Heartmate 3 left ventricular assist device system in patients with glucose-6-phosphate dehydrogenase deficiency
Elena Grasso, Roberto Lorusso, Ahmed Ibrahim, Mohamad Ibrahem Abdelhamed, Hassane Abdallah, Omer Ali Sayin

TL;DR
This study examines the safety of a heart pump device in patients with a genetic enzyme deficiency that causes red blood cell breakdown.
Contribution
The study provides early evidence on the safety of Heartmate 3 LVADs in patients with G6PD deficiency, a previously understudied population.
Findings
Five G6PD-deficient patients received LVADs without major complications during hospitalization.
No macroscopic hemolysis occurred during follow-up despite the patients' condition.
Two patients died, two devices were removed, and one received a heart transplant during follow-up.
Abstract
Glucose-6-phosphate dehydrogenase (G6PD) deficiency is a genetic enzymatic disorder that affects millions of people worldwide and characterized by hemolysis under oxidative stress. Left ventricular assist devices (LVADs) have substantially enhanced survival and quality of life for individuals with advanced heart failure. However, their use is associated with the risk of hemolysis, thrombosis, and embolic events. These risks may be heightened in patients with glucose-6-phosphate dehydrogenase (G6PD) deficiency. Given the limited published research on this subject, the primary objective of this study was to assess the degree of hemolysis and identify associated factors in adult patients with glucose-6-phosphate dehydrogenase (G6PD) deficiency who underwent Heartmate 3 (HM3) left ventricular assist device (LVAD) implantation. This retrospective, observational, single-center study was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
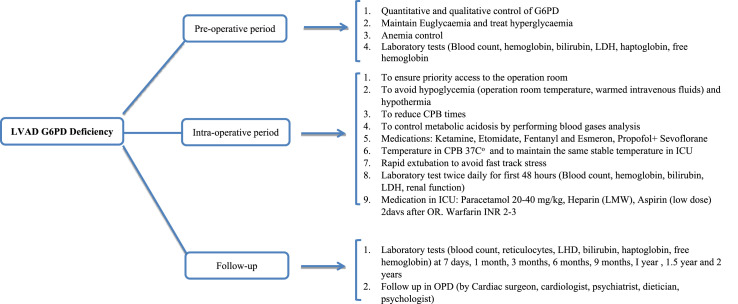 Figure 1
Figure 1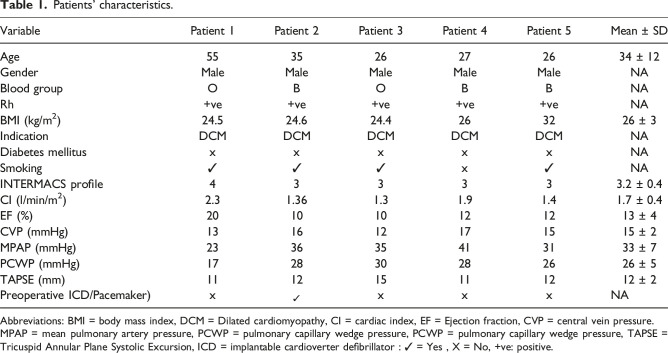 Figure 2
Figure 2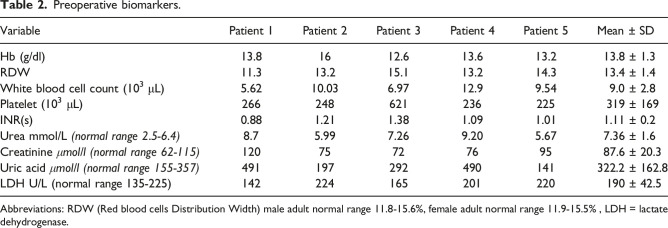 Figure 3
Figure 3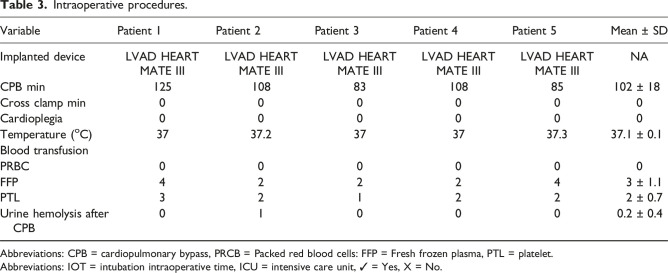 Figure 4
Figure 4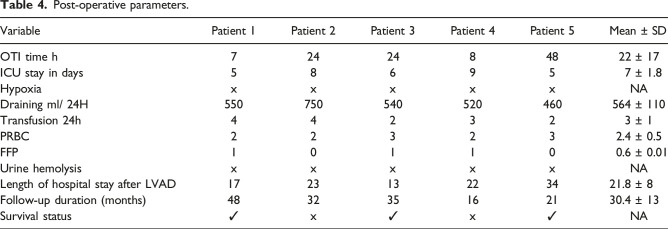 Figure 5
Figure 5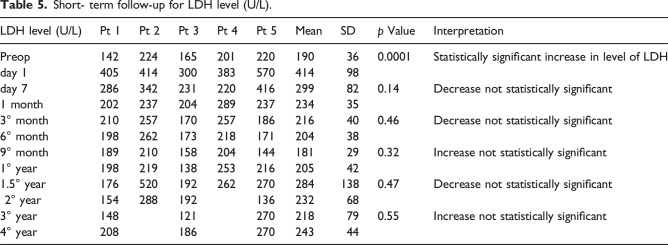 Figure 6
