Clinical relevance of intraoperative blood loss in pancreatic surgery: a systematic review and meta-analysis to reappraise the impact on post operative pancreatic fistula
Giampaolo Perri, Danhui Heo, Rayner Peyser Cardoso, Swizel Ann Cardoso, Antonio Facciorusso, Riccardo Pellegrini, Domenico Bassi, Umberto Cillo, Giovanni Marchegiani

TL;DR
This study finds that intraoperative blood loss is a significant predictor of postoperative pancreatic fistula after pancreatic surgery.
Contribution
The study provides updated evidence on the clinical relevance of intraoperative blood loss in predicting postoperative pancreatic fistula.
Findings
Intraoperative blood loss was significantly higher in patients who developed postoperative pancreatic fistula.
IBL was identified as an independent risk factor for POPF in 17 out of 26 studies reviewed.
The meta-analysis included 10,008 patients and confirmed the association between IBL and POPF.
Abstract
Postoperative pancreatic fistula (POPF) is the major complication following pancreatic surgery, significantly impacting patient outcomes. Intraoperative blood loss (IBL) represents a modifiable risk factor for POPF, but its actual clinical relevance is not clearly defined. This study explores the available literature to reappraise the association of IBL and the development of POPF. A systematic review and meta-analysis of original studies published between January 2006 and August 2025, reporting IBL in patients undergoing pancreatic resections and its association with POPF were performed. Studies that used the International Study Group on Pancreatic Surgery (ISGPS) or the International Study Group on Pancreatic Fistula Definition (ISGPF) definitions for POPF were included. Qualitative synthesis included all eligible studies; quantitative meta-analysis was conducted for studies…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
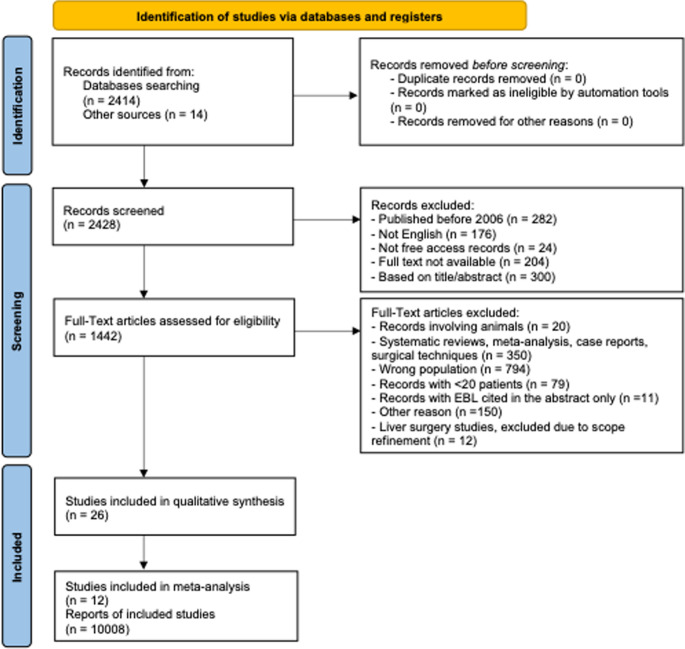 Figure 1
Figure 1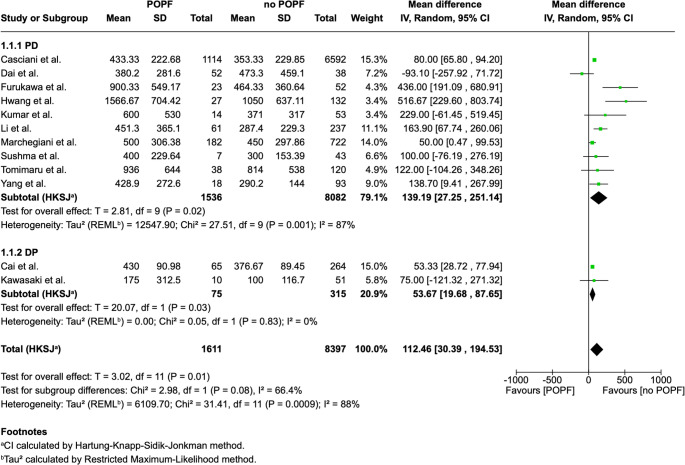 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPancreatic and Hepatic Oncology Research · Hemostasis and retained surgical items · Pancreatitis Pathology and Treatment
Introduction
Despite advances in surgical techniques, perioperative care, and anesthesia have significantly improved the outcomes, pancreatic surgery still is characterized by high rates of postoperative mortality and morbidity. Among these complications, postoperative pancreatic fistula (POPF) represents the most frequent and concerning complication after pancreatic surgery [1–3]. POPF is a dangerous complication that can trigger serious secondary problems. The leaked pancreatic fluid contains proteolytic enzymes that damage surrounding tissues and erode blood vessels, causing severe hemorrhage requiring emergency intervention [4, 5]. POPF also creates a persistent source of intra-abdominal infection, leading to abscess formation and sepsis [4, 6]. POPF management is complex and typically requires prolonged drainage, percutaneous interventions, and occasionally completion pancreatectomy, resulting in extended hospital stays and substantially elevated healthcare costs [7, 8]. Moreover, POPF has frequently been associated with delays in initiating adjuvant chemotherapy, or even the inability to receive it, which may adversely affect long-term oncologic outcomes [9].
