An Unusual Initial Presentation of Gout at the Wrist: Extensor Tenosynovitis With Dual-Energy CT and MRI Correlation
Kwan Kit Chan, Wai Hoi Chan

TL;DR
A 34-year-old man with wrist pain had gout diagnosed using advanced imaging techniques like dual-energy CT and MRI.
Contribution
This case highlights the rare initial presentation of gout at the wrist and the diagnostic utility of multimodal imaging.
Findings
Dual-energy CT identified monosodium urate crystal deposits in extensor tendons.
MRI showed tenosynovitis and tophus infiltration, aiding surgical planning.
Postoperative recovery resolved symptoms, confirming the diagnosis.
Abstract
Gout involving the wrist as an initial presentation is uncommon, especially when manifesting as extensor tenosynovitis with tophaceous deposits. We present the case of a 34-year-old male with chronic wrist pain and a dorsal wrist mass whose diagnosis was established through multimodal imaging, including dual-energy CT (DECT) and MRI. DECT effectively identified monosodium urate (MSU) crystal deposits in the extensor tendons, while MRI demonstrated tenosynovitis and tophus infiltration, guiding surgical synovectomy. Postoperative recovery was favourable with the resolution of symptoms. This report highlights the diagnostic challenges of wrist gout and underscores the value of advanced imaging techniques in early detection and operative planning.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
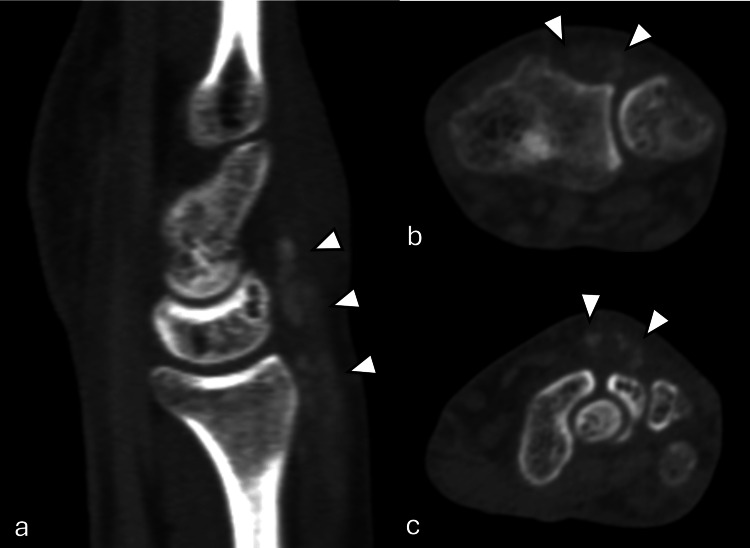 Figure 1
Figure 1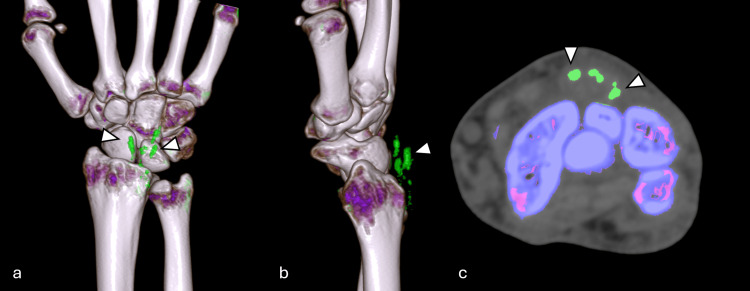 Figure 2
Figure 2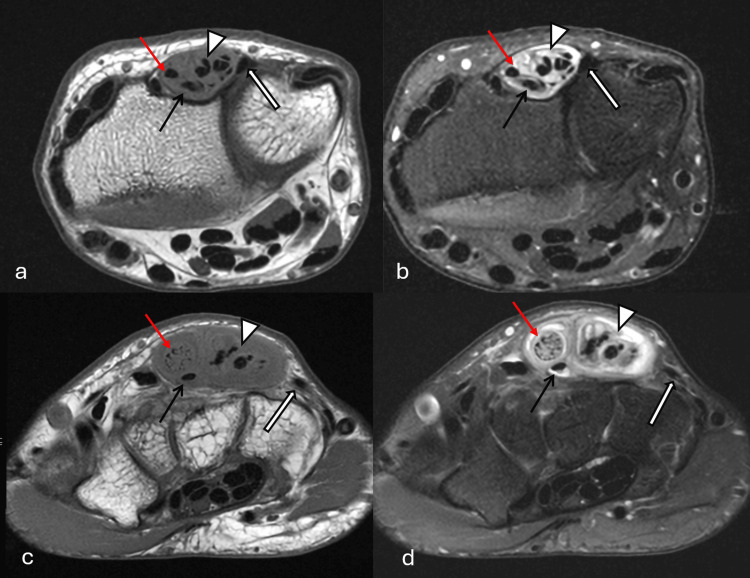 Figure 3
Figure 3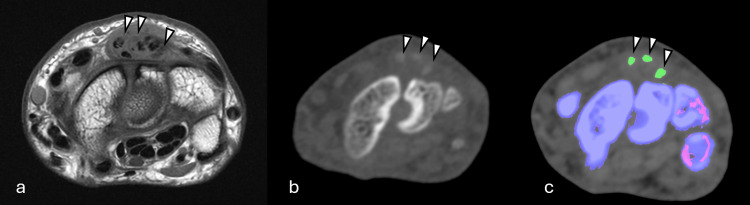 Figure 4
Figure 4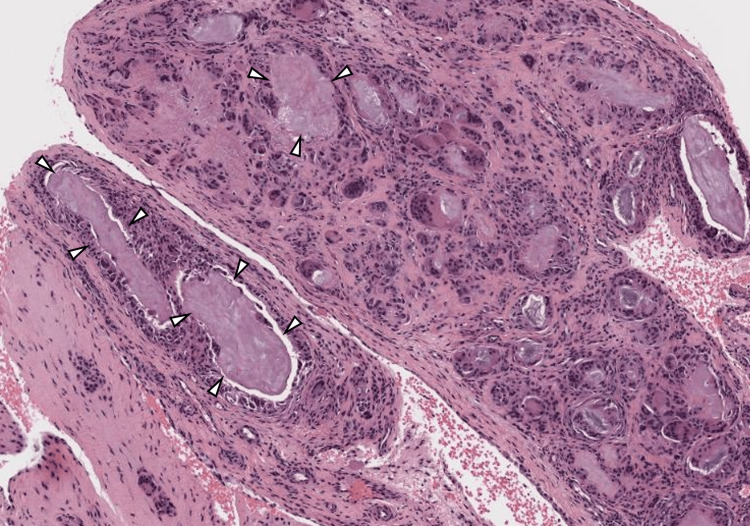 Figure 5
Figure 5| Blood test | Result | Normal range |
| Uric acid | 0.72 mmol/L | 0.25-0.52 mmol/L |
| White blood cell count | 7.4 x109/L | 4.0-9.7 x109/L |
| C-reactive protein | 3.1 mg/L | <5.0 mg/L |
| Creatinine | 116 umol/L | 64-104 umol/L |
| Rheumatoid factor | <15.9 IU/mL | <15.9 IU/mL |
| Cyclic citrullinated peptide antibodies | <1 RU/mL | <5 RU/mL |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGout, Hyperuricemia, Uric Acid · Musculoskeletal synovial abnormalities and treatments · Shoulder Injury and Treatment
Introduction
