Efficacy of new immunomodulatory drugs on major adverse cardiovascular events in patients with coronary heart disease: a systematic review and meta-analysis of randomized controlled trials
Donghang He, Yuhan Li, Zefei Jiang, Xin Cao, Rong Luo

TL;DR
New anti-inflammatory drugs like colchicine and canakinumab can reduce heart-related risks in patients with coronary disease when used long-term.
Contribution
The study identifies specific immunomodulatory drugs that effectively reduce major adverse cardiovascular events in coronary heart disease patients.
Findings
NLRP3 inflammasome and IL-1β inhibitors significantly reduced MACE in patients with coronary heart disease.
Benefits of immunomodulatory drugs were observed only in trials with follow-up exceeding six months.
No significant MACE reduction was found for broad-spectrum immunomodulators or Lp-PLA2 inhibitors.
Abstract
Despite optimal standard therapy, residual inflammation continues to increase major adverse cardiovascular events (MACE) in patients with coronary heart disease (CHD). New immunomodulatory drugs targeting specific immune pathways have shown mixed efficacy across trials, warranting comprehensive evaluation of their role in secondary prevention. We performed a systematic review and meta-analysis of 25 randomized controlled trials (RCTs) from January 1, 2014, to October 1, 2024, identified from eight databases: the cochrane library, (public medicine) pubmed, embase, web of science, china national knowledge infrastructure (CNKI), wanfang data knowledge service platform(WanFang), Weipu information database(VIP), and china biomedical literature database (SinoMed). Eligible studies assessed the efficacy of immunomodulatory agents, including colchicine, and canakinumab on MACE. Primary outcome…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
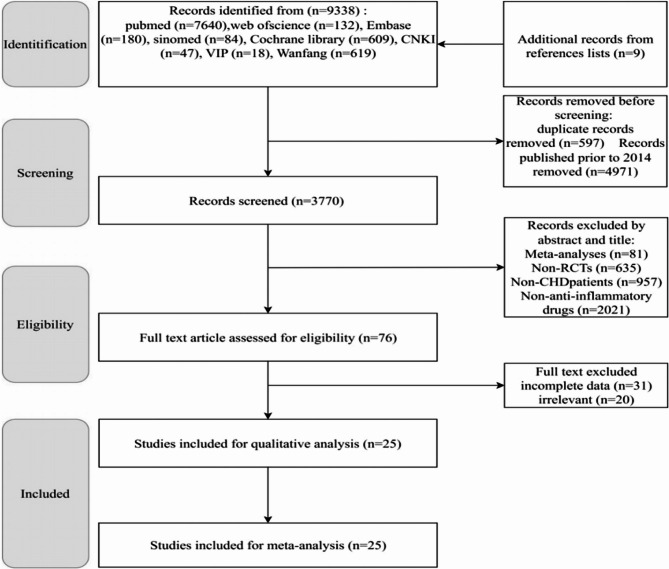 Figure 1
Figure 1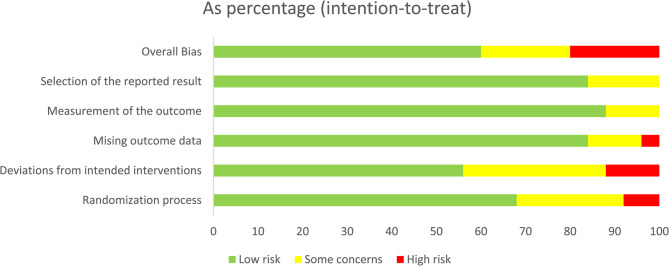 Figure 2
Figure 2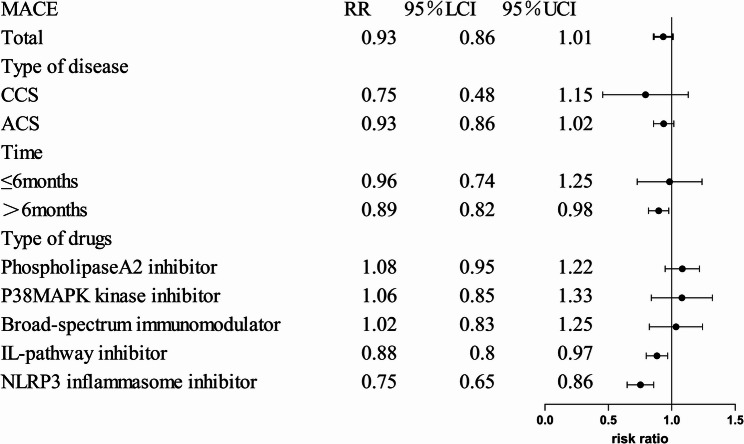 Figure 3
Figure 3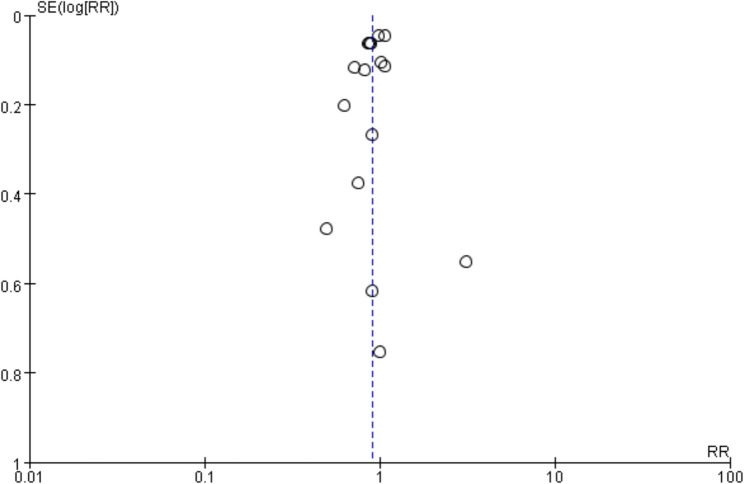 Figure 4
Figure 4- —National Natural Science Foundation of China
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAtherosclerosis and Cardiovascular Diseases · Cardiac Fibrosis and Remodeling · Heart rate and cardiovascular health
Introduction
Cardiovascular death remains the leading cause of mortality worldwide. According to 2020 mortality data, heart disease and stroke now cause more deaths each year than the combined total of cancer and chronic lower respiratory diseases. In 2020, the death rate from heart disease and stroke was 207.1 per 100,000 people. In 2020, cardiovascular diseases (CVD) were estimated to account for 19.05 million deaths worldwide, representing an increase of 8.71% compared to 2010. Ischemic heart disease climbed from the third leading cause of death in 1990 to the top cause by 2019 [1].
