Clinical utility of Thromboelastography in patients with COVID-19: a prospective observational study
A. Deepak Sai, Ravindra Prithvishree, K. Nagesh Savan, Mohan Ganesh, Gupta Nitin, Kishore Asish, S. Nisarg, Chaudhuri Souvik, Paonam Bemma

TL;DR
This study shows that Thromboelastography (TEG) can predict mortality in COVID-19 patients by detecting early coagulation issues.
Contribution
The study demonstrates that hypocoagulable TEG results are a strong early predictor of 28-day mortality in COVID-19 patients.
Findings
45% of patients had abnormal TEG results, with 32% showing hypercoagulability.
Hypocoagulable TEG was associated with a 7.49 times higher risk of 28-day mortality.
Common thrombotic complications included stroke, myocardial infarction, and pulmonary embolism.
Abstract
Coronavirus disease (COVID-19) has been associated with thromboembolic and bleeding complications. Our study aims to understand the utility of early Thromboelastography (TEG) in the emergency department as a point-of-care test in predicting clinical outcomes. A prospective observational study was conducted in the emergency medicine department (ED) during June 2021- May 2022 with inclusion criteria of all patients above 18 years who arrived at the ED and had a positive COVID-19 RT PCR test. Hematological investigation, including TEG, was sent. Patients were followed up for 28-day mortality, thrombotic and bleeding complications. A total of 166 patients were enrolled in the study. 46% of patients had critical COVID-19. TEG was abnormal in 45% of patients. Hypercoagulability was seen in 32% of patients. 28-day mortality in our study population was 32.3%. The most common thrombotic…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
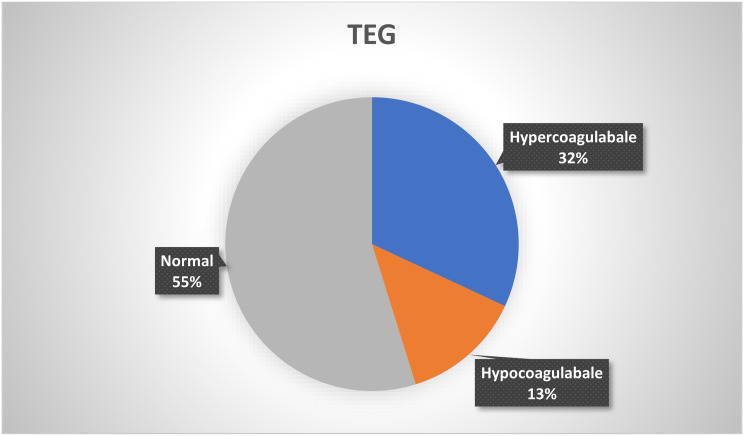 Figure 1
Figure 1- —Manipal Academy of Higher Education, Manipal
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTrauma, Hemostasis, Coagulopathy, Resuscitation · COVID-19 Clinical Research Studies · Sepsis Diagnosis and Treatment
Introduction
Coronavirus disease (COVID-19) is caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Since the diagnosis of the first case in December 2019, it has rapidly spread across the globe, leading to a profound public health problem, claiming millions of lives [1]. It primarily affects the respiratory system and presents as fever, cough, and shortness of breath. Additionally, it can also present as extrapulmonary manifestations, including cardiovascular, neurological, and thromboembolic complications [2]. Hypercoagulopathy in COVID-19 leads to thromboembolic complications such as pulmonary thromboembolism, deep vein thrombosis, stroke, and acute coronary syndrome. It affects multiple organs and can cause long term effects, which may lead to lifestyle modifications [3].
Thromboelastography (TEG) is a whole blood-based viscoelastic test used to evaluate the dynamic properties of blood coagulation. It provides a comprehensive analysis of the coagulation process by measuring interactions between plasma coagulation factors and cellular factors. Conventional coagulation tests like PT, APTT, platelet count, and fibrinogen concentration take significant time (45–60 min) and only measure individual components of the coagulation cascade, but TEG gives a real-time assessment of the entire coagulation process, including clot initiation, propagation, stabilization, and dissolution in lesser time (15–30 min). Detecting a hypercoagulable coagulation status is another advantage of TEG over conventional coagulation tests. It has been proven to be a valuable tool in managing coagulopathies in various clinical settings, including surgery, trauma, and liver disease [4].
