Endogenous endophthalmitis complicating infective endocarditis: a multicentre case-matched control cohort
Iris Layani, Florent Arregle, Sebastian Santos Patarroyo, Aurore Aziz, Julien Mancini, Julien Ternacle, Peter Laursen Graversen, Emil Foesbol, Nuria Fernández-Hidalgo, Marco Tomasino, Antonia Sambola, Audrey Le Bot, Pierre Tattevin, Christophe Tribouilloy, Claire Lucas

TL;DR
Endogenous endophthalmitis is a rare but severe eye complication of infective endocarditis, requiring early detection to prevent vision loss.
Contribution
A multicenter study identifies clinical and microbiological differences in patients with IE-related endogenous endophthalmitis compared to controls.
Findings
EE patients had higher rates of diabetes, cirrhosis, glomerulonephritis, embolism, and Janeway lesions compared to controls.
Streptococcal infections were more common in EE patients, while Enterococcal infections were less common.
Most EE patients received intravitreal antibiotic injections, with partial visual improvement in 55% of cases.
Abstract
Endogenous endophthalmitis (EE) is a rarely reported complication of infective endocarditis (IE). In an international series, we sought to determine the clinical and microbiological profile, treatment, and outcome of patients presenting with IE-related EE. Cases recorded from 2014 to 2023 in nine centres in Europe and the United States were collected. Results were compared to a matched control group. Sixty-six patients with EE were reported, mean age of 65.2 ± 14.9 years, 71% (n = 47) male. Blood cultures were positive in 97% (64 cases) of patients, with a predominance of streptococci (46%, n = 30). As compared with the control group (n = 264), the EE group presented with more frequent diabetes (35% vs. 21%, P = 0.02), history of cirrhosis (9% vs. 3%, P = 0.04), glomerulonephritis (15% vs. 0.4%, P < 0.001), embolism before admission (92% vs. 55%, P < 0.001), and Janeway lesions (9%…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
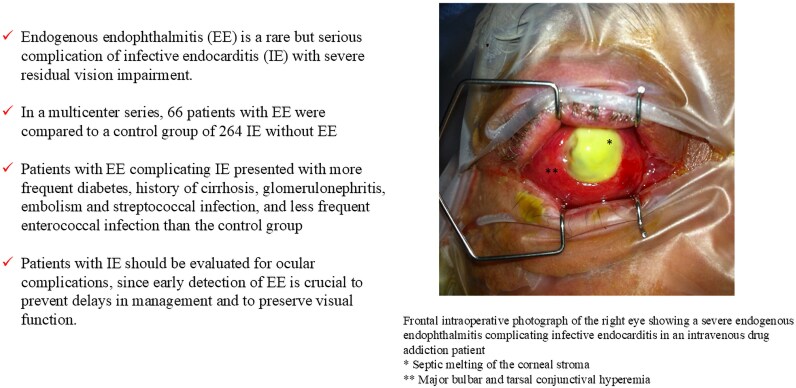 Figure 1
Figure 1 Figure 2
Figure 2| Endophthalmitis | Control |
| |
|---|---|---|---|
| Male | 47 (71) | 195 (74) | 0.6 |
| Age | 65.2± 14.9 | 66±14.6 | 0.8 |
| Medical history | |||
| Hypertension | 31 (47) | 115 (44) | 0.6 |
| Diabetes | 23 (35) | 55 (21) |
|
| Smoking | 18 (27) | 95 (36) | 0.16 |
| Atrial fibrillation | 12 (18) | 88 (33) |
|
| Chronic renal failure | 11 (17) | 26 (10) | 0.12 |
| Heart failure | 7 (11) | 49 (19) | 0.12 |
| Cirrhosis | 6 (9) | 8 (3) |
|
| Intravenous drug use | 4 (6) | 20 (8) | 0.8 |
| Clinical characteristics | |||
| Heart Failure | 14 (21) | 73 (28) | 0.29 |
| Septic shock | 12 (18) | 22 (8) |
|
| Osler’s node | 4 (6) | 5 (2) | 0.08 |
| Janeway lesion | 6 (9) | 3 (1) |
|
| Glomerulonephritis | 10 (15) | 1 (0.4) |
|
| Total embolism | 61 (92) | 144 (55) |
|
| Echocardiography | |||
| Left heart | 59 (89) | 223 (85) | 0.31 |
| Right heart | 5 (8) | 47 (18) |
|
| Prosthetic valve | 17 (26) | 94 (36) | 0.13 |
| Cardiac device-related infective endocarditis | 5 (8) | 31 (12) | 0.33 |
| Vegetation | 54 (82) | 201 (76) | 0.33 |
| Microbiology | |||
| Positive Blood culture | 64 (97) | 229 (87) |
|
| | 20 (30) | 67 (26) | 0.43 |
| Streptococci | 30 (46) | 68 (26) |
|
| Enterococci | 0 | 48 (18) |
|
| Gram negative bacilli | 3 (5) | 18 (7) | 0.78 |
| Fungi | 2 (3) | 2 (0.8) | 0.18 |
| Endophthalmitis | |
|---|---|
|
| |
| Ocular symptoms | |
| Left eye | 39 (59) |
| Right eye | 49 (74) |
| Bilateral | 22 (33) |
| Decreased visual acuity | 63 (96) |
| Ocular pain | 36 (55) |
| Red eye | 36 (55) |