Coronary heart disease (CHD) patients remain at high risk of major adverse cardiovascular events (MACE), including myocardial infarction, cardiovascular death, and cardioembolic stroke, despite receiving optimized, guideline-directed therapies. The recurrence of MACE remains concerningly high: antiplatelet therapy is associated with a recurrence rate of up to 27.7%, while statin therapy and even complete revascularization do not fully mitigate this risk, with over 20.0% of patients experiencing recurrent events within three years [2].
Repeated hospitalizations, reduced functional capacity, and increasing financial stress place a dual physical and psychological burden on affected individuals. Therefore, identifying more effective therapeutic strategies to improve long-term outcomes in CHD has become a critical public health priority.
Contemporary CHD management strategies are based on three pillars: thrombus inhibition (e.g., aspirin), reduction of low-density lipoprotein cholesterol (e.g.,statins), and restoration of coronary blood flow perfusion (e.g.,stenting) [3]. However, emerging evidence suggests atherosclerosis is fundamentally a chronic inflammatory process [4]. Even under optimal lipid-lowering and antithrombotic therapy, the residual inflammation risk contribute to drive adverse cardiovascular events [5]. The landmark Canakinumab Anti-Inflammatory Thrombosis Outcomes Study (CANTOS) first demonstrated that targeted inhibition of interleukin-1β(IL-1β) significantly reduced MACE risk independently of lipid levels [6]. However, the subsequent trials have yielded mixed results: low-dose colchicine significantly reduced MACE in Colchicine Cardiovascular Outcomes Trial (COLCOT) and Low-Dose Colchicine 2 trial (LoDoCo2) [7, 8], whereas methotrexate failed to confer cardiovascular benefits in the Cardiovascular Inflammation Reduction Trial (CIRT) [9].These findings underscore the persistent controversy regarding the clinical utility of new immunomodulatory drugs. Evidence for the efficacy and safety of targeting alternative inflammatory mediators, such as IL-6, TNF-α, and the NLRP3 inflammasome, remains inconsistent, contributing to uncertainty in guideline recommendations. A comprehensive evaluation of these agents is thus crucial for refining secondary prevention strategies in CHD.
Previous meta-analyses focused narrowly on individual agents, such as colchicine [10], and often excluded more recent trials. To address this gap, we conducted a systematic review and meta-analysis of updated RCT evidence to address the following key questions: (1) Do inflammatory pathway inhibitors reduce MACE risk in patients with CHD? (2) Are there differences in efficacy and safety among drug classes or molecular targets? (3) Is existing evidence sufficient to guide precision medicine approaches in targeted CHD populations, including stable angina and acute myocardial infarction cohorts?
By addressing these questions, our study aims to provide robust evidence to guide clinical decision-making and providing a theoretical foundation for the development of immunomodulatory approaches in cardiovascular medicine.
Overview and registration
This meta-analysis was conducted in accordance with the recommendations of the “Preferred Reporting Entries for Systematic Reviews and Meta-Analyses” (PRISMA) statement and has been registered in the PROSPERO database of prospective Systematic Reviews (Registration ID: [CRD42024597008]).
Search strategy
A comprehensive literature search was performed in PubMed, Embase, Cochrane Library, Web of Science, Sinomed, VIP Information, Wanfang Data Knowledge Service Platform (WanFang), and China National Knowledge Infrastructure (CNKI) from January 1, 2014, to October 1, 2024, without language restrictions. The search strategy combined terms for (1) new immunomodulatory drugs, such as interleukins, colchicine and methotrexate. (2) coronary artery disease, using Medical Subject Headings (MeSH) and free-text keywords adapted for each database. Supplementary Table 1 lists the adjusted search strategies for each database. Conduct manual searches of relevant conference abstracts, clinical trial registries (e.g., ClinicalTrials.gov), and perform citation tracing of reference literature.
Inclusion criteria
(1)Population: Adult patients (≥ 18 years) with a diagnosis of coronary heart disease (CHD), as defined by recognized guidelines [11, 12], confirmed by one or more of the following objective criteria: a history of myocardial infarction (MI), percutaneous coronary intervention (PCI), coronary artery bypass grafting (CABG), significant multivessel coronary artery disease documented by angiography, or ischemic cardiomyopathy (left ventricular ejection fraction < 35% of ischemic etiology).(2) Intervention: use of new immunomodulatory drugs. (3) Comparison: placebo or other drugs. (4) Outcome: studies with cardiovascular outcomes (e.g., MACE, Stroke). (5) Study Design: randomized controlled trials (RCTs). (6) Publication Date: Studies published from January 2014 to October 2024. (7) Data Availability: full-text accessible with complete outcome data.
Exclusion criteria
- Duplicate studies. (2) Studies with non-cardiovascular outcomes. (3) Non-randomized controlled studies. (4) No valid data was provided or the data was missing.
Study selection
The retrieved literature was imported into Endnote 20, and duplicate literature was deleted. Two reviewers used the aforementioned inclusion and exclusion criteria to screen the studies by reading the titles and abstracts. Following the initial screening, the full texts of the identified studies were reviewed to determine their eligibility, and those that did not meet the inclusion criteria were excluded. Conflicting assessments of study eligibility were resolved through reviewer discussion or consultation with a third reviewer.