The usefulness of TEG in COVID-19 has gained attention due to a predisposition for thromboembolic complications in COVID-19. COVID-19-associated coagulopathy (CAC) is characterized by a thrombotic condition predominantly observed in early phases of infection, with a cumulative incidence of thromboembolic events in CAC is around 30% [5, 6]. TEG could significantly identify hypercoagulability in COVID-19 patients, guide anticoagulant therapy, and improve clinical outcomes. The severe inflammatory state secondary to the infection leads to a derangement of hemostasis, typically observed in patients with sepsis and has been described as a state of acute disseminated intravascular coagulation (DIC) [7]. As the severity of the disease advances, a hypocoagulable picture is also observed with a hemorrhagic tendency because of widespread endotheliopathy, consumption of coagulation factors, and acidosis [8]. A systematic review by Hartman et al. demonstrated that TEG helps identify coagulation abnormalities earlier than standard tests, thus providing critical insights for tailored therapeutic interventions [9].
TEG monitors dynamic changes in coagulation parameters, which makes it helpful in managing COVID-19. As COVID-19 causes coagulation abnormalities that can lead to both thrombosis and bleeding manifestations, TEG can be a pivotal tool in the diagnostic and therapeutic arsenal against this multifaceted disease. Our study aims to understand the possible utility of early TEG in the emergency department as a point-of-care test predicting clinical outcomes such as thromboembolism, bleeding, and mortality.
Methodology
We conducted a prospective observational study in a tertiary care center in South India from June 2021 to May 2022. Approval from the Institutional Ethics Committee was obtained, and the trial was registered under CTRI [CTRI/2021/09/0362275] before the recruitment of patients. Assuming the prevalence of hyper coagulopathy among COVID-19 patients as 31% (Salem et al.) [10] with a confidence interval of 95% and a margin of error of 7.5%, the estimated sample size was 147 patients.
All patients above 18 years who arrived in the Emergency Department and were confirmed COVID cases by a positive COVID-19 RT PCR (nasal or throat) during the study period were included. Patients with pre-existing coagulation disorders were excluded.
The data was collected after obtaining consent from the patient or their legally acceptable representatives. Demographic data of all the included patients, including age, comorbidities, and medications, were documented after interviewing the patient or their relatives. Patient’s vital signs [heart rate, systolic and diastolic blood pressure, room air saturation], requirement of oxygen support, and presence of shock at admission were noted. Hematological investigations, such as Complete blood count, D-dimer, Prothrombin time, Activated Partial Thromboplastin Time, and TEG [TEG 500, Hemonetics, USA] were sent at the time of admission, the results of which were recorded. The NIAID ordinal scoring system was documented at admission and at the time of final disposition of the patient. Charlson’s comorbidity index was calculated. Treatment during the hospital stay was recorded. Based on the history from the interview, the patients with pre-existing coagulation disorders were excluded.
The outcomes of the patients were recorded as death, discharge, or discharge against medical advice. Duration of hospital stay and number of days of ICU stay (if any) were also calculated. The presence of thrombotic complications was considered if the patients had a new onset of Myocardial infarction as defined by the fourth universal definition of myocardial infarction [11], or had imaging evidence of deep vein thrombosis, acute pulmonary thromboembolism, or stroke. Thromboembolism risk estimation was assessed by the serial Doppler and Echo. They were done on admission and on day 5 or when it was feasible. The presence of Upper gastrointestinal bleeding, Pulmonary hemorrhage, hematuria, hemothorax, retroperitoneal hemorrhage, and intracranial bleeding during their hospital stay was taken as the presence of bleeding complications. Patients were then followed up for 28 days post-admission via telephonic interview to look for complications such as death, readmission, thrombosis, or bleeding. If the patients were admitted to another hospital during the 28 days post-discharge, details would be collected from the discharge summary.
Statistical analysis
The categorical variables were summarized as percentages, and continuous variables as mean (with standard deviation) or median (with interquartile range). The included patients were categorized into two groups based on whether they developed thrombosis. The two groups’ TEG parameters, clinical profiles, and outcomes were compared. The t-test was used for continuous variables, and the Chi-square test was used for categorical variables. A p-value of less than 0.05 was considered significant.
Results
A total of 166 patients who met the inclusion and exclusion criteria between June 2021 and May 2022 were enrolled in the study. Of these, 70% were male. The median age of the patients was 61.8 years (± 15.5). The median Charlson Comorbidity score was 4 (IQR 2-6.25). The patients presented to the emergency department a median of 3 days (IQR 2-5.25) after the onset of symptoms. The mean NIAID score at admission was 4.3 (± 0.7) among the study population. One-fifth of the patients (20%) were in shock and required vasopressors upon admission, as seen in Table 1. Based on the WHO severity score, 46% of patients had critical COVID.