Intraoperative blood loss (IBL) is a key factor influencing postoperative outcomes, particularly in hepato-pancreato-biliary (HPB) surgery, where it has been frequently associated with adverse perioperative outcomes [10–13]. In pancreatic surgery, high IBL may contribute to relative ischemia of the pancreatic remnant, potentially impairing healing of the pancreatico-enteric anastomosis [14, 15]. Furthermore, aggressive fluid resuscitation in response to blood loss can result in tissue edema [16, 17], while perioperative blood transfusions may induce immunosuppression [18, 19], both of which can further compromise anastomotic integrity.
However, the relationship between IBL and POPF remains controversial. While excessive IBL is often associated with increased postoperative morbidity and mortality, its direct impact on the development of POPF is not fully elucidated.
Therefore, this study aims to systematically review the existing literature and perform a meta-analysis to evaluate the clinical impact of IBL in pancreatic surgery, with particular focus on its association with the development of POPF.
Methods
Study design
A systematic literature search was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guidelines [20]. A protocol has been registered in PROSPERO (https://www.crd.york.ac.uk/PROSPERO/view/CRD42025649406). The study was initially designed to include HPB surgeries, encompassing both liver and pancreatic surgeries. However, during the full-text assessment showed that there were insufficient data on liver surgery outcomes to perform a meta-analysis. As a result, the scope of the study was narrowed to focus exclusively on pancreatic surgery. The flowchart and subsequent analyses were revised accordingly to reflect this refined focus.
The PubMed database was searched for full-text, English-written studies published before September 1, 2025. The search string is available as supplementary data (Supplementary Fig. 1). Although liver surgery was initially included in the search strategy, these studies were subsequently excluded as insufficient data were available to perform a meta-analysis on liver surgery outcomes. Studies were included if they applied either the International Study Group of Pancreatic Fistula (ISGPF) 2005 definition or the updated International Study Group of Pancreatic Surgery (ISGPS) 2016 definition for clinically relevant POPF (CR-POPF) [21, 22]. The primary outcome of interest was the occurrence of POPF. Studies were eligible if they reported IBL stratified by POPF versus no POPF, or by CR-POPF versus no CR-POPF. In the ISGPS 2016 definition, CR-POPF corresponds to grades B and C. For studies using the ISGPF 2005 classification, POPF grade B and C were also considered as CR-POPF. All studies published before January 1, 2006, case reports or descriptions of surgical techniques, series with < 20 patients, studies with IBL cited only in the abstract or not referring to pancreatic resections, duplicates, editorials, systematic reviews/meta-analyses, studies without free-access records, and animal studies were excluded from the systematic review.
