i) PHP: 49(ii) vIOP: 53Naturalistic Cohort Study(i) In-person PHPAN (restrictive type): n = 26 (53.1%)AN (binge-purge type): n = 4 (8.2%)BN: n = 4 (8.2%)ARFID: n = 4 (8.2%)OSFED-atypical AN: n = 11 (22.4%)OSFED-other: 0 (0%)(ii) Virtual IOPAN (restrictive type): n = 31 (58.5%)AN (binge-purge type): n = 5 (9.4%)BN: n = 1 (1.9%)ARFID: n = 1 (1.9%)OSFED-atypical AN: n = 13 (24.5%)OSFED-other: n = 2 (3.8%)FBT (primary) + CBT + DBT(i) PHP: 6 h per day for a 5 days a week (~ 32 h over 5 days weekly)Calendar days from treatment initiation to discharge: 38.67 days (17.19)(ii) vIOP: 3 × 3 h virtual group session + 1 day patients attend medical and psychiatric appointments per week (~ 13 h over 4 days weeklyCalendar days from treatment initiation to discharge: 50.83 (13.83)Expected body weight (%EBW): In both groups, patients showed significant improvements in %EBW over time, with average %EBWs suggesting that participants were at or very close to weight restored at 3- and 6-months post-treatmentNRAmount billed was 64,854 for PHPPrograms for adultsHome-based treatments Eating Disorder and Nutrition Unit, CHU Le Bocage [Dijon, France] Daniel et al. [64]118(i) Tube feeding (TF) + CBT: 61 patients(ii) Tube feeding (TF) alone: 57 patientsOpen Prospective StudyBN: 100%(i) Tube feeding(ii) Tube feeding + CBTThe frequency of binge-purge episodes was lower after treatmentThe improvement in energy and protein intake was similar in the two groupsHome-tube feeding was quoted as too hard in 12% of the patients who stopped it, very hard (very difficult) in 24% of them, hard in 35%, easy in 24% and very easy in 5% of themNRCommunity-Based Treatments Eating Recovery Center [USA] Blalock et al. [82]57Naturalistic Pilot Feasibility StudyAN: n = 21 (37%)BN: n = 21 (37%)BED: n = 9 (16%)ARFID: n = 3 (5%)OSFED: n = 3 (5%)DBT + CBT + ACT 3 × 3-h group therapy sessions weekly, 1 h of individual or family therapy weekly, one biweekly appointment with a registered dietitian and a biweekly in-person meeting with the patient's local medical providerA period of 6 weeks with an average of M (SD) = 5.85 (1.72) weeksBinging: statistically significant and clinically meaningful improvementsPurging: statistically significant and clinically meaningful improvementsRestricting: statistically significant and clinically meaningful improvements(1) All patients attended all therapy during treatment period(2) Patients strongly endorsed VIOP as a helpful experienceNR Amarum Expertise Centre for Eating Disorders [Netherlands] Deumens et al. [66]182Naturalistic StudyBED: 100%1-day group intervention per week containing 3 blocks (each 75 min)A period of 20 weeksBMI: Statistically significant improvementsEDI-II Drive for thinness: Statistically significant improvementEDI-II Interceptive awareness: Statistically significant improvementEDI-II Bulimia: Statistically significant improvementBody attitude: Statistically significant improvementNRNR Amarum Expertise Centre for Eating Disorders [Netherlands] Lammers et al. [71]431Naturalistic StudyBED: 100%1-day group intervention per week containing 3 blocks (each 75 min)A period of 20 weeksBMI: Statistically significant improvement from baseline to end of treatment (moderate effect size) and from end of treatment to 6 month follow up (weak effect size)EDI-II Bulimia: Statistically significant improvement (large effect size) from baseline to end of treatment90 patients dropped out of treatment (83 women and 7 men)NR Amarum Expertise Centre for Eating Disorders[ Netherlands] Vroling et al. [79]376Naturalistic Cohort Study (secondary analysis)BED: 100%1-day group intervention per week containing 3 blocks (each 75 min)A period of 20 weeksNR21.81% of the patients dropped out of treatmentNR Amarum Expertise Centre for Eating Disorders [Netherlands] Lammers et al. [70](i) CBT + : n = 33(ii) DBT-BED: n = 41Open, Quasi-randomized, Controlled trialBED: 100%(i) CBT + : 1-day group intervention per week containing 3 blocks (each 75 min)(ii) DBT-BED: 20 × 2-h group-sessionsA period of 20 weeksEDE-Q Global: The CBT + group experienced greater reductions that approached significance at end of treatment and reached significance at 6 month follow-upObjective binge eating episodes: The CBT + group showed greater reductions at end of treatment, but these differences were no longer significant at 6 month follow-upEmotional eating: No significant group differences7 (9.5%) participants dropped out of the treatment and/or study during the course of the trial, including 2 (6.1%) from CBT + and 5 (12.2%) from DBT-BEDNR Amarum Expertise Centre for Eating Disorders [Netherlands] Lammers et al. [69](i) CBT + : n = 133(ii) DBT-BED: n = 