| Conjunctivitis | 18 (27) |
| Hypopion | 20 (30) |
| Tyndall | 17 (26) |
| Hyalitis | 20 (30) |
| Intravitreal haemorrhage | 12 (18) |
| Roth’s spots | 16 (24) |
| Retinal detachment | 11 (17) |
| Visual acuity before treatment (logMAR) | 1.5 (0.2–>2.3) |
| Outcome | |
| Vision improvement | 36 (55) |
| Visual acuity after treatment (logMAR) | 0.7 (0–>2.3) |
| Severe vision impairment (worse than 0.4 logMar, ≈20/50) | 43 (65) |
| Blindness (worse than 1.0 logMar, ≈20/200) | 20 (30) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOcular Infections and Treatments · Ocular Diseases and Behçet’s Syndrome · Retinal and Optic Conditions
Endogenous endophthalmitis (EE) results from bacterial or fungal infection involving the vitreous and/or aqueous humours.^1^ Although a rare condition, it is frequently complicated by blindness and loss of the affected eye.^2^ Up to 15% of endophthalmitis cases are endogenous, due to haematogenous spread of organisms from extraocular sites, with infective endocarditis (IE) being the most common source.^1,3^ EE resulting from IE has been documented primarily in case reports.^4^ A recent retrospective study focused on predictive factors of EE complicating IE,^5^ but did not include data on microbiology or patient outcomes. In this international investigation, we aimed to determine the clinical features, treatment, and outcomes of patients presenting with EE complicating IE.
Materials and methods
Cases between 2014 and 2023 were included, and data were collected from the local IE registries of nine hospitals across Europe and the USA (see Supplementary material online, Table). Patients were included if they had definite IE according to the Duke^6^ or ESC criteria^7^ and presented with associated EE. Patients were compared to a 4:1 matched control group of IE patients without EE (matching on the nearest date of diagnosis from La Timone, Marseille, IE cohort).
The diagnosis of EE was based on a combination of clinical, microbiological (from blood cultures, intraocular samples from the anterior chamber or vitreous for Gram staining, culture (bacteria or fungi), and/or PCR), and imaging findings. Visual acuity was expressed in logarithms of the Minimum Angle of Resolution (logMAR) units, in accordance with international ophthalmology standards. On this scale, higher logMAR values indicate poorer visual acuity, while lower values (approaching zero or negative) indicate better vision. For reference, 0.0 logMAR corresponds to 20/20 Snellen equivalent, 0.4 logMAR to approximately 20/50, and 1.0 logMAR to approximately 20/200. Severe impairment was defined as visual acuity worse than 0.4 logMAR (≈20/50) in the affected eye. Patients were classified as legally blind when visual acuity was worse than 1.0 logMAR (≈20/200) at follow-up. The thresholds used in this study are consistent with the U.S. definition of legal blindness (best-corrected visual acuity of 20/200 or worse in the better-seeing eye, or visual field ≤ 20 degrees) as established by the Social Security Administration^8^ and are broadly aligned with the World Health Organization (WHO) classification of vision impairment.^9^ For patients with bilateral EE, visual acuity was assessed separately for each eye. For statistical analysis and classification of visual outcomes (e.g. severe impairment, legal blindness), the value from the eye with the worst visual acuity at follow-up was used. This approach was chosen to reflect the maximum degree of functional impairment experienced by the patient and to avoid underestimating vision loss in bilateral cases.