During the screening at least two researchers (A.M., G.P., D.H., and R.P.C.) independently screened all the identified studies. After a first screening based on the title and abstract for assessing full-text eligibility, two researchers independently performed the full-text assessment (A.M., G.P., D.H., and R.P.C.). A final consensus was reached after discussion with a senior researcher (G.M.) in cases of any disagreement. Statistical analysis was performed by two authors (D.H., A.F.) including a second senior researcher (A.F.).
Statistical analysis
The risk of bias was determined using the ROBINS-I tool for cohort studies. The methodological quality of the included studies was evaluated independently by two authors (S.A.C and R.P.C) (Supplementary Fig. 2). The meta-analysis was conducted through a random-effects model using Restricted Maximum Likelihood Estimation (REML) to calculate mean difference (MD) and 95% confidence intervals (CI) between POPF vs. no-POPF in pancreatic surgery patients. If the outcomes were reported in medians with interquartile range (IQR) or 95% CI or range the mean and standard deviation values were calculated from the statistical estimations in accordance with the Cochrane manual and Wan et al. [23, 24]. Heterogeneity between study-specific estimates was estimated using the inconsistency index (I^2^), and cutoffs of < 30%, 30%–59%, 60%–75% and >75% suggested low, moderate, substantial, and considerable heterogeneity, respectively [25]. Publication bias was assessed qualitatively using funnel plot asymmetry (Supplementary Fig. 3). Additionally, the certainty of evidence for outcomes related to POPF was assessed using the updated Grading of Recommendations Assessment, Development, and Evaluation (GRADE) approach (Supplementary Fig. 4). All analysis was performed using RevMan 5.3 software (the Cochrane Collaboration).
Sensitivity analysis
We conducted a leave-one-out sensitivity analysis to evaluate the influence of individual studies on the pooled estimates. In this procedure, each study was excluded in turn and the meta-analysis was repeated to assess any changes in effect size or heterogeneity. Outcomes that lost or gained statistical significance after exclusion were noted, whereas results that remained unchanged were considered stable.
Results
The PRISMA study selection flowchart is shown in Fig. 1. The systematic search identified 2414 studies, and an additional 14 were added through cross-checking references. A total of 1442 studies were screened for full-text eligibility. Of these, 26 studies met the criteria for full-text review and were included in the qualitative synthesis [14, 26–50]. Among them, only 12 were eligible for statistical analysis and were included in the quantitative synthesis [14, 28, 31, 33, 34, 36, 41, 44, 47–50].Fig. 1. The PRISMA study selection
The characteristics of the 26 studies on pancreatic surgery are summarized in Table 1. Twenty (77%) focused only on pancreatoduodenectomy (PD), 5 (19%) only on distal pancreatectomy (DP), and 1 (4%) on both. Twelve studies (46%) used the updated ISGPS definition of POPF [22], and 14 (54%) referred to CR-POPF according to the previous ISGPF definition [21]. Among the 13,108 patients included, 20% developed POPF. The lowest rate of POPF was reported by Malleo et al. [42] at 13%, while Dai et al. [14] had the highest rate at 57.8%. Seventeen studies evaluated blood loss as an independent risk factor for POPF by multivariate analysis [14, 16, 28, 34, 41–48, 50–54]. Of these, 12 were included in the qualitative synthesis, while 5 additional studies were analyzed separately because they were excluded from the qualitative analysis due to patient duplication and other limitations.