42Open, Quasi-randomized, Controlled trialBED: 100%(i) CBT + : 1-day group intervention per week containing 3 blocks (each 75 min)(ii) DBT-BED: 20 × 2-h group-sessionsA period of 20 weeksEDE-Q Global: Both groups showed statistically significant improvement between baseline and EOT and between baseline and follow-up, but improvement was greater in CBT + group (medium effect size) between baseline and EOTObjective binge eating episodes: Scores in both groups decreased significantly between baseline and EOT, and between baseline and 6-month follow-upEmotional eating: CBT + group (small effect size) showed statistically significant improvement between baseline and EOT28 (16.0%) participants dropped out of the treatment during the course of the trial, including 20 (15.0%) from CBT + and 8 (19.0%) from DBT-BEDNR Anorexia Nervosa Intensive Treatment Team (ANITT) [Lothian region, UK] Munro et al. [77]33Service EvaluationAN: 100%Schema Therapy2 to 10 contacts a weekA period of 18-month with 6-month period of reduced-intensity treatment (progress reviews)NR(1) The mean overall service satisfaction was 4/5(2) Patients perceived staff as supportive, caring and genuine(3) Patients valued individualised care, a holistic psychological approach based on emotional and physical needs and not just weight(4) Only 2 patients dropped out during a 2 year periodA total saving of £391,656 in a 2 year period Anorexia Nervosa Intensive Treatment Team (ANITT) [Lothian region, UK] Munro et al. [76]26Naturalistic Case SeriesAN: n = 24 (92%)Atypical AN: n = 2 (8%)Schema Therapy 2 to 10 contacts a weekA period of 18-month with 6-month period of reduced-intensity treatment (progress reviews)BMI: Increased on average by 3.9 kg/m2 from a mean of 13.0 at intake to 16.9 at the end of the study periodEAT-26: 7 patients (27%) showed statistically significant change, with five (19%) achieving change to the level of remission or recovery. 13 patients (50%) showed no statistically significant change, with nine of these showing non-significant improvement. Six patients (23%) described statistically significant deterioration75% of the sample were either ‘satisfied’ or ‘extremely satisfied’ with the treatmentNR Behavioral Wellness Clinic/Louisville Center for Eating Disorders [Louisville, KY, USA] Levinson et al. [72](i) In-person: 60 patients(ii) Telehealth: 33 patientsNonrandomized Control Trial(i) In-personAN: n = 26 (43.33%)BN: n = 6 (10.00%)OSFED: n = 22 (26.67%)BED: n = 5 (8.33%)ARFID: n = 1 (1.67%)(ii) TelehealthAN: n = 14 (42.4%)BN: n = 4 (12.12%)OSFED: n = 10 (30.03%)BED: n = 4 (12.12%)ARFID: n = 1 (3.03%)CBT-E + FBT + Exposure therapy + DBT3 h daily for 5 days per weekLength of stay (weeks)(i) Telehealth: M(SD)* = *11.07 (6.3)(ii) In-person: M(SD)* = 12 (8.03)BMI: Both groups had significant improvement at dischargeEDE-Q: Both groups had significant improvement at dischargeNRNR Lui [73][USA]1Case studyBN: 100%Individual: integrative cognitive affective therapy & group: narrative therapy + ACT + DBT15 × 1 h individual therapy + 3 × 3-h group therapy sessions per weekLength NRBMI: No changeEDE-Q: Patients scores reduced from baseline to end of treatment, and from end of treatment to 1-month follow-upEPSI: Patients scores reduced from baseline to end of treatment, and from end of treatment to 1-month follow-up for body dissatisfaction, binge eating and negative attitudes toward obesity. Patient's cognitive constraint, purging and restriction scores reduced from baseline to end of treatment. Patient's excessive exercise score increased from baseline to end of treatment, but was lower at 1-month follow up compared to baselineNRNR Centre for Mental Health, University Health Network [Toronto, Canada] MacDonald et al. [75](i) IOP Group: 103 patients (46.6%)(ii) Individual CBT: 118 patients (53.4%)Sequential Cohort Study(i) IOP Group:AN (restrictive type): 8.7%AN (binge-purge type): 9.7%BN: 63.1%PD: 18.4%(ii) Individual CBT Group: AN (restrictive type): 9.3%AN (binge-purge type): 10.2%BN: 66.9%PD: 13.6%CBT(i) IOP Group: 6 to 14 h per week up to 16 weeks(ii) Individual CBT: 16 sessions over 14 weeksBMI: AN patients in both treatment group showed an improvementED symptoms: Both groups followed very similar trajectory of return to clinically significant symptoms at 12-month follow-upNRNR Centre for Mental Health, University Health Network[Toronto, Canada] MacDonald et al. [74](i) IPT + IOP: 9 patients(ii) IPT + individual therapy: 6 patients(iii) IOP alone: 3 patients(iii) Individual therapy alone: 12 patientsRetrospective Chart ReviewARFID: 100%Initial assessment: n = 42From IP to IOP: n = 8Directly IOP: n = 3CBT-AR + CBT + DBTCBT-AR: 2 × per week for the first 16 sessions