A total of 13 patients had regional wall motion abnormalities on the day of admission. Eleven patients had right atrium and right ventricular dilatation, and two patients had DVT on the day of admission. PT and APTT were deranged in 5 patients. Platelet count was < 1,00,000 in 36 patients. Among 166 patients, 33% had elevated D-dimer levels at admission.
Table 1. Demographic and clinical details at the time of admission of patients enrolledVariablesValues [ %]Mean Age61.8+/-15.5GenderMale 117 (70%)Female 49 (30%)Median onset of symptoms3 Days (IQR 2-5.25) Comorbidities HTN102 (60%)DM101 (60%)CKD35 (21%)IHD34 (21%)Heart failure29 (17%)CVA24 (14%)COPD19(11%)Asthma8(4%)Septic shock35 (20%) WHO category at admission Critical78 (46%)Severe37 (22%)Moderate33 (19%)Mild18 (10%) NIAD score at Admission 31 (1%)4130 (78%)519 (11%)613 (7%)73 (1%) Prior Antiplatelets usage No antiplatelets127 (76%)Single antiplatelets28 (16%)Dual antiplatelets11 (2%)Prior Anticoagulant usage4 (2%)Abbreviations: HTN: Hypertension; DM: Diabetes Mellitus; CKD: Chronic Kidney Disease; IHD: Ischemic Heart Disease; CVA: Cerebrovascular Accident; COPD: Chronic Obstructive Pulmonary Disease; WHO: World Health Organization; NIAID: National Institute of Allergy and Infectious Diseases; IQR: Interquartile Range
Among 166 patients, TEG was abnormal in 75 patients (45%). Hypercoagulability was seen in 1/3rd (32%) of patients, and the TEG was hypo-coagulable in 22 patients as described in Fig. 1. In 16 patients, TEG showed fibrinolysis, among which 11 patients showed secondary fibrinolysis, and 5 showed primary fibrinolysis. Out of 15 cases showing thrombotic complications, TEG was hypercoagulable in 40% of the patients, and secondary fibrinolysis was seen in 4 patients. Anticoagulation was started for 126 out of 166 patients. Low molecular weight heparin was initiated for 76 patients, and the remaining were started on heparin. Antiplatelet drugs were started in all the patients with thrombosis and 78% without thrombosis. Among patients with previous anticoagulation and antiplatelet usage, TEG was hypercoagulable in 1 patient (1 out of 4) and 14 patients (14 out of 39), respectively. Only 4 patients with previous antiplatelet usage and 1 with previous anticoagulation usage have hypocoagulable TEG.As noted in Table 2, the TEG parameters of the COVID-19 patients were compared with the institutional reference range.
Fig. 1. Distribution of TEG among the study population
Table 2TEG parameter of COVID-19 study patients with institutional reference rangeInstitutional Reference valueCOVID-19 study populationParameterMean [SD]RangeMean [SD]RangeR time6.22(1.77)3.3–10.64.3 [1.9]1.3–14K Time2.00(0.44)1.2–3.21.85[1.36]0.8–10.2Alpha angle61.26(5.9)54.9–7265.9[12.3]4.6–85MA55.45(5.93)51.2–62.661.8[10.4]8.8–79.5LY303.14(3.17)0–104.67[10.7]-0.2-59.8CI− 0.17(1.47)-2.1-3.21.8[3.23]0-3.2Patient samples were compared with the institutional reference rangeAbbreviations: R time -reaction time, MA: maximum amplitude, LY30: lysis at 30 min, CI -clot index.SD- standard deviation
As noted in Table 3, Among 166 patients, 60% were discharged from the hospital, 27% died, and 13% went against medical advice from the hospital. A telephonic follow-up was done for the patients to assess the 28-day mortality. Twenty-eight-day mortality in our study population was 32.3% (53/164, 2 were lost to follow-up). Among 166 patients, thrombotic complications were seen in 15 patients. The most common thrombotic complications were stroke (7, 4.2%), followed by myocardial infarction (6, 3.6%), pulmonary embolism (2, 1.2%), and DVT (1, 0.6%). In the study population, 19 patients had bleeding manifestations, of which 13 patients developed bleeding following initiation of anticoagulation.