Table 1 Characteristics of the included studiesCharacteristics* N* (%)Year2010–20156 (23)2016–202520 (77)Study TypeRetrospective23 (88)Prospective3 (12)PANCREATIC SURGERY (N = 26)Resection TypePD20 (77)DP5 (19)Both1 (4)POPF definitionISGPF14 (54)ISGPS12 (46)PATIENTS (N = 13108)CR-POPFYes2633 (20)No10,385 (80)
Meta-analysis
Risk of bias assessment
The risk of bias assessment using the ROBINS-I tool is shown in Supplementary Fig. 2. Among the 12 studies included in the meta-analysis, nine were assessed as having a low or moderate risk of bias, while three had a serious risk, mainly due to residual confounding and deviations from intended interventions. Overall, most studies demonstrated a low to moderate risk of bias.
Association between intraoperative blood loss and POPF
The characteristics of the 12 studies that included in the quantitative synthesis are summarized in Table 2. Among the 12 studies included in the meta-analysis [14, 28, 31, 33, 34, 36, 41, 44, 47–50], patients underwent PD or DP. Five studies (42%) used the CR-POPF ISGPF definition and the other Seven (58%) used the ISGPS updated definition. In total, 10,008 patients were analyzed, of whom 1611 developed POPF (overall POPF rate of 16%). The lowest median IBL in POPF patients in the PD group was 380 ml, reported by Dai et al. [49]and lowest median IBL in POPF in all groups including PD and DP was 175 ml, reported by Kawasaki et al. [36]. After statistical analysis, a significant mean difference of 112.46 ml (30.39, 194.53; p = 0.01) between POPF group and no-POPF group was found, with higher intraoperative blood loss associated with POPF development (Fig. 2).Table 2. Characteristics of included studies in the meta–analysisStudyDesignCountryStudy periodPOPF definitionGroupPatientsnumberAge, ySex(Female)Texture (Soft)Duct size, mmPathologyCasciani et al.^*^[47]RetrospectiveInternational2003–2020ISGPSPOPF14.5%(N=1114)N/AN/A85.6% (N=798)≥ 3: 56.8%(N=529)< 3: 43.2%(N=403)(Pancreatic cancer or pancreatitis):32.1% (N=299)no POPF85.5%(N=6592)N/AN/A48.0%(N=2335)≥ 3: 76.6%(N=3723)< 3: 23.4%(N=1140)(Pancreatic cancer or pancreatitis): 43.7%(N=2123)Cai et al. [50]RestrospectiveChina2019–2023ISGPSPOPF19.8%(N=65)61.4 ± 4.5^§^46.2% (N=30)73.9%(N=48)2.0 (1.3–2.6)^†^N/Ano POPF80.2%(N=264)65.7 ± 3.9^§^40.9%(N=108)29.2%(N=77)2.3 (1.5–2.9)^†^N/ADai et al. [49]RetrospectiveChina2014–2023ISGPSPOPF57.8%(N=52)65.8 ± 10.9^‡^11.5%(N=6)64.1%(N=25)3.0 ± 0.1^‡^(Malignant):84.6% (N=44)no POPF42.2%(N=38)63.1 ± 9.9^‡^26.3%(N=10)27.3%(N=6)3.6 ± 0.2^‡^(Malignant):92.1% (N=35)Furukawa et al. [14]RetrospectiveJapan2014–2020ISGPFPOPF30.7%(N=23)71 (62–74)^†^21.7%(N=5)87.0%(N=20)2 (2–4)^†^(Malignant):13.0% (N=3)no POPF69.3%(N=52)68 (63–77)^†^36.5%(N=19)55.8%(N=29)2 (2–2)^†^(Malignant):44.2% (N=3)Hwang et al. [44]RetrospectiveKorea2002–2008ISGPFPOPF17.0%(N=27)62.9 ± 11.2^§^N/AN/A3 (2–3)^†^N/Ano POPF83.0%(N=132)59.6 ± 12.0^§^N/AN/A3 (2–5)^†^N/AKawasaki