Risk of bias assessment
The quality assessment of the included study was conducted in accordance with the standards outlined in the Cochrane Handbook of Systematic Reviews of Interventions (Edition 5.0.1). Two independent reviewers will use the Cochrane Risk of Bias Assessment Tool (RoB 2) to evaluate the risk of bias in randomized controlled trials. Each criterion was assessed using three rating categories based on the study specifics: “low risk”, “high risk”, or “unclear risk”. Any discrepancies will be resolved through discussion or arbitration by a third reviewer [13].
Data extraction
This study included RCTs from 2014 to 2024 that explored the effects of various inflammatory pathway blockers on the cardiovascular system of patients with CHD. These drugs included anakinra, colchicine, tocilizumab, canakinumab, varespladib, darapladib, losmapimod, and methotrexate. The primary cardiovascular outcomes we focused on included MACE, all-cause mortality, revascularization, and several inflammatory indicators. MACE is defined as a composite of cardiovascular death, myocardial infarction, and stroke [14]. In studies that did not report the definition of MACE, we calculated the numbers of these three events based on the aforementioned definition to obtain this composite indicator. In studies employing multiple drug doses, we included them in separate groups. For studies reporting clinical outcomes at multiple follow-up time points, we utilized the data from the longest follow-up time. Two reviewers independently extracted data items from the included studies and assessed the eligibility of the studies based on the aforementioned criteria. The research began with a preliminary screening through titles and abstracts. Following the initial screening, a comprehensive review of the confirmed research texts was conducted to determine their eligibility. Baseline characteristics and clinical outcomes of interest were extracted using standardized data extraction tables. Some studies did not show the continuous data directly. For studies reporting continuous data as medians and interquartile ranges (IQRs), we estimated the means and standard deviations (SDs) using established statistical conversion formulas and incorporated these values into our literature database. Any discrepancies were resolved through discussion. A third reviewer will be consulted if required.
Statistical analysis
In this study, data synthesis was performed using Review Manager 5.4 software (Cochrane Collaboration, Oxford, UK). The meta-analysis of categorical variables was conducted using the Mantel-Haenszel (M-H) statistical method to calculate risk ratios (RR) with 95% confidence intervals (CI). For continuous variables, the inverse variance (I-V) statistical method was employed to calculate mean differences (MD), standardized mean differences (SMD), and 95% CI. MD was used to interpret outcomes when the units and dimensions of the measurement scales were consistent (e.g., neutrophil count), while SMD was applied for outcomes with varying units (e.g., hs-CRP, IL-6). Statistical heterogeneity across pooled data was assessed using the I² statistic: an I²<50% indicated low heterogeneity, and a fixed-effect model (FEM) was selected for synthesis; an I²≥ 50% suggested substantial heterogeneity, in which case a random effects model (REM) was used to synthesize the data. All tests were two-tailed, and statistical significance was defined as P < 0.05. Conducting a meta-regression by using Stata 17.0 to explore potential sources of heterogeneity.
Subgroup analyses were performed based on the following three criteria: (1) Type of new immunomodulatory drugs (e.g., colchicine, methotrexate); (2) Follow-up duration (≤ 6 months vs.>6 months); (3) Disease classification of enrolled patients [ACS (Acute Coronary Syndrome) or CCS (Chronic Coronary Syndrome)]. Sensitivity analysis was conducted by gradually excluding the included individual studies to explore the impact of the quality of individual studies on the overall results. Publication bias was evaluated using funnel plots when ≥ 10 studies reported primary outcome data [13], meanwhile, Begg’s test and Egger’s test were conducted to calculate the publication bias [15]– [16].
This study utilized the GRADE (Grading of Recommendations Assessment, Development, and Evaluation) system to evaluate the quality of evidence for primary outcomes. The GRADE system reduced evidence quality based on five domains: risk of bias, inconsistency, indirectness, imprecision, and publication bias. Evidence quality was categorized into four levels: high, moderate, low, or very low. Two independent researchers conducted assessments using the GRADE pro GDT online tool, with disagreements resolved by discussion and consultation with a third reviewer.
Result
Search results and study characteristics
Initially, 9,329 relevant articles were retrieved from 8 databases, with an additional 9 articles identified from reference lists, totaling 9,338 articles. After excluding non-recent (older than 10 years) and duplicate publications, 3,770 articles remained for screening. Following title/abstract review and full-text assessment, a final total of 25 articles met the inclusion criteria [6–9, 14, 17–36]. The PRISMA flowchart is shown in Fig. 1.Fig. 1. Flow chat
The included studies comprised large-scale projects such as CANTOS and COLCOT, along with several smaller investigations. The new immunomodulatory drugs were utilized: anakinra (3 studies), colchicine (15 studies), tocilizumab (1 study), canakinumab (1 study), varespladib (1 study), darapladib (2 studies), methotrexate (1 study), and losmapimod (1 study). Baseline characteristics of the study populations are summarized in Table 1.