Gout is a common inflammatory arthropathy affecting approximately 3.9% of adults, characterized by the deposition of monosodium urate (MSU) crystals in joints and soft tissues [1]. In the upper extremity, tophi are most often found in the subcutaneous tissues, particularly around the elbow and the proximal interphalangeal joints [2]. Wrist gout as an initial presentation is relatively uncommon and accounts for only about 0.8-2% of all gout cases [3].
Wrist gout as an initial presentation is diagnostically challenging due to its rarity, atypical presentation, and overlap with other joint diseases and arthritis that can cause wrist pain. Traditional imaging modalities may not adequately demonstrate MSU crystal deposits, making dual-energy CT (DECT) an invaluable diagnostic tool [4]. MRI is also helpful in the diagnosis of gout at uncommon sites or early in the disease, before bone damage appears [5]. We present a case of chronic extensor tenosynovitis secondary to tophaceous gout in a young adult male, emphasizing the diagnostic value of multimodal imaging, including DECT and MRI, in establishing the diagnosis and guiding surgical management.
Case presentation
A 34-year-old right-handed male patient presented with a four-year history of chronic right wrist pain and a two-year history of palpable mass on the dorsal aspect of his right wrist. He was a smoker and an occasional alcohol consumer. The pain was episodic in nature with functional limitations characterized by restricted wrist extension when fingers were extended, though he could extend his wrist normally when fingers were flexed. No other joint pain or mass at joints was reported by the patient. His father had gout and hyperuricemia.
Physical examination revealed a mobile mass on the dorsal wrist that moved distally with finger flexion and proximally to the level of the distal margin of the extensor retinaculum with finger extension. There was no focal tenderness or signs of acute inflammation. Finger extension was full without finger drop. Laboratory investigations showed elevated serum uric acid at 0.72 mmol/L (normal range: 0.25-0.52 mmol/L). C-reactive protein, white blood cell count, rheumatoid factor, and cyclic citrullinated peptide antibodies were normal. Creatinine was mildly elevated at 116 umol/L (normal range: 64-104 umol/L) (Table 1).
