Primary Ewing sarcoma of the kidney mimicking hydatid cyst: A case report with literature review
Rebaz M. Ali, Shakhawan Hama Amin Said, Shano M. Ali, Mzhda Sahib Jaafar, Rawa Bapir, Rawa M. Ali, Hadeel Adnan Yasseen, Rezheen J. Rashid, Hiwa O. Abdullah, Sasan M. Ahmed, Fahmi H. Kakamad

TL;DR
A rare case of kidney Ewing sarcoma was mistaken for a hydatid cyst, highlighting the difficulty in diagnosing this aggressive tumor.
Contribution
This case report adds to the limited literature on primary renal Ewing sarcoma and its diagnostic challenges.
Findings
Primary renal Ewing sarcoma can mimic a hydatid cyst on imaging.
The disease is rare, comprising only 1% of renal tumors.
Diagnostic challenges arise due to nonspecific imaging features.
Abstract
Primary renal Ewing sarcoma (EWS) is a rare and aggressive disease with a poor prognosis. Due to its nonspecific presentation and radiological findings, it can be misdiagnosed. This study reports a case of primary renal EWS mimicking a hydatid cyst. The case (31-year-old female) presented with right loin pain for a one-month duration. Abdominal magnetic resonance imaging demonstrated a well-defined, thick-walled cystic lesion occupying the upper and middle poles of the kidney, compressing the adjacent calyces and renal vessels, and showing thin peripheral septa. The features were suggestive of a hydatid cyst. The latex agglutination test for hydatid disease was negative. An excisional biopsy followed by a partial nephrectomy was performed, and histopathology confirmed the cyst as primary renal EWS. Extraosseous cases are rare, accounting for approximately 6% of all EWS cases. Primary…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