Table 1. Characteristics of studiesNumberStudy IDCountrySample size(E/C)Gender(F/M)Age(E/C)InterventionComparisonType of drugsOutcomeDurationTypeDiagnosis methodsFunding sources1Abbate2015 [17]US20/20E:2/18 C:8/12E:58 ± 11.2 C:54.8 ± 9.6anakinra 100 mg QDplaceboIL-pathway inhibitorACDE28monthsRCTHistory of PCINational Institutes ofHealth2Abbate2020 [18]USE1:33E2:31C:35E1:9/27E2:5/26C:5/30E1:54.8 ± 10.1E2: 53.6 ± 12.4C: 57.4 ± 10.8E1:anakinra 100 mg QDE2:anakinra 100 mg BIDplaceboIL-pathway inhibitorA12monthsRCTHistory of MI, CABGNational Institutes ofHealth3Akodad2017 [19]France23/21E:4/19C:5/16E:60.1 ± 13.1C:59.7 ± 11.4colchicine 1 mg QDOMT aloneNLRP3 inflammasome inhibitorAG1monthRCTHistory of MI, PCINo4Akrami2021 [20]Iran120/129E:34/86C: 42/87E:56.9 ± 7.56C:56.89 ± 7.45colchicine 0.5 mg QDplaceboNLRP3 inflammasome inhibitorACD6 monthsRCTHistory of MI, significant multivessel coronary artery disease documented by angiographyShiraz University of Medical Sciences5Broch2021 [21]Norway101/98E:21/80C:11/87E:62 ± 10C:60 ± 9tocilizumab 280 mg0.9%NaCl 100 mlIL-pathway inhibitorGH6 monthsRCTHistory of MISouth-Eastern Norway RegionalHealth Authority, the Central Norway Regional Health Authority, andRoche6Deftereos2015 [22]Greece77/74E:25/52C:18/52E:58 ± 9C:59 ± 12.72colchicine 0.5 mg BIDplaceboNLRP3 inflammasome inhibitorGHduring hospitalizationRCTHistory of MIInvestigator-initiated and -funded study.7Ridker2017 [6]AmericaE1:2170E2:2284E3:2263C:3344E1:541/1629E2:572/1712E3:606/1657C:865/2479E1:61.1 ± 10.1E2:61.2 ± 10.0E3:61.1 ± 10.1C:61.1 ± 10.0E1:canakinumab 50 mgQ3ME2:canakinumab 150 mgQ3ME3:canakinumab 300 mg Q3MplaceboIL-pathway inhibitorACDE3.7 yearsRCTHistory of MINational Institutes ofHealth8Hennessy2019 [23]Australia119/118E:30/89C:25/93E:61 ± 13.6C:61 ± 12.5colchicine 0.5 mg QDplaceboNLRP3 inflammasome inhibitorG1 monthRCTHistory of MINational Heart Foundation of Australia9Kajikawa2019* [24]Japan14/141/2768 ± 7colchicine 0.5 mg QDplaceboNLRP3 inflammasome inhibitorG14daysRCTHistory of MI, PCI, CABG, significant multivessel coronary artery disease documented by angiographyMinistry of Health, Labour and Welfare10Martinez2015 [25]AustraliaE1:40E2:33C:10E1:3/37E2:3/30C:3/7E1:64.5 ± 10.2E2:61.1 ± 10.C:61.3 ± 6.7E1:ACS with colchicine 1.5 mgE2:CAD with colchicine 1.5 mgplaceboNLRP3 inflammasome inhibitorGduring hospitalizationRCTHistory of MISydney Medical School Foundation Grant11Mewton2021 [26]France101/91E:21/80C:17/74E:59.0 ± 10.6C:60.9 ± 10.4colchicine 0.5 mg BIDplaceboNLRP3 inflammasome inhibitorACHI12 monthsRCTHistory of MI, PCIFrench Ministry of Health12Morton2014 [27]UK93/89E:30/63C:22/67E:61.4 ± 11.7 C:61.3 ± 12.3anakinra 100 mg QDplaceboIL-pathway inhibitorAFG12 monthsRCTHistory of MIUK Medical Research Council ExperimentalMedicine Grant13Nicholls2014 [28]Australia2573/2572E:660/1913C:691/1881E:60.7 ± 9.8C:61.0 ± 10.0varespladib 500 mg QDplaceboPhospholipaseA2 inhibitorACD4 monthsRCTHistory of MIAnthera Pharmaceuticals.14Nidorf2020 [8]Australia2762/2760E:457/2305C:389/2371E:65.8 ± 8.4C:65.9 ± 8.7colchicine 0.5 mg QDplaceboNLRP3 inflammasome inhibitorACD29 monthsRCTSignificant multivessel coronary artery disease documented by angiographyNHMRC project grant15O’Donoghue2014 [29]UK6504/6522E:1657/4847C:1669/4853E:64.4 ± 8.2C:64.6 ± 8.9darapladib 160 mg QDplaceboPhospholipaseA2 inhibitorACDE2.5yearsRCTHistory of MIGlaxoSmithKline.16O’Donoghue2016 [30]UK1731/1758E:500/1231C:532/1226E:67.1 ± 9.6C:67 ± 8.9losmapimod 7.5 mg BIDplaceboP38MAPK kinase inhibitorAE6 monthsRCTHistory of MIGlaxoSmithKline17Psaltis2024 [31]Australia32/32E:4/28C:2/32E:59.16 ± 11.22C:64.42 ± 11.53colchicine 0.5 mg QDplaceboNLRP3 inflammasome inhibitorG18 monthsRCTHistory of MI, significant multivessel coronary artery disease documented by angiographyNational Health andMedical Research Council18Ridker2019 [9]US2391/2395E:461/1930C:437/1958E:65.71 ± 8.97C:65.83 ± 8.82methotrexate 18.8 mg QWplaceboBroad-spectrum immunomodulatorADE6 monthsRCTHistory of MI, significant multivessel coronary artery disease documented by angiographyNational Institutes ofHealth19Roubille2024 [32]Canada462/497E:106/356C:107/390E:62.5 ± 10.4C:62.4 ± 10.7colchicine 0.5 mg QDplaceboNLRP3 inflammasome inhibitorABEF22.6 monthsRCTHistory of MI,The Canadian Institutes of HealthResearch20Shah2020 [33]US206/194E:13/193C:13/181E:65.9 ± 9.9C:66.6 ± 10.2colchicine 1.8 mgplaceboNLRP3 inflammasome inhibitorADEF1 monthRCTHistory of MI, PCIAmerican Heart Association Clinical Resea9rch Program21Tardif2019 [7]Canada2366/2379E:472/1894C:437/1942E:60.6 ± 10.7C:60.5 ± 10.6colchicine 0.5 mg QDplaceboNLRP3 inflammasome inhibitorABEEF23 monthsRCTHistory of MI,No22Tong2020 [34]Australia396/399E:74/322C:89/310E:59.7 ± 10.2C:60.0 ± 10.4colchicine 0.5 mg BID for the first month, 0.5 mg QD for 11 monthsplaceboNLRP3 inflammasome inhibitorACDE12 monthsRCTHistory of MI, significant multivessel coronary artery disease documented by angiographyPeninsula Health and Faculty ofMedicine23Vaidya2018 [35]Australia40/40E:8/32C:10/30E:56.3 ± 8.9C:58.4 ± 14.2colchicine 0.5 mg QD plus OMTOMT aloneNLRP3 inflammasome inhibitorG12 