Staying engaged: a scoping review of psychological and motivational drivers of adherence to technology-supported physical activity in older adults
Sven J. G. Geelen, Tiia Kekäläinen, Mary Hassandra, Karen Feyen, Solveig A. Arnadottir, Salit Bar Shalom, Yael Netz, Erja Portegijs, David Beckwée

TL;DR
This review explores what motivates older adults to stick with technology-based physical activity programs, highlighting factors that help or hinder their engagement.
Contribution
The study differentiates between adherence to physical activity and technology use, identifying psychological and motivational factors specific to each.
Findings
Key facilitators for adherence include ease of use, personalized content, and social support.
Barriers include low digital literacy and repetitive content in technology-based interventions.
12 out of 19 psychological/motivational variables showed statistically significant associations with adherence outcomes.
Abstract
As populations age, maintaining physical activity (PA) is essential to reduce chronic disease risk and preserve functional independence in older adults. Technology-supported interventions, such as wearables, mobile applications, and web-based platforms, have emerged as effective tools to promote PA. However, engagement with technology alone is not sufficient. Effectiveness depends on whether digital tools foster sustained adherence to prescribed PA, since health benefits are dose-dependent on activity levels. In this sense, adherence matters not just for short-term participation but for embedding long-term behaviour change, an especially pressing challenge for older adults, who are typically less active and may experience greater barriers to digital engagement. This scoping review aimed to identify psychological and motivational factors that influence adherence to both the physical…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
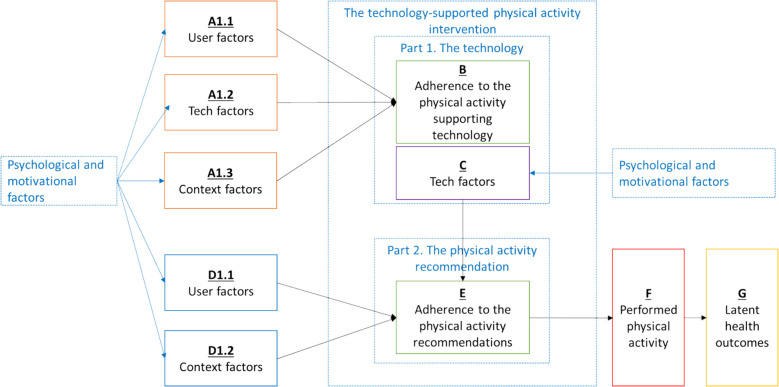 Figure 1
Figure 1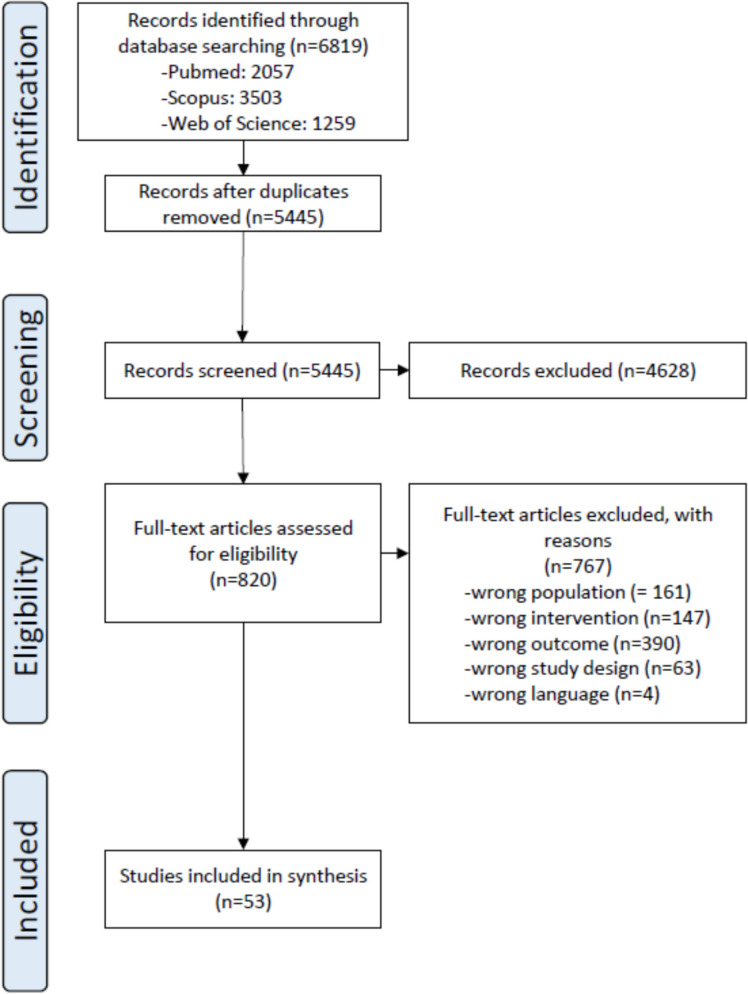 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPhysical Activity and Health · Technology Use by Older Adults · Innovative Human-Technology Interaction
Introduction
As the global population ages rapidly, maintaining physical activity (PA) among older adults is crucial for preventing age-related functional decline and chronic diseases [1]. Since there is a well-documented dose–response relationship between PA and health outcomes, maintaining adherence to the recommendations is especially crucial [2]. However, there remains limited understanding of how the factors driving adherence are embedded within current technology-supported PA programs, or how their effectiveness varies across different individuals and contexts. This is especially important for older adults, who often face unique challenges such as declining cognitive and physical function [3], lower digital literacy [4], and varying motivational needs [5]. These factors must be considered within the field of gerontechnology—the interdisciplinary study of technology to support ageing—which seeks to design interventions tailored to older adults’ abilities and preferences [6]. Without such insights, digital solutions may fail to promote sustained adherence in this growing and diverse population.