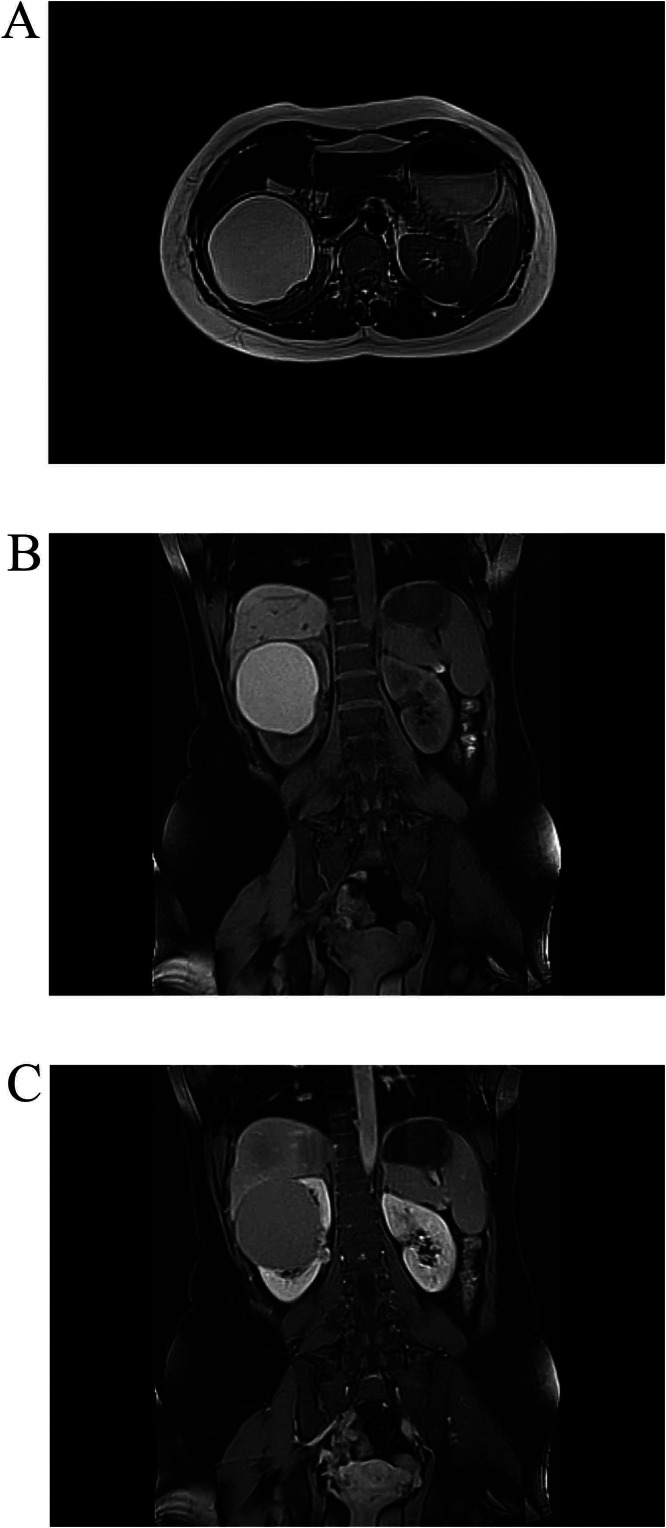 Figure 1
Figure 1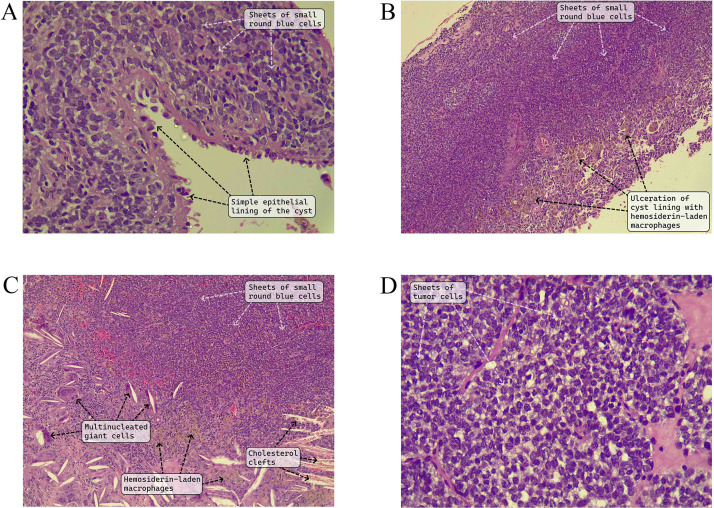 Figure 2
Figure 2 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSarcoma Diagnosis and Treatment · Cardiac tumors and thrombi · Renal cell carcinoma treatment
Background
Ewing sarcoma (EWS), also known as peripheral neuroectodermal tumor, is a malignant bone tumor that mainly affects children and young adults, peaking in the second decade of life. Extraosseous cases are rare, accounting for approximately 6% of the cases. The most common sites include the head and neck regions, trunk, extremities, and retroperitoneum [1,2]. Primary renal EWS is a sporadic and aggressive condition that comprises only 1% of renal tumors [3,4]. Due to its aggressive nature, this tumor highly metastasizes, commonly to the lungs, followed by the regional lymph nodes and the liver [3]. The disease has a poor prognosis, typically with survival of less than one year. This is due to factors including delayed diagnosis, large tumor size, aggressive behavior, and high likelihood of metastasis [4,5]. Due to the nonspecific clinical presentation and radiological imaging findings of the tumor, it can be misdiagnosed provisionally [6,7]. This study aims to report a case of primary renal EWS in an adult female. The report has been written based on the CaReL guidelines [8].
Case presentation
Patient information
A 31-year-old female presented with right loin pain for one month without any other symptoms. Her past medical and surgical histories were negative.
Clinical findings
Apart from right loin tenderness, no other significant abnormality was noticed during the physical examination.