monthsRCTSignificant multivessel coronary artery disease documented by angiographyNo24White2014 [14]UK7904/7924E: 1506/6398C: 1461/6463E:65 ± 8.9C:65 ± 8.9darapladib 160 mg QDplaceboPhospholipaseA2 inhibitorACDE3.7 yearsRCTHistory of MI, PCI, CABG, significant multivessel coronary artery disease documented by angiographyNo25Xu2023 [36]ChinaE1:107E2:108C:95E1:29/78E2:30/7C:20/75E1:61.5 ± 12.2E2:62.5 ± 12.2C:60.5 ± 10.8E1:colchicine 0.5 mg QDE2:colchicine 0.25 mg QDplaceboNLRP3 inflammasome inhibitorACHGI12 monthsRCTHistory of MIScience and Technology Plan Project of Huadu District, Guangzhou CityA. MACE B. Cardiac arrest C. Unstable angina D. Any case of death E. Revascularization F. Gastrointestinal adverse reaction G. Inflammatory markersOMT optimal medical therapy, NLRP3 NOD-like receptor family, pyrin domain-containing protein 3 inflammasome, IL Interleukin, P38MAPK kinase inhibitor, p38 Mitogen-Activated Protein Kinase Inhibitor, PCI percutaneous coronary intervention, LVEF left ventricular ejection fraction, CABG coronary artery bypass grafting, MI myocardial infarctionH.Infarct size I.LVEF. *No age or gender grouping was performed (the literature did not provide grouped data)
Risk of bias assessment
This systematic review included a total of 25 RCTs, rigorously assessed using the Cochrane Risk of Bias tool (RoB 2.0). The risk of bias assessment results are illustrated in Fig. 2. Details information is shown in supplement Fig. 2.Fig. 2. Risks of bias of the included studies. risk of bias. Green: low risk; yellow: some concern; red: high risk
Randomization process: most studies were judged as low risk, although a few raised some concerns, and two studies were judged as high risk [25, 35]. Deviations from intended interventions: 8 studies were rated as having some concerns [17]– [18, 25–27, 29, 35]– [14], and 3 studies were rated as high risk [19, 22, 36], primarily due to the open-label design without placebo control. Missing outcome data: most studies were rated as low risk because all randomized participants completed follow-up. One study was considered high risk due to a high rate of loss to follow-up [34]. Measurement of the outcome: The majority of studies were judged as low risk, particularly those employing blinded outcome assessment; only three studies were rated as having some concerns [19, 25, 36]. Selection of the reported result: Four studies raised some concerns, mainly due to unavailable preregistered protocols or potential selective reporting [23–25, 29].
Primary outcome
The primary outcome of this study was the incidence of MACE. Subgroup analyses were conducted based on the type of new immunomodulatory drugs, follow-up duration, and disease classification, with results detailed in Fig.3.Fig. 3. Subgroup analysis of MACE
Overall summary
Among the 25 included studies, 15 reported the incidence of major adverse cardiovascular events (MACE) [6–9, 14, 17, 20, 26–30, 32–34]. Adding new immunomodulatory drugs to standard therapy during treatment did not show significant improvement in MACE incidence compared to standard therapy alone. (RR = 0.92,95%CI: [0.84,1.01], P=0.09, I²=60%, 17 trials, 65,420 participants).
Subgroup analysis based on the types of new immunomodulatory drugs
Based on different immunomodulatory drugs, these studies were divided into the IL-pathway inhibitors, NLRP3 inflammasome inhibitors, Lipoprotein-associated phospholipase A2 (Lp-PLA2) Inhibitors, p38 Mitogen-Activated Protein Kinase (MAPK) Inhibitors, broad-Spectrum immunomodulators. Compared with the control group, the incidence of MACE was significantly reduced in the NLRP3 inflammasome inhibitors group (RR = 0.75, 95% CI: [0.65,0.86], P < 0.0001), and the IL-pathway inhibitors group (RR = 0.86, 95% CI: [0.75,0.97], P = 0.02). However, in the Broad-spectrum immunomodulator group, Lp-PLA2 inhibitor group, and p38 MAPK kinase inhibitor group, no significant improvement in MACE incidence was observed compared with the control group (P > 0.05). The forest plot are shown in Supplement Fig. 2.1.
Subgroup analysis based on the follow-up time
Based on the follow-up periods, these studies were divided into a group with follow-up ≤ 6 months and a group with follow-up > 6 months. Compared with the control group, when the follow-up period was ≤ 6 months, the improvement in MACE incidence in the intervention group was not significant (P > 0.05), whereas when the follow-up period exceeded 6 months, the intervention group showed a significant reduction in MACE incidence (RR = 0.88, 95% CI: [0.79,0.97], P = 0.01). The forest plot are shown in Supplement Fig. 2.2.
Subgroup analysis based on the disease classification
Based on the different disease types of the included population, these studies were divided into an ACS group and a CCS group. Compared with the control group, the MACE incidence rate in the intervention group with CCS showed no significant improvement (P > 0.05), and similarly, the incidence of MACE in the intervention group with ACS also showed no significant improvement (P > 0.05). The forest plot are shown in Supplement Fig. 2.3.