Adherence to PA is understood as the extent to which individuals complete the prescribed activities, as outlined in a program or recommendation. This is typically expressed through the FITT dimensions: Frequency, Intensity, Time, and Type of the physical activity. Adherence rates are generally higher in supervised PA programs [7] and in well-controlled research studies. Moreover, it is known that adherence is harder to achieve over the long-term as human behaviour is resistant to change, and relapsing into previous habits is common over time [8]. In real-world settings, community-based programs often lead to more modest PA gains due to less rigorous strategies to reach and retain participants and support program adherence, combined with greater heterogeneity in participants and participant responses, than programs executed in research settings [9–11].
In general, barriers to and facilitators of PA include factors related to the individual and the environment [12, 13]. Factors related to the program as well as the individual have been suggested to impact adherence to PA programs and recommendations [12–15]. Among these, motivation, intention, automatic processes, habitual actions, and goal-directed behaviours play a central role in influencing the adherence [16]. Motivation plays a key role in the adoption and maintenance of PA and is shaped by psychological factors, which encompass cognitive (e.g., thinking, reasoning), affective (e.g., emotions, feelings), and social (e.g., social and environmental influences, perceptions, interactions) dimensions [17, 18]. Utilizing psychological and motivational support strategies may therefore enhance adherence to PA programs and recommendations through self-determined motivation [16]. Indeed, studies have shown that PA programs using behaviour change techniques, in addition to the primary PA component, may lead to larger gains and improved program adherence, especially for those without a physically active approach in life[19].
Over the past decades, a growing array of technologies has been developed and implemented to facilitate and support the delivery of PA programs for older adults [20, 21]. Technology-assisted PA programs involve the use of technology as a tool to support or enhance adherence to, or the outcomes of, PA interventions, in line with the WHO definition of technology-assisted approaches [22]. Technologies which remotely support and monitor PA (e-health, m-health, and wearable solutions) may increase the reach of PA programs, and also provide opportunities for tailoring programs [23]. In addition, progress self-monitoring and digital interactive elements have been proposed as strategies to enhance adherence to PA programs and recommendations [24]. Yet, a previous review showed that adherence to technology-assisted exercise programs was higher compared to traditional exercise programs; however, details about adherence were lacking, and most studies were of a pilot nature [25].
Adherence in technology-assisted PA interventions involves both sustained participation in the PA and continued engagement with the supporting technology. This distinction is critical, as the technological component plays a dual role—not only as a delivery mechanism (e.g., exercise sessions via a mobile app) but also as a behavioural target requiring its own engagement strategies (e.g., consistent app usage, syncing wearable devices, responding to prompts). In this context, the level of adherence with technology in technology-assisted programs underscores that technology itself can be a determining factor in the effectiveness of PA interventions.
The PhysAgeNet Cost Action network was established to address specific challenges related to evidence-based PA interventions in old age, including those related to the use of technology [26, 27]. In this context the current scoping review was performed, aiming to systematically search and explore key psychological and motivational factors that drive older people’s adherence to PA programs and adherence to technologies in technology-supported PA programs. A scoping review design was chosen because the field is still emerging, the evidence is highly heterogeneous in terms of study design and outcomes, and the purpose was to map the breadth of available evidence rather than to conduct a narrow or quantitative synthesis.
Methods
The protocol for this scoping review was pre-registered with the Open Science Framework (OSF) (10.17605/OSF.IO/SA2EM). The review was conducted following the methodological guidance of the Joanna Briggs Institute (JBI) [28] and reported in accordance with the PRISMA extension for scoping reviews (PRISMA-Sc-R) [29].
Search strategy
The search strategy was collaboratively developed by five authors (DB, EP, MH, TK, and YN) and an Information Specialist (BL). Searches were conducted in Medline (via PubMed), Web of Science and Scopus in March 2023, covering studies published from 2000 up to March 1, 2023. The year 2000 was chosen as a starting point because digital and mobile technologies for supporting PA interventions only became widely available in the early 2000 s, making earlier publications less relevant. Filters were applied to limit results to English-language publications to ensure accurate interpretation and consistency in data extraction, as translation was beyond the project’s resources. Review articles were excluded to focus on primary studies reporting original data, while systematic reviews were considered separately during interpretation. The search strategy was composed of four primary elements: (1) older adults, (2) physical activity, (3) technology, and (4) adherence. The full search strings for each database are presented in Appendix 1.
Screening process
The screening and data extraction processes were based on NICE guidelines [30] and PRISMA [29]. A screening tool defining the eligibility criteria was developed prior to the data searches and refined after pilot testing. In summary, qualitative, quantitative, and mixed-method studies were included if they examined technology-supported physical activity interventions and explored how psychological or motivational factors influenced adherence with the technology. A detailed overview of the eligibility criteria is presented in Table 1 of Appendix 2. In brief, studies were included if the mean sample age was ≥ 60 years and the minimum age was ≥ 50 years. Physical activity was broadly defined to include aerobic, strength, balance, flexibility, or multi-component programs, in line with WHO recommendations. Interventions were required to be technology-assisted, incorporating digital, electronic, or automated components (e.g., wearable devices, mobile or tablet applications, web-based platforms, interactive video programs, telehealth systems, or exergaming). Technologies could act as a primary delivery tool or be combined with human-delivered elements (e.g., tele-coaching or social components). Studies had to include an intervention period and report adherence outcomes, defined as either adherence to the PA program (using FITT principles: Frequency, Intensity, Time, and Type) or adherence to technology use (e.g., wear time, log-ins), rather than merely reporting study attrition. Ten reviewers (BAK, DB, EP, JH, KF, MC, SA, SJGG, TK, YN) conducted the screening process using the Rayyan software (https://www.rayyan.ai/). The screening procedures occurred in two stages: titles and abstracts were reviewed independently in blinded pairs, followed by a consensus discussion within each pair after unblinding, with a third reviewer assisting as needed. The same process was applied for full-text articles, with any disagreements similarly resolved in discussion with a third reviewer when required.Table 1. Qualitative research data: overview of the thematic analysisThematic groupDefinition of the groupNumber of factorsExampleCategory 1: User factors that relate to technology adherenceAttitudes, Expectations and Knowledge about TechnologyThis theme encompasses a wide range of feelings, beliefs, and past interactions related to technology. It includes both positive aspects like excitement and comfort, and negative aspects