and 1 × per week for the final 4 sessionsGroup: 1 clinician-supported meal and 1 psychotherapy group every dayBMI: Patients showed improvement (only reported for those transitioned from IP to IOP)(1) Of the nine patients who transitioned from inpatient to IOP, eight (88.9%) completed IOP and one (11.1%) ended treatment early(2) Three patients (7.1% of the total sample) had a direct entry to IOP, all of whom (100%) completed treatmentNR Yorkshire Centre for Eating Disorders [Leeds, UK] Saeidi et al. [78]Patients: (n = 6)Clinical team members (n = 8)Service EvaluationAN: 100%2 to 7.5 h per week, up to five visits per weekLength NREating Disorders Quality of Life Scale: The average score for quality of life increased from 2 to 2.3, with social interaction the most improved areaPlease qualitative findings regarding treatment experiences in Table 2(1) Treatment reduced costs by 30% over 2 years as a result of reductions in the use of psychiatric hospital beds(2) The service reduced the number of inpatient admissions by 38% Bright Heart Health [23 states of USA] Wilkes [80]34Naturalistic Feasibility StudyAN: n = 5 (14.7%)BN: n = 12 (35.3%)BED: n = 3 (8.8%)Atypical AN: n = 4 (11.8%)Low-frequency BED: n = 1 (2.9%)Night eating syndrome: n = 1 (2.9%)Other: n = 8 (22.9%)CBT + DBT + experiential therapy + somatic therapy11-h per weekAverage period of 10 weeksBMI: Small to moderate improvementEDE-Q: Restraint, eating and weight concern subscales yielded moderate to large effect sizes, the shape concern and global score subscales yielded large effect sizes from baseline to end of treatmentBinge/Purge: Significant improvements in frequency of binge eating, vomiting, laxative use, and compulsive exercise from baseline to end of treatment (small to moderate effect sizes)(1) Treatment was proved to be moderately feasible(2) 56% of participants who started the program successfully completed the program while 15% of them dropped out(3) Majority of participants were satisfied with the service (medium to high level satisfaction) and quality of service and would recommend the program to a friendNRPrograms for all ageCommunity-based treatments Eating Recovery Center [USA] Rienecke et al. [84](i) Adults: 305(ii) Children and adolescents: 33Naturalistic Study(i) Adults:AN-R (n, %) = 41 (13.4%)AN-BP (n, %) = 16 (5.2%)BN (n, %) = 21 (6.9%)BED (n, %) = 67 (22.0%)ARFID (n, %) = 9 (3.0%)OSFED (n, %) = 139 (45.6%)(ii) Children and adolescents:AN-R (n, %) = 11 (33.3%)AN-BP (n, %) = 3 (9.1%)BN (n, %) = 2 (6.1%)BED (n, %) = 2 (6.1%)ARFID (n, %) = 1 (3.0%)OSFED (n, %) = 14 (42.1%)DBT + CBT + ACT + additional EFFT for C&A3 × 3-h group therapy sessions weekly, 1 h of individual or family therapy weekly, one biweekly appointment with a registered dietitianaverage number of days treatment for adults was 62.41 days (SD = 29.90) and for children/adolescents was 79.48 days (SD = 37.04)NRTreatment satisfaction was high, with no statistically significant differences between age groupsNR[Northeastern USA]Walker et al. [86]210Naturalistic StudyAN-BP: n = 77 (36.7%)AN-R: n = 54 (25.7%)BN: n = 42 (20.0%)BED: n = 22 (5.2%)OSFED: n = 24 (11.4%)ARFID: n = 2 (1.0%)CBT-E + DBT4-h per day, 3 days per week from 2013 to 2015 and up to 4 days per week from 2015 to 2017Average of 15.82 (SD = 13.38) weeksEAT-26: Patients who completed four or more IOP weeks demonstrated statistically significant decreases from Week 1 to dischargeNRNRACT: acceptance and commitment therapy; AN: anorexia nervosa; AN-BP: anorexia nervosa, binge-purge type; AN-R: anorexia nervosa, restricting type; ARFID: avoidant/restrictive food intake disorder; BED: binge eating disorder; BMI: body mass index; BN: bulimia nervosa; CBT: cognitive behavioral therapy; CBT-AR: cognitive behavioral therapy for avoidant/restrictive food intake disorder; CBT-E: enhanced cognitive behavioral therapy; C&A: children and adolescents; CGAS: Children’s Global Assessment Scale; DBT: dialectical behavior therapy; EAT-26: Eating Attitudes Test-26; EBW: expected body weight; ED: eating disorders; EDE: Eating Disorder Examination; EDE-Q: Eating Disorder Examination Questionnaire; EDI-2: Eating Disorder Inventory-2; EDNOS: eating disorder not otherwise specified; EFFT: emotion-focused family therapy; EPSI: Eating Pathology Symptoms Inventory; FBT: family-based treatment; FT-ED: family therapy for eating disorders; HBT: home based treatment; HT: home treatment; IBW: ideal body weight; IOP: intensive outpatient program; IPT: inpatient treatment; MANTRA: Maudsley anorexia nervosa treatment for adults; M (SD): mean (standard deviation); NR: not reported; OP: outpatient program; OSFED: other specified feeding or eating disorders; PD: purging disorder; PHP: partial hospitalization program; TAU: treatment as usual: UK: United Kingdom; USA: United States of America; VIOP: virtual intensive outpatient program; W4H: Weight for Height ratioThis paper used the same participants/dataset as Pauli et al. [54]Table 5. Summary of qualitative findings: positive aspects and challenges/areas for improvementTreatment programs and author(s)NDistribution of participants by diagnosisBrief treatment descriptionBrief summary of findingsPrograms for children and adolescentsHome-based treatmentsNorth Buckinghamshire Child and Adolescent Mental Health Service [Aylesbury, UK] Bezance and Holliday [43]9Mothers of daughters with AN or EDNOS-AN: n = 9 (100%)FBTVaried from 2 to 12 weeks (approximately 8 weeks)Positive aspects: (i) Source of hope for participants; (ii) reduced carer burden and increased confidence in supporting daughters; (iii) practical and emotional support to restore their own resources and take back controlChallenges/areas for improvement:* (i) Confusion and lack of information around HT and mother's role in treatment; (ii) negative impact of inconsistency between staff members/change in person visiting; (iii) concerns around the impact of HT on other family members, specifically other children; (iv) feelings of insufficient treatment length and fear of relapse post-HT5 out of 9 adolescents received inpatient treatment following HT, several mothers of these adolescents felt HT had been offered too late Child and Adolescent Home Treatment Team [Gloucestershire, UK] Clark-Stone et al. [44]6AN n = 6 (100%)FBTStarting with 10 contacts per week and gradually reducingA period of 6 weeksPositive aspects:* (i) New skills to manage distress at mealtimes; (ii) provided hope and empowerment in families, even following end of interventionChallenges/areas for improvement: (i) Personality differences between staff and families created mixed views amongst parents; (ii) most described initial meals with HT team as "awkward", "distressing" and "scary" Hospital Infantil Universitario Niño Jesús [Madrid, Spain] Morón-Nozaleda et al. [53]43Carers of adolescents with AN (restrictive type): n = 30 (50.8%)AN atypical: n = 7 (11.8%)AN (purging type): n = 3 (5.1%)BN: n = 5 (8.5%)ARFID: n = 3 (5.1%)OSFED: n = 11 (18.6%)CBT + FBT5 × home visits per week + 2 programmed calls per dayMean stay of 39.14 days (SD = 14.47)Positive aspects: (i) a better understanding of the disease; (ii) newly acquired ability to manage the disease in a natural environment and gain confidence; (iii) participation of all family members; (iv) lack of patient separation from the family environment; (v) greater adaptation to everyday life; (vi) better parental understanding of the sacrifices made by patients; (vii) comfort and reassurance derived from playing an active role in recovery; and (viii) reduced fear and anguish in the face of illnessChallenges/areas for improvement: Families mostly highlighted difficulties with family logisticsCommunity-based treatments Eating Disorder Intensive Pathway—East London Foundation Trust [London, UK] Komarova [59]5NA (clinicians treating children and young people)FT-ED (Maudsley Approach) + distress tolerance + CBT 3–5 times a week*A period of 6–8 weeksPositive aspects:* (i) flexibility of care (adjusting duration of pathway to needs of patient); (ii) preventing inpatient admissions; (iii) multidisciplinary team interventions; and (iv) the intensity and duration of treatmentChallenges/areas for improvement: (i) Admission prevention and in-reach; (ii) clinical team; (iii) staffing levels; (iv) staff training; and (v) practical challenges (e.g., room booking)Programs for adultsCommunity-based treatments Anorexia Nervosa Intensive Treatment Team (ANITT) [Lothian region, UK] Hannon et al. [68]5AN-R: n = 4 (80%)AN-BP: n = 1 (20%)Schema Therapy2–10 contacts a weekA period of 18-month with 6-month period of reduced-intensity treatment (progress reviews)Positive aspects: (i) Sense of safety and control and ability to practice change in the 'real world'; (ii) therapeutic alliance providing continuity of reliable, empathic and compassionate relationships and building trust; (iii) collaborative, personalized and flexible treatment planning; (iv) slow pace of change and focus on wellbeing beyond just eating and weightChallenges/areas for improvement: Experiencing difficulty when team members with whom participants had built up positive relationships left the team Yorkshire Centre for Eating Disorders [Leeds, UK] Saeidi et al. [78]Patients: 6Clinical team members: 8AN: n = 6 (100%)Treatment approach NR2–7.5 h. per week, up to five visits per weekLength NRPositive aspects:Patients: (i) Improved quality of life; (ii) accessibility and approachability of staff; (iii) a reduction in the number of hospital admissions, (iv) improved confidence, particularly as they were often involved in planning and reviewing their own careClinical team: (i) improve access for people with SEEDs to general wards by facilitating admission at an earlier stage; (ii) have a clear plan of action in place for service users before admission; (iii) support staff to manage SEED service users while on the ward Ladder to the Moon Program [Atlanta-Georgia, USA] Crenshaw [65]10AN-BP: n = 2 (20%)BN (binge-purge type): n = 2 (20%)BN (binge type): n = 6 (60%)Feminist Consciousness3 × 3-h group therapy sessions per weekA period of 3 weeks to 6 monthsPositive aspects:(i) "Acceptance": (i) acceptance of themselves and their bodies; (ii) acceptance of others; and (iii) acceptance of their spirituality(ii) "Making Different Choices": (i) making choices about depending on others; (ii) making choices about how to express feelings of anger or loss of control; and (iii) making choices about experiencing sexualityChallenges/areas for improvement: The process of developing a feminist consciousness at times created anxiety producing shifts in thinking Within Health* [USA] Wolfe et al. [87]38NRIntegrative treatment model: ACT, CBT, DBT, interpersonal with experiential modalities (e.g., art therapy, movement) (indicated based on patient presentation) at least 3 h per day; 3–5 days per weekLength NR**Positive aspects:(i) sense of being "seen" and "heard" by providers, fostering authentic connections; (ii) genuine care, empathy, and commitment of providers, promoting trust and support; (iii) creation of a “sense of community” in remote care, facilitating engagement and supportChallenges/areas for improvement: (i) lack of physical presence and contact, making it harder to connect and build relationships; (ii) technological issues (e.g., bugs, small screen) that hinder smooth communication and engagement; (iii) privacy concerns and distractions in remote settings, affecting the comfort and focus of treatmentPrograms for all ageCommunity-based treatments Equilibrio [Colombia] Rodríguez Guarin et al. [85]Patients: 14Family members:10Therapists: 8AN-R: n = 3AN-BP: n = 3AN (atypical) n = 3BN: n = 6CBT + Psychodynamic psychotherapy + DBT + Expressive therapy + Art therapy ~ 19 h per week, including individual, group and family sessionsLength is not clear, at least 8 weeks**Positive aspects:(i) being able to stay home and continuity of the treatment, (ii) allowing therapists to observe family dynamics and intervene directly in the home environment, (iii) eliminating the need to travel and for the flexibility it provided around schedulesChallenges/areas for improvement:(i) privacy, (ii) connection difficulties, (iii) lower level of participation in group sessions, (iv) no physical examination, (v) the need for "more teaching-orientated" methods during the group sessions, (vi) lack of adequate assistance during critical moments before or after meals, affecting adherence to the nutritional regimen*** Adherence to sessions was 100% for family members and 90% for patientsACT: acceptance and commitment therapy; AN: anorexia nervosa; AN-BP: anorexia nervosa, binge-purge type; AN-R: anorexia nervosa, restricting type; ARFID: avoidant/restrictive food intake disorder; BN: bulimia nervosa; CBT: cognitive behavioral therapy; DBT: dialectical behavior therapy; EDNOS: eating disorder not otherwise specified; FBT: family-based treatment; FT-ED: family therapy for eating disorders; NA: not applicable; NR: not reported; SD: standard deviation; OSFED: other specified feeding or eating disorders; UK: United Kingdom; USA: United States of America^*^This program offers treatment for all age groups, however qualitative outcomes were only focusing on adult patients
As shown in Table 2, the included papers represented a range of study designs with the majority of the papers rated as moderate to low for the quality of evidence for effectiveness. Only one study [70] fell into the highest level of classification (level 1—“experimental designs”) with a pseudo-RCT design. Six studies came under the second level (“quasi-experimental designs”), while the majority were at level 3 (“observational-analytic designs”—17 studies) or at level 4 (“observational-descriptive studies”—9 studies). Similarly, all ten studies reporting evidence on meaningfulness fell into level 3 (“single qualitative study”), and the six studies including evidence for economic evaluation came under the second lowest level of evidence (level 6: “Single economic evaluation of moderate or poor quality”).