Secondary outcome
The secondary outcomes of this study included the incidence of, incidence of cardiac arrest (CA), incidence of gastrointestinal adverse reaction, incidence of death from any cause, incidence of revascularization, incidence of infection, hs-CRP, left ventricular ejection fraction (LVEF), IL-6, infarct size, and neutrophil count. The specific details are provided in the Table 2.
Table 2. Analysis of primary and secondary outcomeOutcomesstudy numbersP for Q testI²Effect modeRR/MD(95%)P for Z testMACE150.00260%RE0.93 [0.85, 1.02]0.13All-cause mortality130.670%RE0.97 [0.92, 1.03]0.30Cardiac arrest30.930%FE0.87 [0.38, 2.01]0.75Revascularization9<0.000175%RE0.85 [0.73, 0.98]0.03Infection70.550%FE1.06 [0.92, 1.22]0.45Angina100.00459%RE0.72 [0.58, 0.90]0.004Gastrointestinal adverse reaction40.0169%RE1.30 [0.88, 1.93]0.19LVEF20.880%FE1.41 [0.08, 2.75]0.04Hs-CRP9<0.000193%RE−1.05 [−2.10, 0.00]0.05IL-63<0.000197%RE−4.11 [−7.13, −1.09]0.008Neutrophil count20.800%FE−0.74 [−1.19, −0.29]0.001
Incidence of CA
Three studies [7, 26, 32] reported the cardiac arrest. The comparison of the cardiac arrest indicator between the intervention group and placebo group showed no statistically significant difference (RR = 0.87, 95% CI: [0.38, 2.01], P = 0.75). These results show that new immunomodulatory drugs could not reduce the incidence of CA compared with different placebo groups. The forest plot are shown in Supplement Fig. 3.
Incidence of angina
Ten studies [6, 7, 14, 17, 20, 26, 28, 32, 34, 36] (13 trials) reported angina incidence. The results showed that compared with the placebo group, the incidence of angina in the intervention group were markedly improved, with a statistically significant difference (RR = 0.73, 95% CI: [0.58,0.92], P = 0.007). These results show that new immunomodulatory drugs could reduce the incidence of angina compared with different placebo groups. The forest plot are shown in Supplement Fig. 4.
Incidence of all-cause mortality
Thirteen studies [6–9, 14, 17, 18, 20, 27–29, 33, 34] (16 trials) reported the incidence of death from any cause. The results showed no statistically significant difference in the death from any cause outcome between the intervention group and placebo group (RR = 0.98, 95% CI: [0.92, 1.04], P = 0.50). These results show that new immunomodulatory drugs could not reduce the incidence of all-cause mortality compared with different placebo groups. The forest plot are shown in Supplement Fig. 5.
Incidence of revascularization
Nine studies [6, 8, 9, 14, 17, 29, 30, 33, 34] (11 trials) reported the revascularization indicators. The outcomes demonstrated that the incidence of revascularization in the intervention group reduced with a statistically significant difference (RR = 0.86, 95% CI: [0.74,0.99], P = 0.04) compared with the different control group. These results show that new immunomodulatory drugs could reduce the incidence of revascularization compared with different placebo groups. The forest plot are shown in Supplement Fig. 6.
Incidence of gastrointestinal adverse effect
Four studies [7, 32, 33, 36] (5 trials) reported the incidence of gastrointestinal adverse effect. The incidence of gastrointestinal adverse showed no statistically significant difference between the intervention group and placebo group (RR = 1.22, 95% CI: [0.85, 1.74], P = 0.27). These results show that new immunomodulatory drugs could not reduce the incidence of revascularization compared with different placebo groups. The forest plot are shown in Supplement Fig. 7.
Incidence of infection
Seven studies [6–9, 18, 27, 29] encompassing 10 trials reported the incidence of infection. There was no statistically significant difference between the intervention and placebo groups (RR = 1.06, 95% CI: 0.92–1.22, P = 0.45). These findings indicate that the new immunomodulatory drugs did not reduce the risk of infection compared with various placebo controls. The corresponding forest plot is presented in Supplementary Fig. 12.
Inflammatory markers
Nine [19, 21–24, 26, 27, 35, 36] studies (10 trials) reported the hs-CRP. The results showed that there was no significant difference of hs-CRP between placebo group and intervention group (MD=−1.05, 95% CI: [−2.10,0.00], P = 0.05). The forest plot are shown in Supplementary Fig. 8. A total of 3 studies [25, 27, 36] (5 trials) reported IL-6. The results showed that IL-6 was markedly reduced in intervention group when compared with the different placebo groups, (MD=−4.11, 95% CI: [−7.13, −1.09, P = 0.008). The forest plot are shown in Supplementary Fig. 9. A total of 2 studies [22, 36] (3 trials) reported neutrophil count. The results showed that the neutrophil count in the intervention group were markedly reduced compared with the different placebo groups, (MD=−0.74, 95% CI: [−1.19, −0.29], P = 0.001). The forest plot are shown in Supplementary Fig. 10. These results show that compared with different placebo groups, the new immunomodulatory drugs could not reduce level of the hs-CRP, but could reduce the level of IL-6 and neutrophil count.
LVEF
Two studies [26, 36] (3 trials) reported data on left ventricular ejection fraction. The comparison of LVEF between the intervention group and different placebo groups showed no statistically significant difference (MD = 1.41, 95% CI: [0.08,2.75], P = 0.04). These results show that new immunomodulatory drugs were associated with an increase in LVEF compared with various placebo groups. The forest plot are shown in Supplementary Fig. 11.