like fear, anxiety, and dislike. It also covers experiences with using technology, including prior knowledge, skill levels (from tech-savviness to inexperience), and difficulties encountered. Essentially, this theme captures how people feel and interact with technology22Anxiety about technical problems during exercise sessions decreases the level of technology adherencePerceived Social Impact of TechnologyThis theme focuses on how people believe technology affects their social connections and interactions. It includes perceptions of both positive impacts, such as reducing loneliness and facilitating social connection, and negative impacts, such as feeling judged during online interactions or the fear of technology replacing face-to-face contact. It also includes the experience of using technology to manage social interactions, such as being able to hide in online groups3Being less visible in an online setting increases the level of technology adherencePhysical Limitations and Technology UseThis theme addresses the challenges people face when physical health conditions or limitations affect their ability to use technology, especially apps or devices designed for physical activity or health monitoring. It recognizes that physical limitations can create barriers to effective technology use2Having a physical health condition decreases the level of technology adherenceCategory 2: Tech factors that relate to technology adherenceClear InformationClear Information" refers to the presence of accurate, relevant, and well-structured content within a technology system that supports user understanding, decision-making, and engagement. This theme encompasses both the clarity and sufficiency of instructions, visual or text-based guidance, and topic-specific content. It highlights how well technology communicates expectations, provides structured explanations, and avoids ambiguity that may lead to confusion or disengagement9Inconsistent instructions decrease the level of technology adherenceEase of Use & Accessibility"Ease of Use & Accessibility" refers to the degree to which technology is intuitive, user-friendly, and readily available for older adults. This theme encompasses both usability factors—how easily individuals can navigate, operate, and integrate technology into their daily routines—and accessibility factors—ensuring that technology accommodates diverse needs, physical abilities, and technological proficiencies20Experiencing difficulties in using the tech decreases the level of technology adherenceExercise programme content"Exercise Programme Content" refers to the structure, variety, and appropriateness of exercise routines and features provided within a technology-assisted exercise program. This theme highlights how well the program aligns with users' physical, cognitive, and motivational needs, ensuring an engaging and effective experience. The effectiveness of an exercise program depends on its evidence-based foundation, adaptability to diverse users, and ability to sustain motivation while promoting physical activity adherence10Being able to choose from a variety of exercises increases the level of adherence to technologyFeedback & Goal Setting"Feedback & Goal Setting" refers to the ability of technology to support users in monitoring progress, setting personal goals, receiving meaningful feedback, and tracking physical activity (PA) and health indicators. This theme highlights how well the system provides motivational, real-time, and data-driven insights that facilitate adherence, self-regulation, and long-term adherence to an active lifestyle57Being able to formulate goals in the tech increases the level of technology adherenceMotivation & Joy"Motivation & Joy" refers to factors that influence users' willingness to engage with technology-assisted physical activity. This theme captures the role of intrinsic and extrinsic motivators, including competition, gamification, reminders, and enjoyment, in sustaining adherence and adherence to exercise programs. The presence of positive experiences, challenges, and reinforcement mechanisms can enhance motivation, while barriers such as boredom, repetitive elements, and lack of interest may hinder long-term participation28Providing reminders increases the level of technology adherencePersonalization"Personalization" refers to the ability of technology to adapt to individual needs, preferences, and changing life circumstances to enhance user adherence, effectiveness, and engagement. This theme highlights how well a system tailors its content, feedback, scheduling, and exercise progression to suit the diverse requirements of users. A personalized approach ensures that technology-assisted interventions are meaningful, relevant, and aligned with individual goals and abilities11Tailoring the technology to the age of the user increases the level of technology adherenceSetting (home, outdoor,…) & planning"Setting (Home, Outdoor,…) & Planning" refers to the role of location, accessibility, and scheduling in shaping users' adherence to technology-assisted exercise programs. This theme highlights how the exercise environment (home, remote, outdoor, or hybrid settings) and planning mechanisms influence participation, flexibility, and adherence7Ability to train at home increases the level of technology adherenceSocial Interaction & Support"Social Interaction & Support" refers to the role of peer engagement, competition, healthcare communication, and remote assistance in shaping users' experiences with technology-assisted exercise programs. This theme highlights how technology can enhance or hinder social connectivity, motivation, and feelings of support by providing opportunities for interaction, feedback, and assistance25The possibility to message other users through the technology increases level of technology adherenceTechnical & Operational Challenges"Technical & Operational Challenges" refers to barriers and difficulties associated with the functionality, reliability, and usability of technology in supporting physical activity (PA) adherence. This theme highlights the limitations and frustrations users experience due to hardware issues, software malfunctions, connectivity barriers, and maintenance concerns, which can negatively impact adherence and trust in technology27Inability to track all activities decreases the level of technology adherenceTechnology Design & Usability"Technology Design & Usability" refers to the visual, functional, and interactive qualities of technology that influence ease of use, user comfort, and adherence. This theme highlights how well technology is designed to enhance user experience, support seamless interaction, and accommodate various user needs, while also identifying limitations or usability issues that may hinder effectiveness33Technology that is waterproof increases the level of technology adherenceCategory 3: Context factors that relate to technology adherenceContextual FactorsThis theme encompasses external circumstances and situations that can influence adherence to the intervention. It includes factors like exercising outdoors (the environment), participating in a research study (the context of involvement), and the impact on caregiver burden. This theme focuses on how the surrounding circumstances and broader context of the intervention can affect participation3Being able to use the technology outdoors increases the level of technology adherenceFactors Related to the Application and TechnologyThis theme addresses issues arising from the use of technology, specifically the application and activity tracker. It covers aspects like losing interest in the app over time, lack of access to necessary technology, and losing the activity tracker itself. This theme highlights how practical issues related to the technology can affect participation3Getting bored over time with the application decreases the level of technology adherenceSocial Influences on EngagementThis theme centres around the impact of social connections and interactions on participation in the intervention. It includes the influence of family members, the experience of group exercise, the presence of workout partners, and