Diagnostic assessment
Blood investigations, including complete blood count and liver and renal function tests, were normal. An abdominal and pelvic CT scan showed a large (9×9×9 cm), thick-walled, cystic lesion occupying most of the anterior aspect of the upper pole and midportion of the right kidney. It exerted pressure on the pelvicalyceal system and renal vein, resulting in the formation of renal collaterals. The cyst showed internal thin, enhancing septation with no mural nodules or calcification (image not available). Abdominal magnetic resonance imaging (MRI) revealed a well-defined, thick-walled cystic lesion in the upper and middle poles of the kidney (9.5×9 cm), compressing the adjacent calyces and renal vessels, and exhibiting thin peripheral septa with hyperintense signals on T1 and T2 images. The cyst showed no signs of restricted diffusion, enhancing septa, or solid components (Fig. 1). The features were suggestive of a hydatid cyst. However, the cyst lacked daughter cysts, floating membranes, or peripheral calcification of the cyst wall. The latex agglutination test for hydatid disease was negative.Fig. 1. The right renal cystic lesion appeared hyperintense on axial T1WI. A) hyperintense signal on axial T2 WI. B) No signal loss on precontrast coronal fat suppression T1WI, and no restriction on DWI (not shown). C) No obvious enhancement in postcontrast coronal fat suppression T1WI.Fig 1
Therapeutic interventions
An excisional biopsy followed by a partial nephrectomy without lymph node dissection was performed. Histopathologic examination showed a cyst lined by a simple cuboidal epithelium with bland, round nuclei. The wall of the cyst contained sheets of monomorphic, small cells with indistinct cytoplasmic membranes, scant clear or lightly eosinophilic cytoplasm, and round nuclei with stippled chromatin, nuclear membrane irregularity, and occasional grooves. Mitotic activity was low (4 to 5/ per 10 high-power fields), and there was no coagulative tumor necrosis. The cyst lining was ulcerated in areas with sheets of hemosiderin-laden macrophages and cholesterol clefts engulfed by multinucleated giant cells. The resection margin was free from tumor (Fig. 2). Immunohistochemistry (IHC) showed positivity of the tumor cells for CD99 (cytoplasmic staining of moderate intensity in >50% of the tumor cells) and FLI-1 (nuclear staining of moderate intensity in >50% of the tumor cells). AE1/AE3 highlighted the epithelial lining of the cyst, but was negative in the tumor cells. INI-1 was retained in the tumor cells, and WT1, desmin, myogenin, BCOR, TLE-1, CD45CLA, and synaptophysin were all negative (not shown). The combined histologic and immunohistochemical findings were consistent with a primary EWS of the kidney. The patient received 12 cycles of adjuvant chemotherapy (vincristine, actinomycin D, cyclophosphamide/ ifosfamide, and etoposide {VAC/IE}) every 21 days; each cycle was received over five days.Fig. 2A) The renal cyst has a simple epithelial lining of cuboidal and low columnar cells with underlying solid nodules composed of sheets of small, round, blue cells. B) The cyst lining shows extensive ulceration with replacement by sheets of hemosiderin-laden macrophages. C) There are cholesterol clefts engulfed by multinucleated giant cells. D) The tumor cells are small to medium-sized and have scant, lightly eosinophilic to clear cytoplasm with round to oval, hyperchromatic nuclei that have irregular nuclear outlines and occasional grooves. (Hematoxylin and eosin [A-D]; original magnification x 400 [A and D], x 100 [B and C]).Fig 2
Follow-up and outcome
Follow-up included abdominal and pelvic CT scans (Fig. 3) every three months and two positron emission tomography (PET) scans, all of which were normal. However, the third PET scan, taken approximately one year postoperation, revealed an FDG-avid right paracolic peritoneal nodule (1.3×0.9 cm, SUV max 7.1), suspicious for metastasis (not shown). Excision of the peritoneal surface nodule in the paracolic gutter was performed along with an omental biopsy and a peritoneal wash aspirate of the right paracolic gutter. The peritoneal surface nodule exhibited chronic inflammation with foreign body-type granulomas, indicating no malignancy. The omental biopsy and peritoneal wash aspirate also revealed no significant pathology and were negative for malignancy. After one year of follow-up, the patient remains disease-free.Fig. 3. Coronal reformatted contrast-enhanced abdominal CT shows signs of operation at the mid portion in the form of renal cortical discontinuity (arrow).Fig 3
Discussion
EWS was first identified in 1918 and is classified within the family of small round-cell tumors [2]. However, the first case of renal EWS was reported in 1975, and since then, fewer than 150 cases have been reported in the literature [3,7]. The tumor arises from neural crest cells or mesenchymal stem cells. It is characterized by the t(11;22)(q24;q12) translocation, present in 85% to 95% of the cases, which translocates the EWSR1 gene on chromosome 22 to the FLI-1 gene on chromosome 11 [3,9].