Publication bias, meta-regression, and sensitivity analysis
The funnel plots are shown in Fig. 4, the results showed that the funnel plot was symmetrical, suggesting the absence of publication bias. In addition, both Egger’s test (P = 1.00) and Begg’s test (P = 0.84) indicated P > 0.05, further supporting the conclusion that publication bias is unlikely.Fig. 4. Funnel plot of MACE
Meta-regression indicated that type of drugs is a significant source of heterogeneity, P = 0.002. The country class and year are not a significant source of heterogeneity, P>0.05.
In the sensitivity analysis, the point estimate for MACE remained stable (RR range: 0.91–0.95) regardless of which individual study was omitted, indicating the overall result was robust. Details information is shown in Table 3. The exclusion of certain large trials, such as Nicholls 2014 or Nidorf 2020, led to minor fluctuations in the pooled risk ratio and its confidence intervals, but these changes were not substantial enough to alter the primary conclusion of the analysis. For instance, upon excluding Nicholls 2014, the result became statistically significant (RR = 0.90, 95% CI: 0.82, 0.98, P = 0.02), while excluding Nidorf 2020 yielded an RR of 0.94 (95% CI: 0.86,1.03, P = 0.20). The fact that no single study dramatically changed the effect estimate suggests that the observed heterogeneity (I² = 60%) is not driven solely by any one trial but is more likely attributable to broader differences across studies, such as variations in drug mechanisms of action, as identified in our subgroup analysis and meta-regression.
Table 3. Influence plot of MACEIncidence of MACEExcluded Study IDRR(95%CI)P for z testI²P for Q testNone0.92 [0.84, 1.01]0.000760%0.09 Abbate 2020 [18]0.92 [0.84, 1.01]0.000463%0.09 Akrami 2021 [20]0.93 [0.85, 1.02]0.1161%0.0008 MEWTON 2021 [26]0.92 [0.84, 1.01]0.1063%0.0004 Morton 2015 [27]0.92 [0.84, 1.00]0.0558%0.002 Nicholls 2014 [28]0.90 [0.82, 0.98]0.0254%0.006 Nidorf 2020 [8]0.94 [0.86, 1.03]0.2056%0.0003 O’Donoghue 2014 [29]0.91 [0.82, 1.02]0.1162%0.0005 O’Donoghue 2016 [30]0.91 [0.83, 1.01]0.0761%0.0006 Ridker 2017(a) [6]0.93 [0.84, 1.03]0.1661%0.0008 Ridker 2017(b) [6]0.93 [0.85, 1.03]0.1760%0.001 Ridker 2017(c) [6]0.93 [0.84, 1.03]0.1660%0.0010 Ridker 2019 [9]0.91 [0.83, 1.01]0.0862%0.0005Roubille 2024 [32]0.94 [0.86, 1.03]0.1758%0.002 Shah 2020 [33]0.92 [0.84, 1.02]0.1062%0.0004Tardif 2019 [7]0.93 [0.85, 1.03]0.1561%0.0008 Tong 2020 [34]0.93 [0.84, 1.02]0.1162%0.0005 WHITE 2014 [14]0.90 [0.82, 1.00]0.0555%0.004
Quality of the evidence
This study conducted GRADE evidence ratings for the primary outcome and secondary outcomes. The evidence quality for the incidence of MACEs was accessed as moderate. This indicates that the current evidence is highly credible regarding the efficacy and safety of new immunomodulatory drugs therapy in patients with CHD. Detailed results are presented in Table 4.
Table 4. Quality of the evidence (GRADE)Outcome MeasureNo. of StudiesRisk of BiasInconsistencyIndirectnessImprecisionPublication BiasGRADE RatingMACE15Not downgradedDowngrade bNot downgradedNot downgradedNot downgradedModerateDeath from any cause16Not downgradedNot downgradedNot downgradedNot downgradedNot downgradedModerateCardiac arrest3Not downgradedNot downgradedNot downgradedNot downgradedNot downgradedHighAngina10Not downgradedDowngrade bNot downgradedNot downgradedNot downgradedLowGastrointestinal adverse reaction4Not downgradedDowngrade bNot downgradedNot downgradedNot downgradedLowRevascularization9Not downgradedDowngrade bNot downgradedNot downgradedNot downgradedLowHs-CRP9Not downgradedDowngrade bNot downgradedNot downgradedDowngrade cLowLeft ventricular ejection fraction2Not downgradedNot downgradedNot downgradedNot downgradedNot downgradedHighIL-63Not downgradedDowngrade bNot downgradedNot downgradedNot downgradedModerateNeutrophil count2Not downgradedNot downgradedNot downgradedNot downgradedNot downgradedHigh
Discussion
Our meta-analysis systematically reviewed the efficacy and safety of new immunomodulatory drugs for reducing MACE in patients with CHD, as well as related clinical indicators such as incidence of revascularization and angina. It also conducted a comprehensive analysis of the new immunomodulatory drug’s application on cytokines like hs-CRP and IL-6. This study synthesized evidence from 25 RCTs. The evidence indicates while the overall effect on MACE was not significant in CHD patients, the new immunomodulatory drugs could reduced incidence of angina, revascularization, IL-6 levels, neutrophil count levels, and improve the LVEF.
The overall analysis indicated that adding immunomodulatory drugs to standard therapy did not significantly reduce MACE incidence (RR = 0.92, 95% CI: [0.84, 1.01], P = 0.09). However, this null finding masks substantial heterogeneity. Subgroup analysis by drug class demonstrated NLRP3 inflammasome inhibitor (RR = 0.75, 95% CI: [0.65,0.86], P < 0.0001) and IL pathway inhibitors (RR = 0.88, 95% CI: [0.80,0.97], P = 0.009) significantly reduced MACE, whereas broad-spectrum immunomodulator showed no benefit. These dichotomous data suggested that effect may changed with different anti-inflammatory pathway. Furthermore, a treatment duration exceeding six months was necessary to observe a significant MACE reduction (RR = 0.89,95%CI: [0.82,0.98], P = 0.01). indicating that sustained immunomodulation is required for clinical benefit. In contrast, disease classifications (ACS vs. CCS) did not affect outcomes, which demonstrated the new immunomodulatory drugs have no benefits for all sorts of CHD patients.