et al. [36]RetrospectiveKorea2006–2016ISGPFPOPF16.4%(N=10)36 (24–80)70.0%(N=7)70.0%(N=7)N/AN/Ano POPF83.6%(N=51)52 (21–86)66.7%(N=34)81.6%(N=40)N/AN/AKumar et al. [28]RetrospectiveIndia2015–2017ISGPFPOPF20.9%(N=14)48.2 ± 12.1^‡^57.1%(N=8)71.4%(N=10)3.5 ± 2.6^‡^(Malignant):100% (N=14)no POPF79.1%(N=53)48.2 ± 11.3^‡^39.6%(N=21)46.5%(N=20)4.3 ± 2.9^‡^(Malignant):100% (N=53)Li et al. [34]RetrospectiveChina2011–2016ISGPSPOPF20.5%(N=61)62.2 ± 9.4^§^32.8%(N=20)82.0%(N=50)2.6 ± 0.7^§^(Malignant):91.8% (N=56)no POPF79.5%(N=237)61.8 ± 10.1^§^43.0%(N=102)33.8%(N=80)3.2 ± 1.0^§^(Malignant):94.5% (N=224)Marchegiani et al. [48]ProspectiveItaly2016–2021ISGPSPOPF20.1%(N=182)N/AN/AN/AN/AN/Ano POPF79.9%(N=722)N/AN/AN/AN/AN/ASushma et al. [31]ProspectiveIndia2019–2020ISGPSPOPF14.0%(N=7)48 ± 13^§^N/A85.7%(N=6)4 (3.0-4.5)^†^N/Ano POPF86.0%(N=43)54 ± 15^§^N/A32.6%(N=14)4 (3.0-7.0)^†^N/ATomimaru et al. [33]RetrospectiveJapan2009–2017ISGPSPOPF24.1%(N=38)70 ± 7^§^26.3% (N=10)97.4%(N=37)2.8 ± 1.1^§^(Malignant):57.9% (N=22)no POPF75.9%(N=120)70 ± 10^§^45.8% (N=55)43.3%(N=52)4.5 ± 2.0^§^(Malignant):77.5% (N=93)Yang [41]RetrospectiveChina2010–2013ISGPFPOPF16.2%(N=18)56.6 ± 9.8^§^44.4% (N=8)83.3%(N=15)≥ 3: 88.9%(N=16)< 3: 11.1%(N=2)(Malignant):83.3% (N=15)no POPF83.8%(N=93)56.4 ± 10.3^§^51.6% (N=48)75.3%(N=70)≥ 3: 61.3%(N=57)< 3: 38.7%(N=36)(Malignant):87.1% (N=81)*This study, total population (7706) and patient characteristic population (5795) are different. † Median, (IQR) is used. ‡ Median, CI 95% is used. § Mean, SD is used. Duct size refers to the main pancreatic duct (MPD). POPF postoperative pancreatic fistula; ISGPS international study group on pancreatic surgery; ISGPF international study group of pancreatic fistulaFig. 2The forest plot
Subgroup analysis
Subgroup analysis was conducted to separate PD and DP groups in order to evaluate the impact of IBL on POPF within each surgical type. Of the 12 studies, ten were included in the PD subgroup and two in the DP subgroup. Both subgroups demonstrated a statistically significant association between IBL and POPF. The PD subgroup showed a mean difference of 139.19 mL (27.25, 251.14; p = 0.02), and the DP subgroup showed a mean difference of 53.67 mL (19.68, 87.65; p = 0.03). While the PD subgroup continued to show high heterogeneity, the DP subgroup demonstrated markedly lower heterogeneity (I² = 0%).
Sensitivity analysis
A leave-one-out sensitivity analysis was performed to examine the impact of individual studies on the pooled estimates. Sequential removal of each study did not alter the statistical significance of the results, either in the PD subgroup or in the overall analysis. Across the leave-one-out tests, heterogeneity varied between 70 and 91% in the PD subgroup and 33–93% in the overall analysis. Notably, exclusion of Furukawa et al. or Hwang et al. led to a marked decrease in heterogeneity in both the PD subgroup and the overall analysis.