The mean age at diagnosis has been reported to be 24.9 years, with a male predominance. Patients commonly present with flank pain, hematuria, and symptoms related to urinary tract infections. Hematuria may result from tumor infiltration into the renal collecting system [2,3]. Risi et al. reviewed 116 cases of renal EWS and reported the most common clinical symptoms as pain (54%), hematuria (29%), and renal mass (28%) [10]. Approximately 66% of patients present with distant metastasis, with the lungs being the most common site, followed by the liver and bones. Upon reviewing 46 cases of renal EWS in this study [2,3,6,7,[11], [12], [13], [14], [15], [16], [17], [18], [19], [20], [21]] (Table 1, Table 2), the mean age was found to be 28.8 years, without a gender predilection, which is slightly different from the findings mentioned previously. In line with the Risi et al. study [10], the prevalent symptoms were flank pain (45.6%), followed by hematuria (34.8%), abdominal pain (15.2%), and a palpable mass (10.9%). In 45 cases (98%), the involvement was unilateral, while it was undetermined in the other case. Both sides were equally affected, with a mean mass size of 11 cm. In total, 30 cases (65%) had metastasis, consistent with the literature, with the lung being the most commonly involved organ (45.7%), followed by bone/bone marrow (24%) and lymph nodes (15.2%). The present case was a female (31 years old) who presented with right loin pain for a month without any other symptoms.Table 1. Review of 46 cases of primary renal Ewing sarcoma.Table 1. Author/referenceAge (year)/SexMCCImaging findingsTumor size (cm)DFDMETManagementFollow upAithal et al. [2]40/FHematuriaAn enhancing lesion extending into the renal hilum, showingvein thrombosis5.7RCCNoRNTN/AKhudair et al. [3]38/FAbdominal pain, ConstipationA large heterogeneous noncalcific exophytic mass20RCCLung, lymph nodesVDC, MESNA, IE.DiedEl Mohtarim et al. [11]14/FAbdominal pain and swelling, anorexia, weight lossA large lobulated retroperitoneal tumor16.5N/ALung, lymph nodesVAC, IE, RNTNo recurrence after 6 monthsBray et al. [12]31/FHematuria, flank painHeterogeneous, solid, echogenic mass with internal vascularity12RCC or AngiomyolipomaNoRNT, VDC, IENo recurrence after 12 monthsIlhan et al. [13]54/MHematuria, flank painHeterogeneously enhancedhyperdense cystic mass lesion7RCCNoRNT, VAC, IENo recurrencePatra et al. [14]33/FAbdominal painHeterogenousmass with hemorrhage and necrosis7.4N/ALung, bowel serosaRNT, CTDied35/MPalpable lump4.5N/ANoRNT, CTNo recurrence19/MPalpable lump, hematuria19N/ALiverVDC, etoposide, RNTLWD28/MAbdominal pain6.4N/ABoneVDC, etoposide, RNTLWDSardana et al. [7]49/MHematuria, flank painA lobulated mass6.3RCCNoRNT, CTNo recurrenceAlahmadi et al. [6]16/MHematuria, flank painA large heterogeneous mass15RCC/ Wilms tumor/sarcomaNoRNT, etoposide, MESNA, VDCNo recurrenceBradford et al. [15]16/MAbdominal painN/AN/AWilms tumorLung, bonePNT, vincristine, actinomycin, VDC, IE, irinotecan, temozolomideDied11/MFlank and testicle painA large massN/AN/AN/ARNT,VDC,IE,busulfan,melphalan,thiotepa,Everolimus, VIT, VTCRecurred after 60 