Table 3. Outcome of study populationIn-Hospital Outcomesn (%)Death46 (27%)Discharge99 (60%)Discharge against medical advice11 (13%) 28-day mortality 53/164 (32.3%) THROMBOSIS Stroke7 (4.2%)MI6 (3.6%)PE2 (1.2%)DVT1 (0.6%) BLEEDING Hematuria6 (3.6%)Upper GI bleed4 (2.4%)Pulmonary hemorrhage3 (1.8%)Soft tissue hematomas2 (1.2%)Intracranial bleed1 (0.6%)MI: Myocardial infarction, PE: pulmonary Embolism, DVT: Deep Vein Thrombosis, GI Bleed: Gastrointestinal Bleed
As noted in Table 4, we found that a higher total count and platelet count were associated with a higher incidence of thrombosis among the laboratory parameters. Among the patients with thrombosis, TEG was normal in 9 patients and hypercoagulable in the remaining patients. In our study, the TEG parameters did not significantly predict thrombotic complications.
Table 4. Factors associated with thrombotic events in COVID-19 patientsThrombosis (N = 15)No thrombosis (N = 151)p-valueAge68.1 ± 1161.1 ± 15.70.096Male12(80%)105(69.5%)0.397Septic shock at admission6(40%)29(19%)0.06ComorbiditiesDiabetes10(66.7%)91(60%)0.628Hypertension12(80%)90(59.6%)0.122Chronic kidney disease4(27.7%)31(20.5%)0.578Prior stroke2(13.4%)22(14.5%)0.897Heart failure5(33.4%)24(15.8%)0.09Ischemic heart disease5(33.4%)29(19.2%)0.196Chronic obstructive pulmonary disease2(13.4%)17(11.2%)0.81Asthma08(5%)0.361Previous COVID01(0.6%)0.752Received prior COVID vaccination9(60%)78(51.6%)0.554 TEG at admission Hypercoagulable6(40%)47(31.1%)0.482Hypocoagulable022(14.5%)0.112Primary Fibrinolysis1(6%)4(2%)0.385Secondary Fibrinolysis1(6%)10(6%)0.995R3.9 ± 1.24.4 ± 20.356K1.5 ± 0.71.9 + 1.40.339Alpha66.9 ± 7.565.8 ± 12.70.730MA64.6 ± 8.661.6 ± 10.60.284G9.9 ± 3.88.9 ± 3.20.220Other laboratory parametersTC14,500 + 940010,200 ± 58000.011Platelets2.66 ± 1.12.1 ± 10.046INR1.15 ± 0.351.14 ± 0.340.840aPTT29.6 ± 5.132.9 ± 7.50.091D-dimer3.4 ± 3.32.9 ± 3.10.59Outcomes28-day mortality3(20%)50(33.1%)0.345Abbreviations: R time -reaction time, MA: maximum amplitude, TC: Total white blood cell count, international normalized ratio, aPTT- activated partial thromboplastin time
Factors associated with 28-day mortality are analyzed and represented in Tables 5 and 6.
Table 5. Factors associated with death and survival on 28-day follow-up [ n = 164]DeathSurvivorsp-valueOverall53(35%)111(65%)Age60.83 ± 16.862 ± 150.096Female9(16.9%)38(34.2%)0.3Septic shock at admission19(35.8%)16(14.4%)0.003 TEG at admission Hypercoagulable15(28.3%)37(33.4%)0.640Hypocoagulable12(22.6%)9(8%)0.019Primary Fibrinolysis4(7%)1(0.9%)0.067Secondary Fibrinolysis5(9%)6(5%)0.528R4.68 ± 2.34.19 ± 1.60.182K2.22 ± 1.71.67 ± 1.10.039Alpha63.3 ± 13.667.2 ± 11.50.085MA60.4 ± 1162.6 ± 9.80.224G8.63 ± 3.89.13 ± 2.80.159Other laboratory parametersTC10,87710,5240.762PLt1.98 ± 12.22 ± 0.90.161INR1.28 + 0.491.08 + 0.20.007aPTT34.21 ± 7.731.7 ± 7.10.081D-dimer2.37 ± 2.31.97 ± 20.36
Table 6. Factors associated with 28-day mortality using logistic regression analysisParametersOdds ratios [CI]P valueTEG [Hypercoagulable]1.33[0.51–3.45]0.556TEG [Hypocoagulable]7.49[1.06–54.5]0.042Septic shock2.18[0.88–5.44]0.091WHO category [critical]31.85[4.59–695]0.004WHO Category [severe]8.30[1.05–187]0.083
As seen in Table 6, logistic regression analysis for the 28-day mortality shows that patients who had hypocoagulable TEG had a higher 28-day mortality with septic shock and WHO Category were taken as confounders.