the role of technology in fostering social bonding. This theme emphasizes how social dynamics and relationships can motivate or hinder adherence6Assistance from family members with using the technology increases adherence to the technologySupport and Training Related to the InterventionThis theme focuses on the role of guidance, instruction, and support provided to participants in the intervention. It encompasses the initial training received, the availability of qualified trainers, ongoing counselling or support, and any perceived lack of guidance. This theme highlights how the quality and availability of support and training can influence engagement and success with the intervention6Brief training and instructions at the start increases the level of technology adherenceCategory 4: User factors that relate to physical activity intervention adherenceBeliefs, Attitudes, and Perceptions Related to Physical ActivityThis theme encompasses an individual's thoughts, feelings, and opinions about physical activity. It includes their beliefs about the benefits of exercise, their overall attitude towards being physically active (positive or negative), and their perceptions of social expectations regarding physical activity. This theme focuses on the cognitive and emotional aspects of how someone thinks and feels about physical activity, rather than their actual behaviour. It addresses the "why" behind their engagement or lack thereof, from a motivational and attitudinal standpoint20Having a physical health condition decreases the level of physical activity intervention adherenceSelf-Regulation for physical activityThis theme centers around an individual's capacity to manage their own behaviour related to physical activity. It includes skills like setting goals, monitoring progress, maintaining motivation, overcoming barriers, and adapting to challenges. This theme focuses on the processes and strategies people use to control and direct their physical activity behaviour. It addresses how well someone can put their intentions into action and stick with their physical activity routine, irrespective of their beliefs or circumstances14Being disciplined increases the level of physical activity intervention adherenceIndividual Characteristics and Experiences Affecting Physical ActivityThis theme focuses on the personal attributes, past experiences, and current circumstances that influence an individual's ability and likelihood to participate in physical activity. It includes physical factors (like age, health conditions, and physical limitations), cognitive factors (like knowledge and understanding of exercise), motivational factors (like intrinsic motivation and self-discipline), past experiences with physical activity, and practical/logistical considerations (like access to resources and time constraints). This theme emphasizes the tangible and practical aspects of physical activity adherence, focusing on what someone can do and what circumstances they face, rather than their attitudes or beliefs20When already active at the start of a physical activity intervention, older adults are less adherent to the physical activity programCategory 5: Context factors that relate to physical activity intervention adherencePerceived Benefits and Impact of the InterventionThis theme focuses on the positive outcomes and changes individuals experience as a result of participating in the intervention. It encompasses both physical and functional improvements, as well as the perceived impact on daily life and overall well-being. It addresses the tangible and noticeable effects of the intervention from the participant's perspective7Being able to generalize the physical activity intervention to daily life increases the level of physical activity intervention adherencePractical and Environmental ConsiderationsThis theme encompasses the external factors and circumstances that can affect an individual's ability to participate in the intervention. It includes logistical issues like access to technology, travel requirements, and scheduling conflicts, as well as environmental factors like weather conditions, space limitations, and the home environment. This theme highlights how real-world constraints and opportunities can influence participation14Good weather increases the physical activity intervention adherenceProgram Structure, Content, and DeliveryThis theme centers around the design and implementation of the intervention itself. It includes aspects like the clarity of instructions, the structure and organization of the program, the content of the exercises, the format of delivery (e.g., fixed schedules vs. flexibility), and any perceived issues with the program's content or design (e.g., repetitiveness, lack of challenge, age-inappropriateness). This theme focuses on the characteristics of the intervention itself and how they influence adherence26Having always the same exercises decreases the level of physical activity intervention adherenceSocial Influences and Group DynamicsThis theme focuses on the impact of social connections and interactions on participation in the intervention. It includes the influence of family, friends, other participants, and research staff. It also encompasses the dynamics of group exercise settings and the role of social support in motivation. This theme emphasizes how social context and relationships can affect adherence29Exercising together with others increases the level of physical activity intervention adherenceSupport, Guidance, and FeedbackThis theme emphasizes the role of assistance and encouragement provided to participants throughout the intervention. It includes the availability of technical support, guidance from trainers or healthcare professionals, personalized feedback on progress, and any perceived dependence on support. This theme highlights the importance of human interaction and personalized attention in facilitating adherence and success15Provision of personalized feedback increases the level of physical activity intervention adherence
Data extraction
Characteristics of the included studies and all data on factors that drive adherence to physical activity programs and adherence to with technology were extracted. A data extraction template was developed and pilot-tested on eight randomly selected studies, representing qualitative (n = 3), quantitative (n = 3), and mixed-methods (n = 2) designs. Following the pilot, the template was refined. A team of 9 reviewers (EP, JH, KF, MH, SA, SBS, SJGG, TK, YN) conducted the extraction. Regular meetings were held to discuss emerging issues, ensure consistency, and resolve discrepancies. Finally, three authors (MH, SJGG, DB) verified the accuracy of the extracted data.
A formal risk of bias assessment was not conducted, as the objective was to map the breadth of existing evidence rather than critically appraise study quality [28].
Data synthesis and analysis
Behaviour Change Techniques (BCTs) were coded according to the BCT Taxonomy (v1) [31], enabling a systematic analysis of intervention components specifically targeting physical activity adherence and technology adherence. Given the diverse delivery modes identified across studies, coding was intentionally separated into technology-assisted and human interaction-based categories to distinguish techniques delivered primarily through digital tools from those facilitated by direct or mediated human communication. This distinction helps clarify how different strategies leverage either technology or interpersonal dynamics to promote physical activity behaviour change among older adults. Human interaction-based delivery involves direct or mediated communication between older adults and individuals such as healthcare providers, trainers, peers, or coaches, who offer behaviour change techniques, tailored guidance, motivation, emotional support, or practical help. This support can be delivered through various channels, including face-to-face contact, phone calls, video chats, social media, emails, or home visits.
To account for differences in data types, qualitative and quantitative data on motivational and psychological factors were analysed separately.