months18/FHematuria, flank painN/A7.5N/ALungRNT, VDC, IENo recurrence after 56 months17/FKidney diseaseN/AN/AN/ANoVDC, IENo recurrence after 70 months16/FRenal massN/AN/AN/ALungVDC, IE, RNTNo recurrence after 22 months13/FAbdominal and back pain, lower extremity neuralgia,neurogenic bladder, ataxia.A large heterogeneous massN/AN/ABone, bone marrow, lungs, liverVDC, IE, RNT, ureterectomyDied15/FAbdominal and back pain, ataxiaA large renal mass, complete occlusion of the inferior vena cava,bilateral pulmonary metastasisN/AN/ALung, bone marrowRNT, partial ureterecomy,VDC, IE, cyclophosphamideRecurred after 6 months, and the case died after 30 months from presentationCheng et al. [16]31/FFlank pain, abdominal massA hypoechoic mass with central necrosis15.4N/ALymph node, neck, adrenal gland, psoas major, diaphragm, lungRNT, VAC,IE, carboplatin, antiangiogenic drug, apatinibNo recurrence after 18 monthsDoroudinia et al. [17]27/FHematuria, flank painN/A7.3Sarcomatous tumorNoRNT, VDC, IENo recurrenceSuzuki et al. [18]45/FAbdominal painA renal mass with contrast enhancement9.8RCCNoPNTNo recurrence after 12 monthsMurugan et al. [19]a41/MFlank painN/A12N/AMeninges, boneCTDied35/MFlank painN/A17N/ALung, lymph nodesRNT, CTDied43/MFlank painN/A20N/ABone, lungCTDied33/MFlank painN/AN/AN/ALung, brain, liver, skinRNT, CTDied70/FFlank painN/AN/AN/ALungRNT, CT, INFDied21/MFlank painN/A7.2N/APeritoneumRNT, CTDied23/MFlank painN/A9N/ALungRNT, CTDied45/MFlank painN/AN/AN/AAdrenal gland, lymph nodesRNT, CTDied31/FFlank painN/A12.5N/ANoRNT, CTNo recurrence after 108 months32/FFlank painN/A12N/ALung, lymph nodesRNT, CTDied50/MFlank painN/AN/AN/AN/AN/AN/A52/FFlank painN/AN/AN/ALung, liverRNT, CT, INFDied25/MFlank painN/A11.4N/ALungRNT, CTDied26/FHematuriaN/A11N/ANoRNT, CTNo recurrence after 48 months29/MHematuriaN/A9.2N/ALungRNT, CTN/A8/MHematuriaN/AN/AN/ABoneRNT, CTN/A9/FHematuriaN/A19N/ABoneRNT, CT, RTN/A18/FHematuriaN/A5N/ABone, lymph node, brainRNT, CT, RTLWD33/FHematuriaN/A8.5N/ALungRNT, CTN/A32/MHematuriaN/A15N/ANoRNT, CTNo recurrence after 14 months19/MHematuriaN/A6N/ALung, boneRNT, CT, RTDied33/FPalpable massN/AN/AN/ALungRNT, CTDied24/FPalpable massN/A14N/ANoRNT, CTNo recurrence after 156 monthsSadiq et al. [20]14/FFlank painA largeheterogeneous mass with a large necrotic component8N/AAbdominal wallNonradical nephrectomy, VDC, IEN/AYoshihara et al. [21]14/FAbdominal painA mass with contiguousextension through the renal vein into the inferior vena cava8.9Wilms’ tumor, clear cell sarcoma, RCCNoRNT, VDC, IENo recurrence after 70 monthsMCC, main chief complaint; N/A, nonavailable; DFD, differential diagnosis; RCC, renal cell carcinoma; RNT, radical nephrectomy; VAC, (vincristine, actinomycin D, cyclophosphamide); VDC, (vincristine, doxorubicin, cyclophosphamide); IE, (ifosfamide, etoposide); MESNA, Sodium 2-mercaptoethane sulfonate; MET, metastasis; LWD; live with disease; NACT, neoadjuvant chemotherapy; CT, chemotherapy (unknown type); PNT, partial nephrectomy; VIT, (vincristine, irinotecan, and temozolomide); VTC, (vincristine, topotecan, and cyclophosphamide); INF, interferon therapy; RT, radiotherapy.aThe