Discussion
In our observational study assessing the clinical utility of TEG in patients with COVID-19 presenting to the emergency department, we found that TEG at admission was not predictive of thrombotic or bleeding complications. The TEG profile of COVID-19 patients suggests that 32% were hypercoagulable, and 13% were hypocoagulable. The hypercoagulable picture was defined as CI >3 with either of the following: normal or shortened R and K time, increased alpha angle, and MA, and a hypo coagulable state was defined as CI < − 3 with either one of the following: prolonged R and K time, decreased alpha angle and MA, as per a previous study based on a similar population [11]. A hypercoagulable state is commonly seen in patients with COVID-19. Saseedharan et al., in their study, demonstrated an incidence of 62.5% hypercoagulable TEG in patients with moderate to severe COVID-19 admitted to the ICU [13]. Similarly, Maatman et al. had a 50% incidence of hypercoagulable TEG in patients with severe COVID-19 [14]. Panigada et al. also demonstrated a hypercoagulable state in patients intubated due to COVID-19 (raised MA in 87% and low Lys-30 in 100%) [15]. The hypercoagulable state is seen more with severe COVID-19 and may persist even in the presence of anticoagulation medication. The lower number of patients in our study with altered coagulation profiles as identified with TEG could be due to the following reasons: (a) we had a mix of both moderate and severe COVID-19, (b) since only one TEG value was sent on the day of admission, (median 3 days since onset of symptoms), we may have missed any ongoing changes in TEG during the illness.
We had a higher incidence of primary and secondary fibrinolysis (3% and 6%). It was similar to the study by Pazzi et al. showed that hypo fibrinolysis rather than hypercoagulability seems to be associated with poor and adverse outcomes [16]. Incidence of thrombotic events in our study was 9%, which was similar to Lodigiani et al. i.e., 7.7% [17]. Our study showed that common thrombotic complications were stroke, followed by myocardial infarction, pulmonary embolism, and DVT, which was similar to the systematic review by Hartmann et al. 2022 [9].
We didn’t find any statistically significant correlation between the incidence of thrombosis and the presence of a hypercoagulable state on TEG. The use of TEG to predict thromboembolism or mortality is not yet fully proven. Salem et al. also found no correlation between a hypercoagulable state and the incidence of thromboembolic phenomenon [10]. Duenas et al., in their retrospective study on 134 critically ill COVID-19 patients, found no benefit of TEG-guided anticoagulation protocol in reducing death, major bleeding, or thrombosis [18]. Marvi et al. found that low Maximum Amplitude (MA) in serial TEG measurements in critically ill COVID-19 patients was associated with a higher risk of venous thromboembolism [19]. Similarly, Zhong et al., in their observational study, found an increased Maximum Amplitude to be associated with higher mortality [20].
There could be many reasons why we didn’t find any significant correlation between Thrombotic events and TEG parameters. Firstly, we only measured TEG at admission. Secondly, most patients were on prophylactic or therapeutic anticoagulation during their admission. Also, we included both arterial and venous thromboembolic complications as a single composite, even though they have different pathologies due to their similar clinical implications.
With regards to bleeding complications, we had 16 patients (9.6%) with various complications such as Upper GI bleed, pulmonary hemorrhage, and Intracranial bleeding. In a recent systematic review and meta-analysis of 49 studies and >18,000 patients by Jiménez et al., there was a pooled incidence of 7.8% (95% CI, 2.6–15.3) for bleeding and 3.9% (95% CI, 1.2–7.9) for significant bleeding [21]. The cause of bleeding could be primarily due to COVID-19-associated coagulopathy or due to confounding factors such as the use of anticoagulants, steroids, and prolonged ICU stay. Similarly, Parks et al., in their observational study, found 5-fold increase in the risk of bleeding secondary to anticoagulation [22].