For qualitative data, all results sections of the included studies were extracted and imported into separate Word files, which were subsequently uploaded to the qualitative data analysis software ATLAS.ti (Scientific Software Development GmbH, 2024). First, three reviewers (SJGG, DB, MH) inductively coded the papers. Second, SJGG performed a thorough double-check by reviewing all the codes and full-text papers. Third, discrepancies were resolved through discussion among the reviewers. Fourth, a Directed Content Analysis [32] approach was applied to categorize motivational and psychological factors using an adapted framework developed by Yang et al. (2022) [33] by incorporating the distinction between adherence to the technology and adherence to the physical activity component. Yang et al. (2022) propose a framework linking the user, technology, and contextual factors to adherence that together influence the effectiveness of technology-supported physical activity interventions [33]. Their framework provides a valuable structure for understanding what drives people to engage with such programs and supports the development of more consistent adherence measurement. It highlights how these three domains relate to different aspects of adherence. In our review, we build on this foundation by focusing specifically on psychological and motivational factors that underpin adherence. These factors are not mutually exclusive from Yang et al.'s categories; rather, they often manifest within and across user, technology, and context domains. However, Yang et al.'s model does not fully address the dual challenge older adults face—maintaining both adherence to the technology and adherence to the physical activity itself—nor does it account for technologies beyond mHealth, such as wearables and exergames, which are increasingly integrated into interventions for older populations.
The final framework (Fig. 1) consists of five categories: (1) user factors related to technology adherence, (2) technology-related factors associated with both technology adherence and physical activity adherence, (3) context factors related to technology adherence, (4) user factors related to physical activity adherence, and (5) context factors related to physical activity adherence. Fifth, we conducted an inductive thematic analysis to identify and develop themes within each category. This analysis was conducted by the same team of three reviewers (SJGG, DB, MH), with discrepancies resolved through team discussions and, when necessary, by consulting all authors.Fig. 1. This figure shows an adapted version of Yang et al.’s framework, highlighting how different user, technological, and contextual factors influence older adults’ adherence to technology-supported physical activity programs. It separates adherence into two parts: using the technology (B) and following the exercise recommendations (E). These two types of adherence are influenced by different factors (A1.1, A1.2, A1.3, D1.1, D1.2) and both contribute to being more physically active (F), which can lead to better health outcomes (G)
For quantitative studies, correlations and associations of motivational and psychological factors with adherence to the physical activity program and adherence to the technology as described by the included article, were presented.
Results
A total of 6819 studies were initially identified, with 1374 removed due to duplication. After screening 5445 studies based on titles and abstracts, 820 articles were selected for full-text evaluation. Of these, 53 studies were chosen for inclusion [34–86].
The PRISMA flowchart is presented in Fig. 2.Fig. 2PRISMA flowchart
Description of included studies
Appendix 3 provides an extensive overview of the included studies, including a description of the population, PA details, technology and BCTs used. Out of the 53 studies, 19 adopted a qualitative research approach [36, 41, 48, 51, 54–56, 59, 63, 65–67, 69, 73–76, 79, 82], 6 adopted a quantitative research approach [34, 39, 50, 57, 77, 78], and 28 adopted a mixed-methods research approach [35, 37, 38, 40, 42–47, 49, 52, 53, 58, 60–62, 64, 68, 70–72, 80, 81, 83–86]. A wide range of study designs was employed, reflecting the exploratory and developmental nature of the field. Randomized controlled trials (RCTs), including standard RCTs [37, 49, 70, 80], a pilot RCT [47], a cluster RCT [71], and a randomized crossover design [50], were used to assess intervention effects. Numerous feasibility studies [40, 43–45, 58, 60, 61, 65, 68, 72] evaluated the practicality and acceptability of technology-based programs. Mixed-methods approaches were commonly adopted, including explanatory sequential designs [38, 42, 51, 86], a convergent parallel design [84], convergent mixed-methods studies [41, 48, 62], and embedded mixed-methods evaluations [59, 85]. Several studies employed qualitative designs — including focus groups, interviews, and participatory methods — to explore participant experiences [36, 52, 53, 56, 63, 66, 67, 73–75], often as ancillary studies linked to larger RCTs [56, 67]. Secondary analyses of RCT data were also reported [57, 58]. Technology development was a central element across the majority of studies, emphasizing the adaptation and testing of digital or remotely delivered physical activity interventions for older populations.
Sample sizes ranged from two to 174 older adults. The overall mean number of participants per study was approximately 34. On average, each study included 23 female participants and 12 male participants, highlighting the predominance of female participants in the majority of the studies. The overall mean age across the studies is approximately 71.79 years, with an average standard deviation of 6.35 years. Four studies did not provide age mean/range [36, 45, 73, 82]. The included studies were published between 2010 and 2023.
Settings for the interventions were diverse, with 20 studies conducted in community-based settings [38, 39, 45, 51, 52, 56, 57, 61, 62, 65, 66, 68, 69, 71–74, 80, 84, 85], followed by 18 studies in home environments [36, 41, 43, 48, 50, 58–60, 63, 67, 70, 75–79, 81, 83, 86]. Additional settings included 2 studies in clinic environments [40, 47], 3 studies using online platforms [41, 42, 58], 3 studies in rehabilitation settings [54, 55, 67], and 2 studies in healthcare long-term care facilities [44, 46]. Other unique settings were represented by 1 study conducted via telehealth [45], 1 study in a web-based setting [49], and 1 study in a laboratory setting [64]. Five studies did not report clearly the setting [34, 35, 37, 53, 82].
Technologies used to support physical activity.