symptoms for that study were randomly distributed among the cases as they were not specified for each case in the original study.Table 2. Summary of the reviewed cases.Table 2. VariablesFrequency / PercentagePatient demographicsAge (mean ± SD)28.8 ± 13.5Sex Male21 (46.0%) Female25 (54.0%)Main chief compliant/ symptomsa Flank pain21 (45.6%) Hematuria16 (34.8%) Abdominal pain7 (15.2%) Palpable mass5 (10.9%) Others12 (26%)Laterality Right23 (50.0%) Left22 (48.0%) N/A1 (2.0%)Tumor size, range (mean ± SD) cm4.5 – 20 (11 ± 4.6)Differential diagnosisa Renal cell carcinoma8 (17.4%) Wilms tumor3 (6.5%) Sarcoma3 (6.5%) Angiomyolipoma1 (2.0%)Metastatic casesa Lung21 (45.7%) Bone/bone marrow11 (24%) Lymph nodes7 (15.2%) Liver3 (6.5%) Brain2 (4.3%) Adrenal gland2 (4.3%) Others8 (17.4%)Management Nephrectomy alone2 (4.3%) Nephrectomy with chemotherapy39 (85.0%) Chemotherapy alone4 (8.7%) N/A1 (2.0%)Positive immunohistochemistrya CD9935 (76.0%) FLI-110 (21.7%) NKX 2-27 (15.2%) Synaptophysin6 (13.0%) Vimentin4 (8.7%) Others8 (17.4%)Follow up Alive21 (45.7%) Died18 (39.1%) N/A7 (15.2%) Recurrence2 (4.3%)SD, standard deviation; N/A, nonavailable.aIn each case, multiple options for each marker may be present.
Imaging should not be the primary diagnostic tool for renal EWS due to the lack of specific imaging features, which can result in misdiagnosis. Instead, greater emphasis should be placed on histopathology, IHC, and cytogenetic studies to confirm the diagnosis. Hence, most cases are diagnosed postoperatively [3]. Microscopically, most cases are characterized by uniform small round cells with round nuclei, finely stippled chromatin, inconspicuous nucleoli, minimal clear or eosinophilic cytoplasm, and indistinct cytoplasmic membranes [11]. The common differential diagnoses for renal EWS include Wilms tumor, neuroblastoma, clear cell sarcoma, lymphoma, rhabdomyosarcoma, the small cell variant of osteosarcoma, desmoplastic small round cell tumor, small cell neuroendocrine carcinoma, and nephroblastoma. The tumor cells may be arranged in Homer-Wright rosettes, and IHC often shows strong positivity for CD99 and FLI-1. New markers, such as NKX2.2, have further improved diagnostic accuracy [2,11]. NKX2.2 is a protein involved in regulating gene expression within the neuroendocrine and glial differentiation pathway. NKX2.2 is a specific marker for targeting the fusion protein EWS-FLI-1, demonstrating a high sensitivity of 93% and specificity of 89%. However, fluorescent in situ hybridization (FISH) represents the gold standard method, exhibiting high sensitivity (92.3%) and specificity (100%) [11]. Among the reviewed cases, the tumors in 10 cases were preoperatively suspected to be either renal cell carcinoma (17.4%), Wilms tumor (6.5%), sarcoma (6.5%), or angiomyolipoma (2%). In the present case, the MRI features of the cyst (9 cm) were suggestive of a hydatid cyst rather than a complicated cyst. It was a thick-walled cystic lesion with thin peripheral septa; however, the cyst lacked daughter cysts, floating membranes, or peripheral calcification of the cyst wall. The echinococcal serological test was negative.