Figure 6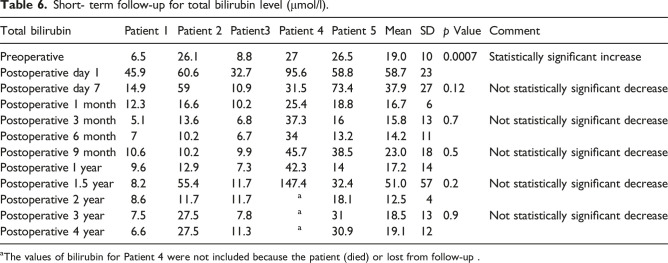 Figure 7
Figure 7Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMechanical Circulatory Support Devices · Cardiac Structural Anomalies and Repair · Transplantation: Methods and Outcomes
Introduction
Durable mechanical circulatory support (MCS) and ventricular assist devices (VADs) have evolved significantly since their introduction over two decades ago. They are now considered viable options for patients with advanced heart failure who are ineligible for transplantation or unable to wait for a donor.^1,2^ However, hemolysis has become an increasingly recognized complication of LVAD_s_ support.^ 3 ^ The incidence of hemolysis varies (5%-18%) depending on the definition and among different generations of LVADs, being slightly higher in continuous-flow than to pulsatile devices.^ 4 ^ There is no reliable prediction or algorithm available for the occurrence or management of hemolysis in patients with LVADs. However, careful clinical and laboratory monitoring remain the cornerstone of patient management in this respect. G6PD deficiency is one of the common human enzyme deficiency disorders with variable prevalence in the middle east and Mediterranean countries.^ 5 ^ This condition might represent a risk factor of exacerbation of hemolysis in LVAD recipients.^ 6 ^ In order to provide a larger, albeit still very limited series, the aim of this case series was to provide a larger clinical investigation on hemolysis and related biomarkers in G6PD deficiency adult patients submitted to left VAD HeartMate 3 (HM3) at our center and followed up after hospital discharge.
Methods
This study presents a retrospective, single-center case-control analysis of 28 HM3 LVAD implants performed at our center since 2017. Of these patients, four (14%) had G6PD deficiency and one (3%) had SCT associated G6PD deficiency. Given the high prevalence of G6PD deficiency in Saudi Arabia, routine qualitative testing was performed on all patients to confirm the presence of this enzyme deficiency. Notably, none of the patients were clinically symptomatic for G6PD deficiency.