The included studies used either a single technology (N = 24) or a combination of multiple technologies (N = 29). Out of the 53 studies, 42 (≈ 79.2%) mentioned user centred-design, while 11 (≈ 20.8%) did not. However, most studies lacked information on the specific user-centred methodologies that were used. We classified the utilized intervention technologies into 11 distinct categories which were directly informed by the technologies that were reported in the included studies: Exergaming Platforms, Interactive Video Programs, Mobile Applications, Robotic Assistants, Sensor-Based Systems, Tablet Applications, Telehealth/Telemedicine Systems, Telephone-Based Interventions, Virtual Reality, Wearable Devices, Web-Based Platforms. The detailed definitions and descriptions of each category are provided in Appendix 4. Wearable devices were the most frequently used (N = 20) [34, 35, 38, 47, 58, 61, 62, 65, 66, 68, 69, 71, 73, 74, 77–79, 82–84]. These devices incorporate fitness trackers and smartwatches to monitor movement, track progress, and offer real-time feedback to users. Web-based platforms followed closely in usage (N = 19) [35, 38, 39, 41–43, 46, 49, 55, 59, 60, 62, 63, 65, 70, 75, 76, 79, 82]. These platforms deliver interventions via internet-accessible websites on various devices and provide structured programs, resources, and tracking features to support users' physical activity goals. Mobile applications (N = 10) [34, 36, 53–55, 68, 70, 72, 75, 78] were another prominent method, providing portability and accessibility for users to engage with programs on their smartphones. In addition, tablet applications (N = 7) [37, 38, 44, 47, 48, 58, 79] offered a similar function but with a larger interface, enhancing the user experience for certain populations. Meanwhile, interactive video programs (N = 13) [39, 44, 48, 51, 56, 58, 63, 65, 70, 79, 81, 83, 86] guided users through pre-recorded or live physical activity sessions, fostering engagement and adherence to exercise routines. Other technological modalities included sensor-based systems (N = 10) [50, 58, 63, 68, 69, 79, 80, 84–86], which utilized movement sensors to monitor physical activity and provide personalized feedback. Exergaming platforms (N = 6) [52, 64, 80, 81, 85, 86] integrated gaming elements with exercise, promoting activity in an engaging and interactive manner. Telehealth and telemedicine systems (N = 5) [39, 45, 50, 54, 56] enabled remote healthcare professionals to guide and monitor physical activity programs, offering real-time support and feedback. Less commonly used were telephone-based programs (N = 4) [43, 50, 57, 83], which relied on voice calls or SMS for content delivery and support. Virtual reality (VR) systems (N = 1) [40] created immersive environments to simulate real-world or imagined exercise scenarios, providing a unique and engaging experience. Additionally, a single study incorporated robotic assistants (N = 1) [67], utilizing robots for remote interaction, movement monitoring, or gamified exercise support.
FITT dimensions of the physical activity programs
The frequency of exercise interventions ranged from daily sessions to a minimum of once weekly, most commonly involving 2–3 sessions per week. Exercise intensity varied widely, including moderate, moderate-to-vigorous, and individually tailored or self-selected intensities, frequently at moderate levels. Sessions typically lasted between 20 and 60 min, though durations varied significantly by exercise type and individual goals. Exercise types primarily included aerobic activities (particularly walking), strength training, balance exercises, flexibility training, and occasionally recreational or virtual exercises (e.g., Wii sports). Many interventions combined multiple exercise types into comprehensive programs tailored to participants' needs and health status.
Behavioural Change Techniques used in the programs
Overall, interventions typically employed a combination of BCTs, aiming to promote physical activity behaviour change via technological delivery methods. The most commonly identified BCTs delivered through technology-assisted interventions included "self-monitoring of behaviour", "feedback on behaviour", "goal setting (behaviour)", "instruction on how to perform the behaviour", and "action planning". Additionally, techniques such as "social support (unspecified)", "prompts/cues", "behavioural practice/rehearsal", and "graded tasks" were frequently utilized. Notably, "adding objects to the environment" was also recurrently mentioned.
To provide more nuanced insight into how these techniques support adherence, we describe hereunder the BCTs separately according to their mode of delivery—whether conveyed via human interaction or integrated through technological tools.
BCTs delivered through human interactions commonly utilized techniques included "instruction on how to perform the behaviour", "social support (practical and emotional)", "demonstration of behaviour", "goal setting (behaviour)”, and "problem-solving". Interactions ranged across face-to-face sessions, virtual coaching, social media, emails, chats, and telephone/video conferencing. Less frequently delivered techniques were "information about health consequences, and "monitoring of emotional consequences". Overall, the most frequently mentioned interaction method is Face-to-Face, followed by Phone calls, Video conferencing, and Social media interactions. Several studies combine multiple methods to enhance the delivery of behaviour change techniques. The data indicates a diverse use of human-mediated methods to support behavioural interventions. The full list and definitions of human interaction methods used to deliver behaviour change techniques are provided in Appendix 5.
BCTs through technology primarily targeted self-regulation and instruction (e.g., goal setting, self-monitoring, feedback), while human-delivered BCTs focused on social and motivational support (e.g., social support, problem solving, verbal persuasion). This reflects the suitability of digital tools for structured guidance and the value of interpersonal contact for adaptive, context-sensitive support.
Qualitative research data
After coding and discussing, 417 psychological and motivational factors to older adults' adherence to technology-assisted physical activity programs that were reported using qualitative data. A comprehensive view of the thematic coding process including the results are shown in Supplementary Appendix 6 and summarized in Table 1.
The 417 psychological and motivational factors reported using qualitative data were assigned to all five groups of our framework (see Fig. 1). Psychological and motivational factors reported using qualitative data were most frequently assigned to the technology-related factors that relate to technology adherence (n = 227, 54%), context factors that relate to physical activity intervention adherence (n = 91, 22%), and user factors that relate to physical activity program adherence (n = 54, 13%). The remaining 45 factors were assigned to user factors that relate to technology adherence (n = 27, 7%) and context factors that relate to technology adherence (n = 18, 4%).
A total of 160 psychological and motivational factors were associated with a decrease in adherence to the physical activity or adherence to the technology. Conversely, 253 factors were linked to an increase in adherence, while 4 factors could be interpreted as either increasing or decreasing adherence.
Across all five categories, we identified 25 distinct themes. Technology-related factors that relate to technology adherence contained 10 themes, while context factors related to physical activity intervention adherence had 5 themes. Context factors that relate to technology adherence included 4 themes, and both user factors that relate to physical activity program adherence and user factors that relate to technology adherence each contained 3 themes. The number of codes within each theme ranged from 2 (i.e., Physical Limitations and Technology Use) to 57 (i.e., Feedback & Goal Setting).