DECT examination (uric acid/calcium pair; Hounsfield unit (HU) threshold: 150; iodine ratio: 1.36) revealed soft tissue swelling with high-density foci over the dorsal aspect of the right wrist, involving the extensor tendons (Figure 1). Color-coded dual-energy analysis demonstrated the presence of uric acid deposits consistent with gouty tophi (Figure 2). No similar findings were identified in the carpal tunnel or the rest of the wrist joint.
CT right wrist in bone windowCT right wrist in bone window with sagittal (a) and axial (b, c) planes. Soft tissue swelling with high-density foci (arrowheads) over the dorsal aspect of the wrist, involving the extensor tendons, corresponds to intratendinous gouty tophiCT: computed tomography
Dual-energy CT of the right wristDual-energy CT of the right wrist with 3D reconstruction (a, b) and at the axial plane (c). Dual-energy CT with color coding demonstrated the presence of uric acid deposits at the fourth extensor compartment of the wrist, consistent with gouty tophi (arrowheads)CT: computed tomography
MRI of the right wrist demonstrated grossly thickened extensor digitorum tendons with moderate-volume sheath fluid and sheath thickening. Heterogeneous para-tendinous and intratendinous signal changes were observed, compatible with tenosynovitis and gouty tophus infiltration (Figure 3), corroborating the DECT findings (Figure 4).
T1W and T2W fat-suppressed images of MRI wristT1-weighted (T1W) axial images (a, c) and T2-weighted (T2W) fat-suppressed images (b, d) of the MRI right wrist of the patient. They demonstrated grossly thickened extensor digitorum tendons with moderate-volume sheath fluid and sheath thickening. Heterogeneous para- and intratendinous signal changes were observed, compatible with tenosynovitis and gouty tophus infiltration. Note the significant tendon thickening at the extensor digitorum communis tendons to the second digit (red arrows), thickened extensor digitorum communis tendons to the third, fourth, and fifth digits with suspect longitudinal tears (arrowheads). Preserved extensor indicis tendon (black arrows) and extensor digiti minimi tendon (block arrows). MRI provided a detailed visualization of the anatomy. The MRI results were consistent with the intraoperative findingsMRI: magnetic resonance imaging
MRI, CT and Dual-energy CT images at the same level of the wristGouty tophi (arrowheads) appeared as low to intermediate signal in T1-weighted (T1W) MRI (a) and as mildly hyperdense foci in CT (b). They were easily picked up in dual-energy CT (c)MRI: magnetic resonance imaging; CT: computed tomography
Based on the clinical presentation, elevated uric acid, family history, together with the DECT and MRI findings, tophaceous gout affecting the wrist extensor tendons was suspected. Allopurinol was started, and a low-purine diet was recommended. Despite medical management with allopurinol, which successfully reduced uric acid levels to 0.57 mmol/L, the patient continued to experience a similar frequency of joint pain attacks and persistent limitation in wrist extension. Consequently, surgery was offered.
Intraoperative exploration revealed copious synovitis predominantly involving the fourth extensor compartment with visible gouty tophaceous material. The extensor digitorum communis tendons to the second, third, fourth, and fifth digits (EDC2, EDC3, EDC4, EDC5) showed approximately 30% partial tears with unhealthy-appearing tendons that were grossly thickened and irregular in appearance, particularly in the area just distal to the extensor retinaculum. The extensor indicis (El) and extensor digiti minimi (EDM) are intact. No signs of infection were present. Debridement of the gouty tophaceous materials with surgical synovectomy of the affected synovium was performed.
Histopathological examination of the resected synovial tissue revealed deposits of acellular pale-staining fibrillary material admixed with multinucleated giant cells with overall features compatible with gout (Figure 5).
Histopathological examination of the resected synovial tissueHistopathological examination (H&E staining) of the resected synovial tissue revealed deposits of acellular pale-staining fibrillary material (arrowheads), admixed with multinucleated giant cells, compatible with gout
Following rehabilitation, the patient regained a full range of motion in the affected wrist. Postoperative follow-up demonstrated resolution of the mechanical symptoms and improved functional capacity.
Discussion
Gout affecting the wrist is uncommon, with wrist tendon urate deposition found in 5.4% of gouty patients in a study involving 148 patients [6]. The fourth and fifth extensor compartments are among the more commonly affected sites in the hand/wrist, with reported involvement rates of 55.1% and 53.8% respectively, of non-acute hand/wrist gout patients [7]. Traditional radiographic imaging has limited utility in early gout diagnosis, typically only revealing changes such as bone erosions, joint destruction, and tophi after 7-10 years of disease progression [6]. Recent advanced imaging modalities, including DECT and MRI, have enhanced both early detection capabilities and diagnostic problem-solving in gout evaluation.