The data presented in Table 1 were collected in all patients and retrospectively reviewed from the electronic database. The Interagency Registry for Mechanically Assisted Circulatory Support (INTERMACS) defines hemolysis as a plasma free Hgb ≥40 mg/dl in association with clinical signs of hemolysis ≥72 hours after implantation.^5,6^ For the purposes of this study, we defined hemolysis according to our institutional protocol, which includes patients with the following 3 parameters: unexplained anemia (Hgb <10 g/dl) in the absence of obvious bleeding, total bilirubin (≥1 mg /dl) and high LDH (>250 u /l). Plasma-free Hgb data was not available for most patients, as they were referred to a laboratory and were not routinely monitored during the study period. Besides, we evaluated the onset of macroscopic hematuria.Table 1.Patients’ characteristics.VariablePatient 1Patient 2Patient 3Patient 4Patient 5Mean ± SDAge553526272634 ± 12GenderMaleMaleMaleMaleMaleNABlood groupOBOBBNARh+ve+ve+ve+ve+veNABMI (kg/m^2^)24.524.624.4263226 ± 3IndicationDCMDCMDCMDCMDCMNADiabetes mellitusxxxxxNASmoking✓✓✓x✓NAINTERMACS profile433333.2 ± 0.4CI (l/min/m^2^)2.31.361.31.91.41.7 ± 0.4EF (%)201010121213 ± 4CVP (mmHg)131612171515 ± 2MPAP (mmHg)233635413133 ± 7PCWP (mmHg)172830282626 ± 5TAPSE (mm)111215111212 ± 2Preoperative ICD/Pacemaker)x ✓ xxxNAAbbreviations: BMI = body mass index, DCM = Dilated cardiomyopathy, CI = cardiac index, EF = Ejection fraction, CVP = central vein pressure.MPAP = mean pulmonary artery pressure, PCWP = pulmonary capillary wedge pressure, PCWP = pulmonary capillary wedge pressure, TAPSE = Tricuspid Annular Plane Systolic Excursion, ICD = implantable cardioverter defibrillator : ✓ = Yes , X = No, +ve: positive.
Surgical and anesthetic management and cardiopulmonary bypass
All patients received assigned cardiac medications until the morning of surgery. G6PD positive patients were prioritized in the operating room to reduce the preoperative stress response. In the weeks leading up to the surgery, the antidiabetic therapy was modified applying an aggressive treatment against perioperative hyperglycemia (tight glycemic control). In the period of preoperative preparation of the patient, the availability of cross- matched blood products was ensured in order to be ready in the event of significant pre or perioperative hemolysis. None of the patient received blood or any blood products transfusion preoperatively. Upon arrival in the operating room, a close temperature control (intraoperative use of warming blankets) was implemented.^ 7 ^ After intubation, all patients were ventilated with 100% oxygen throughout the operation, except during the extracorporeal circulation. All invasive procedures were performed while the patients were under deep anesthesia to avoid oxidative stress.^8,9^ Blood gas checks were repetitively executed to detect acidosis and hyperglycemia, which are potential precipitating factors for hemolysis. Perioperative changes in temperature, hemodynamics, respiratory and metabolic parameters were recorded. The nasopharyngeal temperature was kept at 37°C during the entire bypass time.^9–11^ All patients underwent cardiac surgery through full median sternotomy and received the VAD system HM3. Immediately after coming off CPB, the patient urine was checked regarding any signs of hematuria. Patients were extubated when optimal cognitive, hemodynamic, and respiratory functions were achieved. For postoperative pain management, paracetamol was administered with minimal dose 20-40 mg/kg/day and low-dose aspirin (ASA) was stared on day 2 post intervention^ 12 ^ and warfarin with a target INR of 2.0-3.0 unless bleeding complications occur.
Statistical data analysis
Data was analyzed using SPSS version, descriptive data analysis presented in form of mean ± SD, Number proportion and percentages. We assessed, biomarkers including (LDH, hemoglobin, bilirubin, Platelets) at Baseline, day1, day7, month1, month3, month6, month9, 1year1, 1.5 year, 2 years, 3 years and 4 years, statistical comparison was performed using t-tests. Confidence level was set at 95%, p-value <.05 was considered statistically significant.