Quantitative outcomes
Programs for children and adolescents
Six sources focusing on HBT [44, 45, 49, 50, 52, 54] and five sources focusing on ICT programs [56–58, 60, 63] reported BMI and/or weight-related outcomes. Furthermore, four studies on HBT [45, 49, 50, 54] and five studies on ICT programs [56–58, 60, 63] assessed outcomes related to ED psychopathology (e.g., binge-purge behaviors, restriction). All of these reported significant improvements in BMI and/or weight related as well as ED psychopathology outcomes. Furthermore, seven of these studies reported follow-up data, with follow-up durations ranging from 1 month to 1 year, presenting continued or maintained improvement over time [49, 50, 52, 56–58, 63].
The number of studies which included outcomes on feasibility and acceptability (e.g., treatment retention, drop out, treatment satisfaction) were fewer, with five studies on HBT programs [45, 49, 50, 53, 54] and two on ICT programs [55, 57] reporting this. These papers reported high levels of satisfaction and good levels of treatment adherence.
Cost-effectiveness outcomes for the treatment programs were presented in four studies on HBT [49, 50, 52, 53] and one study on ICT [63]. These sources reported reduced treatment cost and/or number of/length of hospital stays.
Programs for adults
Eight sources focusing on ICT programs [66, 71–76, 80] reported BMI and/or weight related outcomes. Furthermore, one HBT study [64] and eleven ICT studies [66, 69–73, 75, 76, 78, 80, 82] assessed outcomes related to ED psychopathology. Significant improvements were reported for BMI and/or weight as well as ED psychopathology outcomes following treatment, except one case study in a non-underweight patient documented stable BMI over the course of the treatment [73]. Five of these sources also reported follow-up data, with follow-up durations ranging from 1 month to 1 year, describing that improvements either continued or were maintained over time [69–71, 73, 75].
One HBT study [64] and nine ICT studies [69–71, 74, 76, 77, 79, 80, 82] presented feasibility and acceptability outcomes. These studies reported high levels of satisfaction and good levels of treatment adherence, except for one investigating at-home tube feeding for adults with BN, which most participants rated as a difficult experience [64].
Only two ICT studies [77, 78] reported cost-effectiveness outcomes. These studies reported reductions in the treatment cost and/or number of/length of hospital stays.
Programs for all age populations
Outcome data for these programs were limited. Among seven sources, there was only one ICT program presenting outcomes on ED psychopathology [86] which reported improvements following treatment. One other study presented feasibility and acceptability outcomes, demonstrating high levels of program adherence. No papers reported cost-effectiveness outcomes for this type of programs.
Qualitative outcomes
Qualitative outcomes were reported in nine papers, four on children and adolescents [43, 44, 53, 59] four on adults [65, 68, 78, 87], and one on an all age population [85]. These papers commonly presented both positive aspects and challenges/areas for improvement. Reported positive aspects included increased hopefulness, enhanced understanding of the illness, active involvement in treatment planning, acquisition of new skills, reduced isolation, and decreased hospital admissions. Described perceived challenges/areas for improvement in these papers were logistical and practical difficulties (e.g., room bookings, family logistics, technical/connection difficulties), concerns around the impact of program on other family members and staff turnover and changes during the treatment.
Discussion
This scoping review investigated ICT and HBT for EDs with a particular focus on conceptualization of these programs, their implementation, and the breadth and nature of the available evidence. The review also identified knowledge gaps and offers guidance for further research on this topic.
Two thirds of the included studies focused on ICT and one third on HBT. Nearly half of all sources targeted children and adolescents, with the remainder focusing on adults or all ages. HBT predominantly targeted children and adolescents with anorexia nervosa (AN), while ICT for this age group targeted individuals with any ED. Only two studies on HBT addressed adults or all age groups. In contrast, ICT was more commonly used among adults and across all ages, in patients with various EDs.