Quantitative research data
In total, we identified nineteen distinct associations between factors and adherence. All tested associations are presented in Table 2. Of these, 12 were significantly associated, while 7 were found to be non-significant Table 2. Quantitative research data: associations between factors and adherenceN°Associations—standardized formulationStatements from study****Reference1Achieved previous week's step goal was significantly associated with the odds of weekly intervention adherenceOR = 3.1 95%CI [1.391; 6.899]“The odds of weekly intervention adherence for those who met the previous week’s step goal is 3.10 times higher than the odds for those who did not meet the previous week’s step goal.”[78]2Received virtual support was significantly associated with the odds of weekly intervention adherenceOR 1.01 95%CI [1.002; 1.020]“Regarding virtual support received, an increase in total comments received by one “like/comment” showed a one percent increase in the odds of weekly intervention adherence.”[78]3Anxiety was NOT significantly associated with *program usage (i.e., the number of completed program modules)*Users vs. non users4.7 (3) vs. 4.5 (2.9) (p =.62)[42]4Depression was NOT significantly associated with *program usage (i.e., the number of completed program modules)Users vs. non users3.8 (2.9) vs. 3.8 (3); p =.88[42]5Locus of control was NOT significantly associated with program usage (i.e., the number of completed program modules)*Users vs. non users23 (5.4) vs. 23.7 (4.3); p =.46[42]6Self-efficacy was NOT significantly associated with program usage (i.e., the number of completed program modules)Users vs. non usersSelf-efficacy pain: 3.4 (0.8) vs. 3.4 (0.9); p =.76Self-efficacy other symptoms: 3.5 (0.9) vs. 3.4 (0.9); p =.67[42]7Private self-consciousness was significantly associated with maintenance of physical activity“private selfconsciousness significantly moderated 18-month maintenance of physical activity (d = 0.34, β = 0.15, p = 0.04)”[57]8Baseline amotivation was significantly associated with maintenance of physical activity“Baseline amotivation moderated intervention effects (d = 0.55, β = 0.27, p = 0.006)”[57]9Family social support was NOT significantly associated with maintenance of physical activity“Baseline family social support moderating maintenance of physical activity at 18 months (d = 0.31, β = 0.13, p = 0.07)”[57]10Being a locomotor was significantly associated with being adherent to the physical activity intervention“…locomotion was associated with marginally higher adherence scores at week 3 (B = 149.04, t(16.00) = 1.64, p =.12), significantly higher scores at week 7 (B = 193.64, t(16.09) = 2.13, p <.05), and marginally higher scores at week 11 (B = 169.93, t(15.71) = 1.88, p =.08).3[47]11Believing no help is needed to get to the intervention location was significantly associated with exercise program adherenceOR = 10.88; 95%CI [6.27; 18.88][39]12The distance between home and the intervention location was significantly associated with exercise program adherenceOR =.85; 95%CI [.78;.91][39]13Level of satisfaction was significantly associated with exercise program adherence“There was a significant difference in overall patient satisfaction with each increment of adherence (P <.05, analysis of variance). Not surprisingly, highly adherent subjects rated the kiosk component of the training program more highly than other subjects.”[39]14Feeling more energetic than one’s usual level was significantly associated with a higher probability of engaging in some outdoor exercise following an EMA-survery (Ecological momentary assessment)“Feeling more energetic than one’s usual level (within-person effect) was associated with a higher probability of engaging in some outdoor exercise following an EMA survey (OR = 1.73, p =.021)”[70]15Perceived physical performance was significantly associated with walking program adherence“A significant correlation was present between the physical component of the 12-item Short Form Health Survey (PC-12) and walking program adherence (n = 8, r = 0.634, p = 0.049).”[34]16Perceived risk of over-activity was significantly associated with exercise program adherence“when exercise program adherence was set as the dependent variable, the perceived risk of over-activity score from the APQ and HRrest were found to be the most predictive variables”[34]17Reported motivation was NOT significantly associated with physical activity intensity adherence“no differences were found for the PA … intensity between people who reported increased motivation compared to those who did not report an increase in motivation in either group (p > 0.05)”[77]18Reported motivation was NOT significantly associated with physical activity quantity adherence“no differences were found for the PA quantity … between people who reported increased motivation compared to those who did not report an increase in motivation in either group (p > 0.05)”[77]19Motivational support phone calls was significantly associated with daily training time“Daily training time during the intervention phase with telephone support was significantly superior to daily training time during the control phase without telephone motivation (24.2 ± 9.4 versus 19.6 ± 10.3 min, P,0.001)”[50]Bolt text = independent factor; Italic = dependent factor^^association diminished over time
Discussion
The main purpose of this scoping review was to systematically search and explore key psychological and motivational factors that drive older people’s adherence to PA programs and adherence to technologies in technology-supported PA programs. We included 53 studies—primarily qualitative or mixed-method in design—and aimed to identify key factors that would facilitate adherence to technology, adherence to physical activity. A critical distinction—defined a priori—was made between adherence to the physical activity recommendations and adherence to the technology itself. While both are essential to the success of such interventions, they represent conceptually different behaviours. Adherence to physical activity refers to the degree to which users complete the prescribed activities, whereas adherence to technology captures the frequency and quality of interaction with the technological tool (e.g., app usage, wear time). Recognizing and measuring these forms of adherence separately is crucial to identify what drives sustained behaviour change.
From the included studies, we identified 25 thematic categories that captured both barriers and facilitators influencing these two types of adherence. These themes were distributed across five predefined categories of adherence-related factors: (1) user, (2) technology-related, and (3) context factors influencing adherence to technology, and (4) user and (5) context factors shaping adherence to physical activity. Together, these insights highlight a range of user and technological factors that may affect long-term participation.