Results
Base‐line pre‐LVAD implantation patients' characteristics were presented in Table 1. Five male patients with DCM associated with G6PD were included in this study. Preoperative evaluation was conducted for each patient (Table 2). Table 3, shows intraoperative procedures. All patients underwent LVAD HM3 implantation. No blood or blood product transfusions were administered to any of the patients during the surgical procedure. Cardiopulmonary bypass induced hemolysis as observed in urine analysis assessed upon ICU arrival; only Patient two showed bypass induced hemolysis. We did not analyze the urine, which appeared bloody. Table 4 shows, post-operative parameters, the mean intraoperative time (IOT) was 39 minutes (median 22; range: 7- 48). Mean intensive care unit length of stay was about 7 days. Mean drainage was 564 mL/ 24 hours. Blood transfusion data are represented in Table 4. Anticoagulation for LVAD was started with low molecular weight heparin on the ICU after 12–24 h, depending on bleeding amount. Antiplatelet drugs and oral anticoagulants were started on the second postoperative day, unless bleeding complications occur. There was neither mortality nor complication within 30 days, 3 months and 6 months postoperatively. Fortunately, there were no in-hospital deaths.
- Patient 1: surgery went very smoothly and the patient recovered and his LVAD was decommissioned after 40 months of surgery.^ 13 ^
- Patient 2: There was a noticeable hematuria in the ICU. Then, the patient developed drive-line infection and his culture revealed methicillin-resistant staphylococcal (MRSA) infection. Subsequently, his condition was complicated with abdominal abscess and then cerebral hemorrhage which was the direct cause of death (died after 32 months of follow-up).
- Patient 3: decommissioning was done after 12 months of surgery.^ 13 ^
- Patient 4: The patient suffered right sided heart failure and advanced to hepatic failure and cerebral hemorrhage which caused his death after 16 months of surgery.
- Patient 5: who had history of toxic substance intoxication and exhibited both G6PD deficiency and SCT, was the only patient in the study to undergo a heart transplant after less than two years of receiving a LVAD. Table 2.Preoperative biomarkers.VariablePatient 1Patient 2Patient 3Patient 4Patient 5Mean ± SDHb (g/dl)13.81612.613.613.213.8 ± 1.3RDW11.313.215.113.214.313.4 ± 1.4White blood cell count (10^3^ μL)5.6210.036.9712.99.549.0 ± 2.8Platelet (10^3^ μL)266248621236225319 ± 169INR(s)0.881.211.381.091.011.11 ± 0.2Urea mmol/L (normal range 2.5-6.*4)*8.75.997.269.205.677.36 ± 1.6Creatinine *μmol/l (normal range 62-115)*1207572769587.6 ± 20.3Uric acid *μmol/l (normal range 155-357)*491197292490141322.2 ± 162.8LDH U/L (normal range 135-225)142224165201220190 ± 42.5Abbreviations: RDW (Red blood cells Distribution Width) male adult normal range 11.8-15.6%, female adult normal range 11.9-15.5% , LDH = lactate dehydrogenase.Table 3.Intraoperative procedures.VariablePatient 1Patient 2Patient 3Patient 4Patient 5Mean ± SDImplanted deviceLVAD HEART MATE IIILVAD HEART MATE IIILVAD HEART MATE IIILVAD HEART MATE IIILVAD HEART MATE IIINACPB min1251088310885102 ± 18Cross clamp min000000Cardioplegia000000Temperature (^o^C)3737.2373737.337.1 ± 0.1Blood transfusionPRBC000000FFP422243 ± 1.1PTL321222 ± 0.7Urine hemolysis after CPB010000.2 ± 0.4Abbreviations: CPB = cardiopulmonary bypass, PRCB = Packed red blood cells: FFP = Fresh frozen plasma, PTL = platelet.Abbreviations: IOT = intubation intraoperative time, ICU = intensive care unit, ✓ = Yes, X = No.Table 4.Post-operative parameters.VariablePatient 1Patient 2Patient 3Patient 4Patient 5Mean ± SDOTI time h7242484822 ± 17ICU stay in days586957 ± 1.8HypoxiaxxxxxNADraining ml/ 24H550750540520460564 ± 110Transfusion 24h442323 ± 1PRBC223232.4 ± 0.5FFP101100.6 ± 0.01Urine hemolysisxxxxxNALength of hospital stay after LVAD172313223421.8 ± 8Follow-up duration (months)483235162130.4 ± 13Survival status✓x✓x✓NA
Finally, patients 1 and 3 who had lower preoperative LDH, lower bilirubin levels, and higher follow-up Hb had improvement in heart failure leading to VAD deactivation, at 40 months and 12 months, respectively months after implantation.