There is no consensus on the optimal treatment for renal EWS. However, the standard approach involves a multimodal strategy comprising surgical resection, nephrectomy, chemotherapy, and radiotherapy. Chemotherapy typically alternates between VDC (vincristine, doxorubicin, cyclophosphamide) and IE (ifosfamide, etoposide) regimens. This alternating regimen has been shown to enhance outcomes in nonmetastatic EWS [3]. Nevertheless, this regimen is linked to several hematological and nonhematological toxicities. Grade 3 and 4 hematological toxicities, including anemia, thrombocytopenia, and neutropenia, are frequent. Nonhematological toxicities include bacteremia, urinary tract infections, mucositis, and fever [22]. Furthermore, if venous thrombosis is present alongside pulmonary metastasis, cavotomy may be incorporated into the surgical procedure. When surgical margins are positive or there is localized lymph node involvement, radiotherapy should be administered as salvage therapy. However, opinions differ regarding radiotherapy as the first-line treatment option [13]. The prognosis of EWS remains poor, especially if metastasis is present, with a cure rate of only 20% and an overall 5-year survival [2,23]. In our review, 85% of the cases were managed with a combination of nephrectomy and chemotherapy. Only six cases (13%) underwent a single modality of therapy (8.7% chemotherapy alone and 4.3% nephrectomy alone). The IHC staining was positive for CD99 in 76% of the cases, FLI-1 in 21.7%, NKX2-2 in 15.2%, synaptophysin in 13%, and vimentin in 8.7%. Among the cases with a known prognosis (84.8%), nearly half of the cases (39.1%) died due to the disease. Recurrence was found in two cases: one died, and the other’s destination was unknown. As there were no signs of metastasis on the imaging findings of the present study, the patient underwent an excisional biopsy followed by a partial nephrectomy without a lymph node dissection. A diagnosis of primary renal EWS was made on the excisional specimen. The IHC staining was positive for CD99 and FLI-1 (in >50% of tumor cells) and negative for AE1/AE3, INI-1 loss, WT1, desmin, myogenin, BCOR, TLE-1, CD45CLA, and synaptophysin. The patient received 21 cycles of VAC/IE without side effects. The case remains disease-free with no signs of recurrence or metastasis after one year of follow-up. This report's limitation is the absence of a FISH test due to its high cost to the patient.
Conclusion
Primary renal EWS is a rare disease with a poor prognosis. Early detection and management may increase the chances of preventing metastasis and enhancing overall survival. However, imaging findings may not be reliable for an accurate diagnosis, as the disease can mimic a hydatid cyst, among other common differential diagnoses. For radiologists, any large, atypical cystic renal lesion in a young patient that does not entirely fit benign or infectious patterns, should raise suspicion for rare primary renal tumors, including sarcomas, and necessitate multidisciplinary evaluation.
Patient consent
Informed consent was taken from the patient to publish any accompanying data and images.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ali Rebaz M.Hussein Zhino Noori Ali Jalil Salih Saida Bnar Sardar Fakhralddin Saman S.Ali Rawa M.Renal Ewing sarcoma: a case report and literature review Barw Med J 3320255155
- 2Aithal V.Sajitha K.Mathias M.Ewing sarcoma of kidney: a rare entity J Health Allied Sci NU 1412024 s–0044–1786993
- 3Khudair A.D.Khudair A.D.Al-Rawahia T.Marshall R.A.Albenjasim K.Roohi M.Unveiling the uncommon: a case of metastatic ewing sarcoma of the kidney Cureus 1612024 e 5297010.7759/cureus.52970 PMC 1089444538406149 · doi ↗ · pubmed ↗
- 4Alghamdi M.H.Alawad S.A.Alharbi M.G.Alabdulsalam A.K.Almodhen F.Alasker A.A rare case of Ewing's sarcoma of the kidney Urol Case Rep 29202010109410.1016/j.eucr.2019.101094 PMC 692833831890597 · doi ↗ · pubmed ↗
- 5Cochetti G.Paladini A.de Vermandois J.A.Fatigoni S.Zanelli M.Ascani S.Metastatic renal Ewing’s sarcoma in adult woman: case report and review of the literature Open Med 161202139740910.1515/med-2021-0207 PMC 795719233748424 · doi ↗ · pubmed ↗
- 6Al Ahmadi H.H.Al Essa A.Ahmed A.Fadaak K.El Darawany H.M.Alhamam A.Primary Ewing sarcoma/primitive neuroectodermal tumor of the kidney J Pediatr Surg Case Rep 612020101608
- 7Sardana R.Parwani A.V.Shabsigh A.Sheldon J.An unusual case of renal Ewing sarcoma: a case report and review of literature Hum Pathol: Case Rep 252021200537
- 8Prasad S.Nassar M.Azzam A.Y.García-Muro-San José F Jamee M.Sliman R.K.Ca Re L Guidelines: a consensus-based guideline on case reports and literature review (Ca Re L)Barw Med J 2220241319