Our study has shown that there was a correlation between the Hypocoagulable TEG [ odds ratio 7.49] with the mortality at 28-day mortality, which was similar to other studies such as Mohan et al. [12] and Blasi et al. [23]. Multivariable Logistic regression analysis about the factors affecting mortality showed that hypo-coagulability was 7.49 times affect mortality, which was similar to Al Sankari et al. [24]. Kong et al. [26] and Adamzink et al. [25] showed that TEG showing hypo-coagulable and septic shock showed increased mortality. As the disease progressed, TEG profiles of the COVID-19 patients shifted towards hypo-coagulability, which was associated with poor prognosis and increased mortality. The proposed hypothesis for the hypocoagulable TEG in some cases of Severe COVID-19 is due to reduced thrombin generation, which results in COVID-associated coagulopathy [CAC]. It is considered similar to the development of coagulopathy in other consumptive coagulopathies like sepsis-induced coagulopathy [5, 8, 15]. Patients with severe metabolic acidosis and septic shock also have reduced thrombin generation. As the disease severity of COVID-19 progresses, it will lead to a stage of complete cellular shutdown [27]. Further studies are required to confirm this proposed hypothesis.
The implications of sending TEG early helps in deciding the requirement of anticoagulation dose starting based on case to case basis. Findings from a randomised control trial on the effect of anticoagulation dose in patients with severe or critically ill patients showed that there were increased bleeding manifestations in critically ill patients and the enrolment of the critically ill patients were suspended [28]. Hypocoagulable TEG and anticoagulation dose were to be decided on the risk vs. benefit ratio and further studies were required.
This study was one of the few prospective studies looking for venous and arterial thrombotic and bleeding complications in COVID-19 patients. We also tried to assess the benefits of sending TEG early, directly from the emergency department as a point-of-care test, which was not done previously, as the remaining studies were done in the ICU. There are a few limitations to our study. Ours was a single-center observational study, limiting its generalizability to larger populations. The COVID variant was not identified in our patients. Different variants of the COVID-19 virus could have other types of effects on the coagulation and might have confounded our findings. Patients on antiplatelet or anticoagulant therapy were not excluded from the study.
Conclusion
COVID-associated coagulopathy can be associated with both thrombotic (venous and arterial) and bleeding complications. Hypocoagulability on initial TEG has a 7.49 times increased risk of mortality. Hypocoagulable TEG indicates an early predictor for mortality. Early TEG can be an essential tool in managing COVID-associated coagulopathy.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary Material 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The true death toll of COVID. -19 estimating global excess mortality [Internet]. [cited 2024 Nov 23]. Available from: https://www.who.int/data/stories/the-true-death-toll-of-covid-19-estimating-global-excess-mortality
- 2Fourth Universal Definition of Myocardial Infarction. (2018) | Circulation [Internet]. [cited 2024 Nov 23]. Available from: https://www.ahajournals.org/doi/10.1161/CIR.0000000000000617
- 3Maatman TK, Jalali F, Feizpour C, Douglas A, Mc Guire SP, Kinnaman G, et al. Routine venous thromboembolism prophylaxis may be inadequate in the hypercoagulable state of severe coronavirus disease 2019. Crit Care Med. 2020;10.1097/CCM.0000000000004466.10.1097/CCM.0000000000004466 PMC 730208532459672 · doi ↗ · pubmed ↗
- 4Pazzi M, Conti D, Tofani L, Zanfino L, Gemmi E, Pasquinelli F, et al. Impact of Rotational Thromboelastometry (ROTEM) on Clinical Course and Outcomes of COVID-19 Critically Ill Patients: a retrospective single center observational study [Internet]. Research Square; 2023 [cited 2024 Nov 23]. Available from: https://www.researchsquare.com/article/rs-2065618/v 1
- 5Zhong L, Lin Q, He L, Liu D, Zhu L, Zeng Q, et al. Time to the maximum amplitude of thromboelastography can predict mortality in patients with severe COVID-19: a retrospective observational study. Front Med [Internet]. 2024 May 2 [cited 2024 Sep 9];11. Available from: https://www.frontiersin.org/journals/medicine/articles/10.3389/fmed.2024.1356283/full 10.3389/fmed.2024.1356283 PMC 1109711138756947 · doi ↗ · pubmed ↗
- 6Blasi A, von Meijenfeldt FA, Adelmeijer J, et al. In vitro hypercoagulability and ongoing in vivo activation of coagulation and fibrinolysis in COVID-19 patients on anticoagulation. J Thromb Haemost. 2020;18:2646‐2653. [DOI] [PMC free article] [Pub Med] [Google Scholar].10.1111/jth.15043 PMC 743662732762118 · doi ↗ · pubmed ↗
- 7National Institutes of Health. NIH ACTIV trial of blood thinners pauses enrollment of critically ill COVID-19 patients. Available at: https://www.nih.gov/news-events/news-releases/nih-activ-trial-blood-thinners-pauses-enrollment-critically-ill-covid-19-patients. Accessed Febuary 9, 2021.