Discussion
This case series of five patients with G6PD deficiency and chronic heart failure receiving durable VADs represents the first reported experience with a suggested management pathway for this combination in patients undergoing LVAD implantation. It is estimated that about 400 million people are affected by G6PD deficiency worldwide.^ 14 ^ This genetic condition is inherited as an X-linked recessive state, and presents one of the most frequently encountered red-cell enzymopathies. The major interest in the G6PD-deficient state results from the associated hemolytic anemia resulting from oxidative stress.^15,16^ It is worth mentioning that, hemolysis-induced thrombotic events in G6PD patients occur when hemolysis releases free hemoglobin into the bloodstream. This free hemoglobin binds to haptoglobin, forming methemoglobin. When haptoglobin is saturated, free methemoglobin can precipitate in the microcirculation. These precipitates can activate platelets and clotting factors, leading to thrombus formation.^ 14 ^ As mentioned, mechanical circulatory devices have been shown to induce, in some occasion, marked shear stress and, subsequently, blood elements damage.^15–17^
In our center we have implanted only HM3 devices since 2017.
The HM3 is a third-generation continuous flow centrifugal LVAD with the rotor suspended in the bloodstream using a non-contact design via magnetic levitation. The main advantages of this type of system are non-contact bearings, easy changes in pump speed to modulate an artificial pulse, and the smaller size of the device
When it comes to the effect of the LVAD device itself, the HeartMate 3 LVAD is renowned for its superior hemocompatibility, which is attributed to its innovative design features. These include a magnetically levitated rotor that minimizes blood damage, textured blood-contacting surfaces that reduce shear stress, and optimized fluid dynamics that promote smooth blood flow. These design elements contribute to a reduced risk of hemolysis, thrombosis, and other blood-related complications, ultimately improving patient outcomes.^7,18,20^
In fact, according to Uriel N.et al. in the secondary analysis of the MOMENTUM 3 study, HM3 Left ventricular assist System (LVAS) demonstrated greater freedom from HRAEs (hemocompatibility-related clinical adverse events) compared to HMII LVAS at 6 months.^ 21 ^ We used this LVAD in all patients in the series and ventured to include it also in a restricted population with G6PD deficiency. From the analysis in our possession, we have highlighted that for the best management of this small number of patients it would be useful to propose a management flow chart (Figure 1). From our limited case series, patients with G6PD who are candidates for LVAD implantation must follow a dedicated pathway as those with sickle cell disease should.^ 22 ^ In particular, initially all patients must absolutely avoid postoperative hypoxemia (Spo2 ≤ 90% or a Po2 ≤ 60 mmHg). VAD implantation requires the use of extracorporeal circulation which activates the inflammatory response.^18,23^ One of the end results of this process is endothelial damage. Apparently, the lungs are the main organ affected and sustained by this damage.^ 10 ^ A study by Gerrah et al.^ 11 ^ indicates that CPB is a causal factor of hypoxia in patients with G6PD deficiency, leading to increased hemolysis. As a result, these patients lose lung oxygenation reserve, as seen with a lower than normal minimum PaO2 individuals. To avoid this, we shortened CPB times and extubated patients relatively quickly to avoid the increase in free radicals that would be added to those undergoing long-term CPB.^ 24 ^Figure 1.Follow chart of LVD implantation in patient with G6P Deficiency.