Data collected included demographic information, comorbidities, clinical signs and symptoms, echocardiographic findings, microbiological results, and follow-up information, including ophthalmic surgery and outcome of endophthalmitis (visual recovery, complications, and recurrences).
Categorical variables were expressed as percentages (counts) and compared using Χ² or Fisher’s exact tests. Continuous variables were expressed as mean ± standard deviation (SD) and compared using Student t-tests. The visual acuity (logMAR scale) was expressed as median [minimum–maximum]. Analyses were performed using IBM SPSS Statistics 20.0 (IBM Inc., New York, USA).
Ethical and regulatory aspects
Each centre complied with its national ethical and regulatory standards. All patients included gave consent for this protocol.
Results
Sixty-six patients with EE complicating IE were included (10 patients from the USA and 56 patients from Europe) and were compared to 264 control patients. Mean age was 65.2 years (± 15), with a male predominance of 71% (n = 47). Among comorbidities, EE patients had more diabetes mellitus (35% vs. 21%, P = 0.02) and cirrhosis (9% vs. 3%, P= 0.04) compared to the control group, but less atrial fibrillation (18% vs. 33%, P = 0.02) (Graphical Abstract).
Clinical symptoms of IE
In the EE group, 56 (85%) IE were community-acquired, and 4 patients had injection drug use. More patients in the EE group presented with septic shock (18% vs. 8%, P = 0.02). Janeway lesions (9% vs. 1%, P = 0.002), glomerulonephritis (15% vs. 0.4%, P < 0.001), and systemic embolism (92% vs. 55%, P < 0.001) were more frequent in the EE than in the control group (Table 1).
Echocardiography
Most patients (n = 59, 89%) had left-sided IE, while only 8% had right-sided IE, which was significantly lower than in the control group (18%, P = 0.04). There were no cases of bilateral IE. Most patients had native valve IE (68%). Vegetations were identified in 82% of patients, including aortic valve, mitral valve, and tricuspid valve vegetations in 39% (n = 22), 49% (n = 29), and 9% (n = 5), respectively. Annular complications occurred in 17% of patients.
Microbiology
Blood cultures were positive in 97% of patients in the EE group compared to 87% of patients without EE (P = 0.02) and showed a predominance of streptococci and Staphylococcus aureus. When compared to the control group, EE patients had significantly more streptococci infection (46% vs. 26%, P = 0.001) and less enterococci infection (0% vs. 18%, P < 0.001).
Ocular symptoms, treatment and outcome
EE affected the right eye more frequently (74%, n = 49) than the left eye (59%, n = 39) and 33% (n = 22) of patients had bilateral involvement. EE diagnosis was suspected in the presence of symptoms including vision loss in 96% (n = 63) of patients, pain (55%, n = 36), and red eye (55%, n = 36) (Table 2 and Graphical Abstract).
Intravitreal antibiotic injections were performed in 83% (n = 55) of patients. Vancomycin was the most frequently used (71%, n = 47) antimicrobial, followed by ceftazidime (49%, n = 32), and amphotericin B in 6% (n = 4) of patients. Vitrectomy was performed in 26% (n = 17) of patients.
Vision improvement was observed in 55% (n = 36) of patients (74%, n = 14 in the S. aureus group and 52%, n = 15 in the streptococci group). Retinal detachment was present in 11 patients, accounting for 17% of the total cohort. The percentage of patients maintaining a satisfactory level of visual acuity was 30% (n = 20). Conversely, 65% (n = 43) of patients experienced severe impairment. Among them, 30% (n = 20) were classified as legally blind. In-hospital and one-year mortality rates were 16% (n = 11) and 27% (n = 16), respectively. The IE recurrence rate was 4% (n = 2).
Discussion
This international study provides an analysis of the clinical, microbiological, and outcome characteristics of patients affected by EE in IE. Although this complication is rare, it often leads to significant functional impairment.
General characteristics of patients in our cohort, such as age and sex, were consistent with those of a recent cohort of IE patients.^10^ Comorbidities associated with EE were diabetes mellitus and cirrhosis, as recently reported.^5^
Interestingly, streptococci were the most common pathogens in our cohort, followed by S. aureus. No cases of EE complicating E. faecalis IE were detected, however. This is an intriguing observation, as most series of IE cases report that enterococci are among the top three IE pathogens.^10^ Enterococci were not only not identified in our current series of EE cases, but were not seen among pathogens in an earlier series of EE cases, where IE was the most common source^3^ or listed as pathogens in a recently published State-of-the-Art review on ocular infections.^11^ Thus, it is tempting to speculate that certain virulence determinants in EE causation may not be present in IE cases due to enterococci and deserve further study.