The significant reduction in MACE with colchicine (RR = 0.75, 95% CI: [0.65, 0.86],P < 0.0001) are consistent with the COLCOT and LoDoCo2 trials, Colchicine is thought to stabilize atherosclerotic plaques by inhibiting NLRP3 inflammasome mediated production and neutrophil activity [8, 32]. By inhibiting neutrophil chemotaxis, adhesion, and activation of the NLRP3 inflammasome, colchicine can reduce the production of interleukin (IL)−1β and IL-18 [8]. Similarly, the clinical benefit of canakinumab (RR = 0.87, 95% CI: [0.81, 0.94], P = 0.0002) aligns with the CANTOS trial, confirming that blocking this upstream cytokine reduces vascular inflammation independent of lipid regulation [6]. These findings further support the mechanistic theory that targeting upstream inflammatory mediators (e.g., IL-1β, NLRP3) can block the pro-inflammatory cascades driving atherosclerosis. Conversely, the lack of benefit with methotrexate, Lp-PLA2 inhibitors, and p38 MAPK inhibitors is consistent with previous negative trials such as CIRT and SOLID-TIMI 52 [14, 28]. As broad or downstream anti-inflammatory strategies may fail to modulate key pathways of plaque destabilization. The other reason why the broad-spectrum immunomodulator, Lp-PLA2 inhibitor, and p38 MAPK kinase inhibitor showed no benefits in CHD patients is that the involved patients are not enough in quantity. It reminds us that require more RCTs about these drugs in CHD patients to provide sufficient statistics.
We suppose the efficacy of a drug is profoundly influenced by its molecular target within the complex cascade of coronary inflammation. We surprisingly found the effective drugs are targeting upstream, central inflammatory pathways, the upstream inhibition effectively dampens the entire subsequent inflammatory cascade (e.g., reduced IL-1β, IL-6, neutrophil count), leading to plaque stabilization and a significant reduction in MACE, as consistently shown in COLCOT and LoDoCo2 trials cited in our manuscript. However the ineffective drugs are targeting downstream or alternative pathways. The inflammatory cascade, once initiated upstream by NLRP3/IL-1β, may bypass the downstream pathway, or Lp-PLA2 inhibition may simply be insufficient to quell the established inflammatory response driving clinical events, and for p38 MAPK kinase inhibitors and broad-spectrum immunomodulators, their inhibition may be too broad yet not precise enough, or may be compensated by alternative pathways.
In our analysis, therapy of short term showed no benefit in reducing MACE (follow-up ≤ 6 months) may reflect delayed inhibition of neutrophil driven reperfusion injury, as indicated by the conflicting infarct size outcomes reported by Deftereos et al. and Mewton et al. [22, 26]. Notably, in Mewton’s trial, the association of colchicine with an increased risk of left ventricular thrombosis highlights its complex interaction with platelet activation and endothelial repair mechanisms, potentially mediated by microtubule-dependent thrombospondin-1 release [37].
This study still has several limitations. Firstly, the number of studies sample is not enough for Lp-PLA2 Inhibitors, p38 MAPK inhibitors, broad-spectrum immunomodulators, which limits the persuasiveness of subgroup comparisons; the lack of significant differences in reduction of MACE based on disease classification (acute vs. chronic coronary heart disease) may reflect insufficient statistical power due to small subgroup sample sizes rather than true therapeutic equivalence. Secondly, although including the latest trials could provide the latest data, excluding pre-2014 studies may omit historically relevant data. Thirdly, key prognostic variables for coronary artery disease are missing, left ventricular ejection fraction (LVEF) is a critical factor, yet only three studies report it. This degree of missingness is a major limitation that could materially affect the conclusions. Fourthly, some of the included original studies did not directly report the number of patients experiencing MACE—as predefined by us as a composite of cardiovascular death, non-fatal myocardial infarction, and non-fatal stroke—but instead reported the incidence of each component separately. when a study did not report the composite endpoint at all—but did provide separate, complete data for all three component events—did we sum the components to estimate the total number of MACE events. our method could overestimate the true number of patients with MACE.
This meta-analysis demonstrates that despite efficacy in different drugs and follow-up durations is not the same, some specific new immunomodulatory drugs but not all new immunomodulator can provide significant cardiovascular protection for patients with CHD. The other type of drugs do not have benefits may contribute to insufficient sample size. This result showed that we should carry out more researches to identify the effects of broad-spectrum immunomodulators, PhospholipaseA2 inhibitors and P38MAPK kinase inhibitors in CHD patients. Our meta analysis supports the concept of precise anti immunomodulatory therapy in CHD patients. Rather than applying a blanket “anti immunomodulatory” strategy, clinicians should prioritize drugs with proven efficacy and mechanistic rationale, specifically NLRP3 inflammasome inhibitors (e.g., colchicine) and IL-1β pathway inhibitors (e.g., canakinumab) should be considered for secondary prevention in CHD patients. Conversely, based on current evidence, broad-spectrum immunomodulators (e.g., methotrexate) and downstream inhibitors (e.g., Lp-PLA2 inhibitors, p38 MAPK inhibitors) should not be used in CHD patients, as they have not demonstrated significant benefit.
This meta-analysis provides evidence that supports the selective use of colchicine and IL-1 inhibitors in the secondary prevention of CHD, particularly in patients with high inflammatory burden and when used long-term. It is anticipated that future updates to ESC and AHA guidelines may strengthen recommendations for colchicine in both ACS and chronic coronary syndromes and provide more accurate guidance on IL-1 inhibition, potentially reserved for specific high-risk subgroups.
These findings reinforce the theory of inflammation as a modifiable cardiovascular risk factor and pave the way for precision medicine in atherosclerosis management.
Supplementary Information
Supplementary Material 1.