Informing gerontechnology development
As digital tools are increasingly used to support physical activity among older adults, our findings offer practical guidance for gerontechnology researchers and developers. Technology-related factors—such as ease of use, clarity of feedback, and personalization—were most consistently reported. One of the most frequent technology-related factors that supported the adherence of older adults to technology, was found to be the need for a convenient interface. Older adults are more likely to adopt technologies that are intuitive, low in cognitive demand, and seamlessly integrated into daily life. These preferences align with findings from prior research on technology acceptance [87, 88]. Wearables were frequently used, possibly due to their user-friendliness and accessibility, yet their impact on long-term adherence remains uncertain [89]. Engaging in long-term physical activity, which may lead to changing behaviour patterns, depends highly on finding intrinsic motivation sources. Furthermore, the effectiveness of technology in sustaining physical activity for the long run is yet to be established [90]. Future work should therefore focus on longitudinal studies that assess how different technologies, particularly wearables, influence sustained physical activity over time, and explore how interventions can be designed to foster intrinsic motivation tailored to older adults’ individual needs and preferences. At the same time, our findings also point to determinants that operate across both domains of adherence. For instance, self-efficacy, motivation, social support, feedback, and personalization emerged as relevant to both consistent technology use and sustained participation in physical activity. Focusing on such cross-cutting determinants could increase intervention efficiency, as strategies targeting them may simultaneously strengthen engagement with technology and adherence to physical activity. Future developers may therefore consider balancing behaviour-specific strategies with approaches that leverage these overlapping determinants.
Our analysis shows that technologies can be both motivators and mediators. Some older adults find enjoyment in the technology itself, while others are motivated by the physical activity benefits [89, 91, 92]. Therefore, developers should consider dual pathways for adherence—those who rely on technology to initiate activity and those who need it to maintain routine. This line of thought raises an important question: should technology serve as a permanent tool for sustained physical activity or merely act as an intermediatory mechanism to foster intrinsic motivation and behavioural changes, ultimately empowering individuals to engage in physical activity without the mediation of technological devices? Addressing this question requires recognizing that older adults are not a homogeneous group in how they interact with technology or find motivation to stay active. There is thus a need to develop technologies targeting two different audiences among the older population. The first consists of people who need a technological intervention program to initiate and begin physical activity, and the second is those who need technology to consistently perform the activity over time. When looking into ways to improve long term adherence, it may be effective to implement technology-assisted programs which integrate technology into a wider concept, including psychological and social strategies. In addition, some older adults may show an addiction to technology such as smartphones [93]. While this smartphone-overuse is associated with decreased physical activity, it may be utilized by programmers to develop targeted exercise applications that may reverse this phenomenon. This population may be motivated by new features and applications on their smartphone rather than by the benefits of physical activities.
Key facilitators of adherence included motivation, enjoyment, feedback, and goal setting—elements that can be directly enhanced through thoughtful design guided by the overarching principle of personalization. Indeed, as motivation has a major role in initiating and maintaining physical activity habits [94], a personalized approach that addresses these various aspects holistically may lead to behaviour change and result in improved adherence. We conducted a BCT analysis to identify which techniques were embedded across interventions. This analysis revealed a variety of applied BCTs, yet few were explicitly tailored to the preferences or motivational profiles of older users. These findings underscore the importance of embedding BCTs such as self-monitoring, gamification, and motivational reminders. Personalization—based on user history, preferences, and capabilities—was also cited as a driver of sustained adherence. Hence, future research should investigate personalization strategies that adapt BCTs and technologies to older adults’ varying motivations, capabilities, and usage preferences.
Design strategies should also consider variability in social preferences. Social support—whether from peers, family, or through digital means—was one of the most frequently identified facilitators in our review. Nevertheless, digital interventions should balance social connectivity with privacy, as some users value technology as a means to foster interaction, while others may fear exposure or judgment—from peers or the technology itself [88, 92, 95]. Incorporating older adults’ lived experiences and supporting self-efficacy through tailored content is essential. This means enriching not only technological features but also the physical activity content itself to prevent boredom and disengagement. Supporting both intrinsic and extrinsic motivation is crucial to sustaining adherence over time.
Strengths and limitations
This scoping review has several strengths. It is one of the first reviews to comprehensively synthesise psychological and motivational factors influencing both adherence to physical activity and adherence to supporting technologies among older adults, using a structured qualitative research methodology to analyse and categorise data from diverse study designs. The dual focus—on both forms of adherence—and the structured categorization of factors provide valuable insights for developers and researchers alike. Additionally, the incorporation of a BCT analysis strengthens the practical relevance of our findings. However, certain limitations should be acknowledged. A limitation of this review is that, as with any evidence synthesis, the search reflects the state of knowledge up to a specific point in time. Given the rapid pace of innovation in digital health and physical activity technologies, some tools discussed may quickly become outdated. Nonetheless, the psychological and motivational principles identified in this review are likely to remain relevant and can guide the development and evaluation of future interventions. Looking ahead, emerging technologies such as adaptive AI may even strengthen adherence by providing more personalised feedback and dynamically addressing barriers such as low digital literacy, motivational decline, or repetitive content. However, given the extensive data processing and in-depth qualitative assessment undertaken, it is unlikely—though not impossible—that newly published studies would substantially alter the thematic findings of this review. Another limitation relates to the fact that the majority of included studies were qualitative, limiting the generalizability and strength of evidence. Additionally, we did not perform a formal risk of bias assessment or meta-analysis, as these are not typically required for scoping reviews, which aim to map the breadth of existing literature rather than assess intervention effectiveness [29]. Furthermore, a potential limitation of this scoping review is the search cut-off date of March 1, 2023. While some new studies may have emerged since then, we do not expect these additions to substantially alter the current, extensive overview of qualitative insights into psychological and motivational drivers of adherence.
Conclusions
In summary, this review highlights three key insights. First, adherence to physical activity and adherence to technology are conceptually distinct but interconnected targets, each requiring specific attention in intervention design and evaluation. Second, the synthesized evidence offers concrete guidance for gerontechnology developers and researchers, particularly regarding barriers and facilitators that matter to older adults. Third, future technologies should prioritize user-centred design, personalization, and the integration of behaviour change techniques to improve long-term adoption and effectiveness.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1NICE. Developing NICE guidelines: the manual. 2014; Available from: https://www.nice.org.uk/process/pmg 20.