Unfortunately, at one-year follow-up, about two-thirds of patients had experienced severe residual visual acuity impairment. This highlights the poor functional prognosis of this complication that has been characteristic in other investigations^12^ and warrants evaluation with a thorough history and physical examination in every patient with IE, despite the limited yield in prevalence.^5^
Limitations
This is a retrospective observational study with inherent limitations, and the small number of patients impairs the robustness of the results. No multivariate analysis was performed due to the small sample size. Moreover, the control group was obtained from a single centre, which could not be representative of epidemiological data from the other centres.
Conclusion
EE is a rare but serious complication of IE that commonly results in vision loss. Our investigation highlights a high burden of comorbidities such as diabetes mellitus and cirrhosis, and the prevalence of streptococci in this population. Although infrequent, EE should be evaluated in each IE patient with specific evaluation as part of both the history and physical examination, since early detection of EE is crucial to prevent delays in management and to preserve visual function.
Lead author biography
Gilbert HABIB
Present Position and Address
Chair of the Cardiology Department (heart failure, valvular heart disease) La Timone Marseille France.Director of the echocardiographic laboratory la Timone Marseille.
European Society of Cardiology Activities
President of the European Association of Cardiovascular Imaging 2014–2016Chairman of the ESC guidelines on infective endocarditis 2009 and 2015Chairman of the EACVI guidelines for the use of echocardiography in infective endocarditis 2010Chairman of the EORP/ESC EUROENDO registry 2017–2019
Major Publications
More than 300 publications in international peer-reviewed journals.
Supplementary Material
oeaf136_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Durand ML, Barshak MB, Sobrin L. Eye infections. N Engl J Med 2023;389:2363–2375.38118024 10.1056/NEJ Mra 2216081 · doi ↗ · pubmed ↗
- 2Schiedler V, Scott IU, Flynn HW Jr, Davis JL, Benz MS, Miller D. Culture-proven endogenous endophthalmitis: clinical features and visual acuity outcomes. Am J Ophthalmol 2004;137:725–731.15059712 10.1016/j.ajo.2003.11.013 · doi ↗ · pubmed ↗
- 3Okada AA, Johnson RP, Liles WC, D’Amico DJ, Baker AS. Endogenous bacterial endophthalmitis. Report of a ten-year retrospective study. Ophthalmology 1994;101:832–838.8190467 · pubmed ↗
- 4Chen KJ, Sun MH, Chen YP, Wang NK, Wu WC, Lai CC. Endogenous endophthalmitis caused by infective endocarditis in east Asia. Ophthalmol Retina 2019;3:382–384.31014693 10.1016/j.oret.2019.01.007 · doi ↗ · pubmed ↗
- 5Shah MK, Zhu A, Uppuluri A, Henry RK, Zarbin MA, Bhagat N. Risk factors for endogenous endophthalmitis in infectious endocarditis patients. Eye (Lond) 2024;39:125–132.39402169 10.1038/s 41433-024-03390-w PMC 11733160 · doi ↗ · pubmed ↗
- 6Li JS, Sexton DJ, Mick N, Nettles R, Fowler VG Jr, Ryan T, Bashore T, Corey GR. Proposed modifications to the Duke criteria for the diagnosis of infective endocarditis. Clin Infect Dis 2000;30:633–638.10770721 10.1086/313753 · doi ↗ · pubmed ↗
- 7Habib G, Lancellotti P, Antunes MJ, Bongiorni MG, Casalta JP, Del Zotti F, Dulgheru R, El Khoury G, Erba PA, Iung B, Miro JM, Mulder BJ, Plonska-Gosciniak E, Price S, Roos-Hesselink J, Snygg-Martin U, Thuny F, Tornos Mas P, Vilacosta I, Zamorano JL. 2015 ESC guidelines for the management of infective endocarditis: the task force for the management of infective endocarditis of the European Society of Cardiology (ESC). endorsed by: European association for cardio-thoracic surge · doi ↗ · pubmed ↗
- 8Social Security Administration . Disability Evaluation Under Social Security (Blue Book), Section 2.02 Loss of Central Visual Acuity. SSA, 2023. Available at: https://www.ssa.gov/disability/professionals/bluebook/2.00-Special Sensesand Speech-Adult.htm