DECT proved invaluable in this case by definitively identifying MSU crystal deposits within the wrist extensor tendons. This advanced imaging technique utilizes the material-specific attenuation differences of urate crystals at different energy levels (usually at 80 kV and 140 kV), allowing accurate detection and color-coding of MSU deposits [7]. DECT is a highly sensitive and specific non-invasive method for detecting MSU crystals, with reported sensitivity of 88% and specificity of 90% for gout diagnosis [8]. The high sensitivity and specificity of DECT make it particularly useful in cases where joint aspiration is not feasible for definitive diagnosis or when crystal deposition occurs in extra-articular locations such as tendons and ligaments [9].
On MRI, tophi usually appear as low signal on T1-weighted images and variable intermediate to high signal on T2-weighted images, reflecting cellular tissue around the crystals. The vascularity of this tissue affects the extent of contrast enhancement, while calcifications within the tophus cause low T2 signal areas [5]. MRI also provided detailed visualization of the associated soft tissue changes, including tendon thickening, synovial proliferation, and the extent of tenosynovitis [10]. This multimodal imaging approach enabled comprehensive preoperative planning and informed the surgical decision-making process. In this case, the surgical findings correlated well with the imaging studies, demonstrating the efficacy of DECT and MRI in assisting preoperative planning.
Surgical indications for gout in the hand and wrist include severe tenosynovitis, tendon infiltration by tophi, and significant loss of joint or tendon function, as observed in our patient. Surgery involves the excision of inflamed synovium and removal of tophaceous deposits to restore function and reduce symptoms, particularly helpful when medical management fails [11]. Nonsteroidal anti-inflammatory drugs (NSAIDs), colchicine, and corticosteroids (oral or injected) are the primary treatments to reduce pain and swelling during acute gout attacks. For long-term management of chronic gout, urate-lowering drugs like allopurinol or uricosurics reduce tophi and prevent flare-ups [12]. In severe or resistant cases, biologics and targeting agents such as anti-interleukin-1 may be used [13].
Conclusions
Wrist involvement as the initial presentation of gout poses a diagnostic challenge due to its rarity and nonspecific clinical signs. Traditional imaging is often inadequate in early disease stages. DECT combined with MRI offers complementary advantages in detecting urate crystals and associated soft tissue changes. Awareness of this uncommon presentation and the role of advanced imaging can aid in the timely diagnosis and improved patient outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Prevalence of gout and hyperuricemia in the US general population: the National Health and Nutrition Examination Survey 2007-2008 Arthritis Rheum Zhu Y Pandya BJ Choi HK 313631416320112180028310.1002/art.30520 · doi ↗ · pubmed ↗
- 2A rare manifestation of gout at the wrist--a case report Acta Orthop Scand Schuind FA Van Geertruyden J Stallenberg B Remmelink M Pasteels JL 5945967320021244050710.1080/000164702321022910 · doi ↗ · pubmed ↗
- 3An unusual case of gout in the wrist: the importance of monitoring medication dosage and interaction. A case report Chiropr Osteopat Jacobs CL Stern PJ 161520071792292110.1186/1746-1340-15-16PMC 2174925 · doi ↗ · pubmed ↗
- 4Dual-energy CT as a potential new diagnostic tool in the management of gout in the acute setting AJR Am J Roentgenol Nicolaou S Yong-Hing CJ Galea-Soler S Hou DJ Louis L Munk P 1072107819420102030851310.2214/AJR.09.2428 · doi ↗ · pubmed ↗
- 5Imaging in gout--what can we learn from MRI, CT, DECT and US?Arthritis Res Ther Mc Queen FM Doyle A Dalbeth N 2461320112208568410.1186/ar 3489 PMC 3334625 · doi ↗ · pubmed ↗
- 6The distribution of urate deposition within the extremities in gout: a review of 148 dual-energy CT cases Skeletal Radiol Mallinson PI Reagan AC Coupal T Munk PL Ouellette H Nicolaou S 2772814320142433741410.1007/s 00256-013-1771-8 · doi ↗ · pubmed ↗
- 7Distribution of urate crystal deposition in the hands and wrists of patients with chronic gout Hong Kong J Radiol Leng Y Chow DL Chui SK Ip NSK Chan SWC Choi KY Li AOC 8791242021
- 8Diagnostic accuracy of dual-energy CT in gout: a systematic review and meta-analysis Skeletal Radiol Yu Z Mao T Xu Y Li T Wang Y Gao F Sun W 158715934720182972571210.1007/s 00256-018-2948-y · doi ↗ · pubmed ↗