Secondly, anemia (HB less than 8 g/dl) should be avoided in the pre-, intra- and postoperative periods. Our patients did not receive red blood cell transfusions in the pre- and intraoperative period, and we used the cell salvage system with the aim of avoiding or limiting any predisposing factors related to hemolysis. Furthermore, hypothermia, commonly established during cardiac surgery, also constitutes a risk factor for hemolysis in patients with G6PD deficiency. Gerrah et al.,^ 11 ^ in their study of 42 patients, described a positive correlation between hypothermia and postoperative hemolysis. The average temperature during bypass in the study group was 26.7 ± 2.4°C. In our patients, the nasopharyngeal temperature was 32-34°C during the bypass period, and our patients did not show any signs of hemolysis. The link between G6PD deficient and hemolysis in the context of mechanical circulatory support (MCS) is not entirely new^ 19 ^ and we hypothesize that hemolysis resulted, at least in part, from an unfavorable oxidative environment after LVAD implantation rather than from shear stress alone.^ 23 ^ Indeed, it may be useful in the future to obtain peripheral blood smears (Heinz bodies and bite cells) which in many of these patients would confirm oxidative hemolysis rather than mechanical destruction, an analysis that should be performed pre- and post-operatively (Figure 1). Hemolysis is an important complication of continuous flow LVADs in all patients.^ 4 ^ Ravichandran et al.^ 6 ^ demonstrated that hemolysis after LVAD is associated with a high 1-year mortality that is more than 2 times greater than that observed for the non- hemolyzing HM3 patients. In addition, in light of our current findings, we now use aspirin 81 mg and warfarin with a goal INR of 2.0–3.0 unless bleeding complications arise. High doses of ASA were not allowed in deficient patients but low dose of ASA cause no hemolysis.^ 12 ^ We also dose bridging anti-coagulation until an INR of two is achieved.^20,25^
Furthermore, our results suggest that G6PD deficiency does not negatively impact post-implant outcomes or increase the risk of hemolysis-related complications in LVAD patients. No significant increase in hemolysis biomarkers was observed during in-hospital follow-up or post-discharge, and no major hemolysis-related complications occurred in these patients.
It was observed that, Patient 4 with higher mean bilirubin, lower mean Hb and lower mean PTL associated with the smoking factor, was the only one who died from a thromboembolic event. Interestingly, we didn’t find any correlation with smoking but aggressive smoking cessation should be used in all patients with LVAD support.^ 3 ^
Finally, based on our experience, we believe that the following concepts are beneficial in the management of patients with G6PD deficiency and undergoing LVAD implantation, despite the small sample size a single-center design:
-
- Establish a pre- and post-operative management protocol for the category of patients with G6PD deficient.
-
- Anyone suspected of G6PD deficiency, with a family history of the disorder, a history of hemolysis, and/or of African, southern European, Middle Eastern, southeast Asian, or central and southern Pacific Island descent, should be screened for G6PD deficiency.
-
- Avoid perioperative hypothermia, acidosis, hyperglycemia and postoperative infection can precipitate haemolysis in the G6PD-deficient patient.
-
- LDH, bilirubin, and haptoglobin, are strong markers for hemolysis and can be regularly obtained to survey for this potentially deadly diagnosis.
These findings may have implications for the evaluation of LVAD candidacy and may suggest more intensive postoperative surveillance for patients implanted with G6PD deficiency as we described in proposed the flow chart.