Even though certain aspects of the programs included in this review (e.g., admission and discharge criteria) were not always clearly presented, the majority of the programs aligned with a stepped-care model. These programs were primarily offered as step-up (e.g., moving from outpatient to ICT) or step-down (e.g., transitioning from inpatient to HBT) options, offering flexible levels of care based on patients’ progress and clinical needs. and easing transition from hospital settings to patients' natural environments. These programs also appeared to have the potential to reduce costs, by preventing inpatient admissions or reducing length of hospital stays. Even though ED clinical guidelines [11, 12, 14, 15] recommend using stepped-care treatment models and emphasize maintaining patients’ links with their home and community environments (e.g., social network, education, employment), there are as yet no specific recommendations regarding the use of ICT and HBT for EDs.
Unsurprisingly, this review highlighted differences in psychotherapeutic approaches across age groups. For children and adolescents, ED-focused family therapy (FT-ED) was the most common approach, either on its own or combined with CBT and/or DBT. In contrast, adult and all age programs typically offered combinations of individual psychotherapeutic approaches, such as CBT, DBT, schema therapy or ACT, and optional family involvement. Even though “third-wave” behavioral therapies like DBT and schema therapy are not recommended in clinical guidelines as first-line treatments for EDs, it appears that these approaches are offered in HBT or ICT programs due to promising preliminary evidence of their efficacy [9, 14, 88, 89] and perhaps also, as patients may have tried usual first line treatments previously without success.
Differences in the conceptualization and implementation of these programs can be attributed to several factors. Geographical barriers (e.g., postcode lottery, travel time) also impact the delivery and accessibility of both ICT and HBT outside large urban centres [90–92]. Additionally, limited availability of HBT for adults may stem from the fact that it might be potentially less effective or relevant for this group compared to children and adolescents. Adults may have fewer opportunities to involve family members in the treatment process at home, especially if they live alone or with individuals who are not closely connected. For children and adolescents, hospital admissions can be particularly traumatic, leading clinical teams to prioritize HBT. While family involvement can enhance treatment outcomes, implementing FT-ED and engaging families as an integral part of the process is challenging across all age groups. Geographical barriers, low income, single-parent households, and obligations such as childcare or employment can create significant burdens, making it harder for families to attend treatment sessions and manage tasks like meal preparation and supervision [93].
The available evidence on outcomes of HBTs and ICTs for EDs across different age groups were also mapped. Among 46 sources included, 31 provided quantitative outcomes while nine provided qualitative outcomes. Studies commonly reported improvements in BMI, weight restoration, and eating disorder symptoms (e.g., restriction, binge eating, purging), with some including follow-up data suggesting that these outcomes may be maintained over time. Few studies reported cost-effectiveness outcomes, citing reductions in inpatient admissions and overall healthcare costs. Beyond clinical outcomes, the HBTs and ICTs included in this review were frequently described as feasible and acceptable, with reports of patient and family satisfaction, high program adherence, and low dropout rates. Additional perceived benefits included personalization of care, increased flexibility, greater family involvement, and continuity of care within a familiar environment. Although not directly reported in the included sources, these approaches also have potential to reduce stigma and distress associated with institutionalization, while allowing clinicians to observe family dynamics more naturally, providing insights into home life and relationships [94, 95].
Several studies highlighted different challenges regarding HBTs and ICTs, including inconsistent staff availability, concerns around the impact of HBT on other family members, privacy concerns, technological barriers and lack of physical contact for virtual treatments. In addition to these, geographical aspects and workforce requirements can bring challenges in implementing and delivering these treatments. For instance, staff-to-patient ratios, commutes and transportation costs for both staff and patients are barriers to accessibility, particularly in rural areas with limited provider availability [90]. Another disadvantage could be reduced peer support opportunities in HBTs, which are often a core component of inpatient and day-treatment programs.
Our findings are consistent with observations from other psychiatric populations [25, 29, 30] suggesting that ICTs and HBTs may be potential alternatives to institution-based intensive treatments. However, as methodology of this paper focused on mapping the existing evidence without conducting a synthesis or critical appraisal of efficacy, reported benefits and improvements should be interpreted cautiously. Further evaluation through systematic review and/or meta-analysis would be required to determine the efficacy, acceptability, and cost-effectiveness of these treatments.
Gaps and recommendations for future work
This review highlights various gaps in the literature on intensive community and home-based treatments for EDs and offers suggestions for future research.
A major gap in the reviewed literature pertains to the description of the treatment programs. Essential details, such as admission and discharge criteria, treatment components and procedures, program duration, weekly number and duration of sessions, were often not clearly specified. Similarly, where interventions which were originally developed for outpatient settings (e.g., FT-ED, CBT) were integrated into programs, information was lacking as to whether these had been adapted for ICT or HBT settings, and if so in what way. Future research would benefit from providing clear definitions of components, and procedures for ICT or HBT programs which are critical for understanding how and why a program was effective (or not) and for whom, improving transparency and comparability, allowing replication, informing policy, guiding practice, and strengthening the evidence base [96, 97].
Additionally, there was a lack of comprehensive reporting on race and ethnicity among the sources included here. Furthermore, only half of the studies included both female and male patients. Notably, reporting of gender identity was almost non-existent outside of the male–female binary. Capturing such information is important, given the growing evidence suggesting that EDs may be more prevalent in gender non-conforming populations [98, 99]. Underreporting of protected or under-served characteristics may be due to regulations in some countries that restrict or discourage the collection of such data. Where possible, future research should improve reporting and increase representation to ensure rigorous evaluation of ICTs and HBTs across diverse groups.
Another notable limitation concerning the available evidence is the scarcity of higher-level evidence. We identified only one RCT protocol [42] and no completed RCTs. This dearth of experimental studies reflects both the recency of interest in HBT and ICT programs and the unique challenges in conducting RCTs within intensive ED treatment settings. These challenges include patient-related (e.g., treatment preferences), service-related, and wider systemic factors [18, 100, 101]. Moreover, the existing literature is also characterized by variability in outcome measures and data collection periods [102]. Large well-designed RCTs of HBT and ICT programs in different ED populations, assessing clinical effectiveness for patients, impacts on families and cost-effectiveness are an obvious next step. In addition, information from large-scale prospectively gathered naturalistic studies of HBT and ICT programmes would also be of value. Such studies, especially if they included genomic and deeply phenotyped clinical information, together with comorbidity and treatment outcome data could lead to advances in personalization of HBT and ICT through allowing appropriate patient stratification and better prediction of clinical outcomes [103].
Strengths and limitations
To the best of our knowledge this is the first scoping review study systematically investigating non-institutional (i.e., community and home-based) intensive treatments for EDs. Our review provides a comprehensive overview and insight into the extent of literature, characteristics of the programs and their outcomes. Other notable strengths were that the review followed reporting guidelines and used a broad range of evidence sources and methodologies. Moreover, we successfully managed to contact nine lead authors of fourteen studies to clarify some of the missing program details.
The current review also has several limitations. Firstly, although no restrictions were imposed for the publication type or geographical location, the studies included in this review were limited to publications in English. Another limitation was potential exclusion of some sources due to a lack of clarity in reporting of treatment settings and intensity. Finally, some of the outcomes presented in this review were either from the same treatment programs or involved the same patient cohorts in their sample. This overlap may introduce a bias and limit the generalizability and robustness of the conclusions drawn from the review.
Conclusion
This scoping review showed that available HBT programs are predominantly targeting children and adolescents with anorexia nervosa and used family-focused approaches. ICT programs exhibited greater variability in terms of age, diagnostic populations, and treatment approaches. The evidence base for efficacy, acceptability and cost-effectiveness thus far is limited by a lack of RCTs. However, the available literature, whilst heterogeneous in design, suggests that ICTs and HBTs for EDs may be promising alternatives to traditional institution-based intensive treatments, particularly for improving treatment experiences and reducing treatment costs and hospital admissions. To better understand which programs are the most effective and which approach works best for specific patient populations, future research should focus on conducting higher-quality studies. Such studies would need to includeimproved and consistent reporting of program characteristics and ideally use the same outcome measures across studies. This would also facilitate conduct of comprehensive systematic reviews and meta-analyses.
Supplementary Information
Additional file1 (DOCX 40 KB)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rodríguez Guarin M, Gempeler Rueda J, Castro SM, Ospina MM, Villanueva Betancourth C, Amórtegui JP, et al. Feasibility and acceptability of comprehensive virtual treatment in eating disorders: perspectives from patients, parents and therapists during the COVID-19 Pandemic. Rev Colomb Psiquiatr (Engl Ed). 2021.10.1016/j.rcpeng.2023.11.00338008675 · doi ↗ · pubmed ↗
- 2İnce B, Phillips MD, Dalton B, Irish M, Webb H, Mercado Beivide D, et al. Stepping into day treatment approach versus inpatient treatment for adults with anorexia nervosa: the DAISIES RCT. Health Technology Assessment 2024.10.3310/FTJP 6744 PMC 1227804339943786 · doi ↗ · pubmed ↗