Conclusion
In addition to oxidative stress, our study also considered the effects of mechanical stress exerted by the LVAD on patients with G6PD deficiency and chronic heart failure. We demonstrated that LVADs can be safely used in this patient population by implementing a more controlled approach and stringent support protocols to minimize complications. (Table 5 and 6).Table 5.Short- term follow-up for LDH level (U/L).LDH level (U/L)Pt 1Pt 2Pt 3Pt 4Pt 5MeanSDp ValueInterpretationPreop142224165201220190360.0001Statistically significant increase in level of LDHday 140541430038357041498day 7286342231220416299820.14Decrease not statistically significant1 month202237204289237234353° month210257170257186216400.46Decrease not statistically significant6° month198262173218171204389° month189210158204144181290.32Increase not statistically significant1° year198219138253216205421.5° year1765201922622702841380.47Decrease not statistically significant 2° year154288192136232683° year148121270218790.55Increase not statistically significant4° year20818627024344Table 6.Short- term follow-up for total bilirubin level (μmol/l).Total bilirubinPatient 1Patient 2Patient3Patient 4Patient 5MeanSDp ValueCommentPreoperative6.526.18.82726.519.0100.0007Statistically significant increasePostoperative day 145.960.632.795.658.858.723Postoperative day 714.95910.931.573.437.9270.12Not statistically significant decreasePostoperative 1 month12.316.610.225.418.816.76Postoperative 3 month5.113.66.837.31615.8130.7Not statistically significant decreasePostoperative 6 month710.26.73413.214.211Postoperative 9 month10.610.29.945.738.523.0180.5Not statistically significant decreasePostoperative I year9.612.97.342.31417.214Postoperative 1.5 year8.255.411.7147.432.451.0570.2Not statistically significant decreasePostoperative 2 year8.611.711.7 ^ a ^ 18.112.54Postoperative 3 year7.527.57.8 ^ a ^ 3118.5130.9Not statistically significant decreasePostoperative 4 year6.627.511.3 ^ a ^ 30.919.112^a^The values of bilirubin for Patient 4 were not included because the patient (died) or lost from follow-up .
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Maybaum S Kamalakannan G Murthy S . Cardiac recovery during mechanical assist device support. Semin Thorac Cardiovasc Surg 2008; 20: 234–246.19038734 10.1053/j.semtcvs.2008.08.003 · doi ↗ · pubmed ↗
- 2Krabatsch T Schweiger M Stepanenko A , et al. [Improvements in implantable mechanical circulatory support systems: literature overview and update]. Herz 2011; 36: 622–629.21912911 10.1007/s 00059-011-3509-5 · doi ↗ · pubmed ↗
- 3Katz JN Jensen BC Chang PP , et al. A multicenter analysis of clinical hemolysis in patients supported with durable, long-term left ventricular assist device therapy. J Heart Lung Transplant 2015; 34: 701–709.25582036 10.1016/j.healun.2014.10.002 · doi ↗ · pubmed ↗
- 4Pamboukian S Elliot T Mohacsi P , et al. The 2013 international society for heart and lung transplantation guidelines for mechanical circulatory support: executive summary. J Heart Lung Transplant 2013; 32(2): 157–187.23352391 10.1016/j.healun.2012.09.013 · doi ↗ · pubmed ↗
- 5Alangari AS El-Metwally AA Alanazi A , et al. Epidemiology of glucose-6-phosphate dehydrogenase deficiency in arab countries: insights from a systematic review. J Clin Med 2023; 12(20): 6648.37892786 10.3390/jcm 12206648 PMC 10607133 · doi ↗ · pubmed ↗
- 6Ravichandran AK Parker J Novak E , et al. Hemolysis in left ventricular assist device: a retrospective analysis of outcomes. J Heart Lung Transplant 2014; 33(1): 44–50.24418733 10.1016/j.healun.2013.08.019 · doi ↗ · pubmed ↗
- 7Zimpfer D Netuka I Schmitto JD , et al. Multicentre clinical trial experience with the Heart Mate 3 left ventricular assist device: 30-day outcomes. Eur J Cardio Thorac Surg 2016; 50(3): 548–554.10.1093/ejcts/ezw 16927436871 · doi ↗ · pubmed ↗
- 8Sahin S Inal M Kaya G , et al. Anesthesia management of a patient with glucose-6-phosphate dehydrogenase deficiency. Internet J Anesthesiol 2006; 14: 94–96.