GRADE assessment
Supplementary Fig. 4 summarizes the certainty of evidence for the relationship between IBL and POPF. The overall estimate (12 studies; MD 112.46 mL higher, 95% CI 30.39–194.53) was graded as very low because of limitations in study quality, substantial heterogeneity, and indications of publication bias. The PD subgroup (10 studies; MD 112.46 mL higher, 95% CI 30.39–194.53) likewise showed very low certainty, mainly due to inconsistency and possible publication bias. In contrast, the DP subgroup (2 studies; MD 53.67 mL higher, 95% CI 19.68–87.65) was rated as low certainty, mainly due to the observational study design, but without major concerns regarding risk of bias or inconsistency.
Discussion
As there is already solid evidence that POPF is the major cause of postoperative severe morbidity and mortality after pancreatic surgery [1, 2, 7], the present analysis found that IBL is a key intraoperative risk factor for its development [16, 47]. Higher IBL may contribute to POPF with different pathways. First, high IBL may cause relative ischemia of pancreatic remnant, impairing the healing of the pancreatic anastomosis [15, 16, 18, 55, 56]. Relative ischemia of pancreatic remnant also plays a fundamental role in the etiology of postoperative serum hyperamylasemia (POH) and post-pancreatectomy acute pancreatitis (PPAP) [57, 58], that demonstrated relevant implication on POPF development [59, 60]. Additionally, IBL related transfusions might lead to immunosuppression, tissue edema secondary to aggressive volume replacement, and the inflammatory response triggered by ischemia-reperfusion injury [14–16, 18, 19, 51].
Moreover, maintaining a bloodless surgical field reduces the risk of injuring important structures, particularly biliary ducts, and consequently prevents postoperative biliary complications. Another advantage of keeping low IBL is the ability to visualize all bleeding sites during parenchymal resection and thus perfect hemostasis before closure. Blood is also an excellent culture medium, so minimizing IBL may contribute to a lower rate of infectious complications.
The relevance of IBL in pancreatic surgery was confirmed in 17 different studies which identified it as an independent risk factor for POPF [14, 16, 28, 34, 41–48, 50–54] and IBL is consequently one of the four factors included in the Fistula Risk Score [16]. Callery et al. [16] found that IBL >1000 ml was the most significant factor predisposing patients to POPF [OR: 5.60 (1.65, 18.98), p = 0.006]. Additionally, an increased risk of pancreatic fistula was observed with higher intraoperative blood loss, particularly above the 400 ml [47, 52].
Notably, high blood loss contributes to POPF development both in negligible and high-risk patients. Trudeau et al. [51] found that in patients with negligible endogenous risk (≥ 5 mm duct, protective pathology and firm pancreas), EBL >400 ml was associated with a 5-fold increase in POPF occurrence. Moreover, in high-risk patients (small duct, high risk pathology and soft gland) blood loss is the only modifiable risk factor, so minimizing IBL is even more important, and it should be considered among the strategies to mitigate the risk of POPF development [51, 52]. Consistently with these findings, the meta-analysis confirmed these results. Among 8 studies analyzed, with 8624 patients included and overall POPF rate of 15%, significantly higher IBL was found in patients who developed POPF compared to those who did not.
Multiple risk factors for major intraoperative bleeding during pancreatic surgery have been deeply analyzed and identified in several studies. Preoperatively, male sex, BMI ≥ 25 kg/m^2^, biliary drainage, anticoagulation or antiplatelet treatment, liver function, and neo-adjuvant chemotherapy were found to be associated with high IBL [47, 53, 61]. Intraoperatively, locally advanced disease, vascular and multiorgan resection, and resulting longer operative duration increased the risk of extensive bleeding [53, 62]. Regarding surgical approach, minimally invasive techniques demonstrated to reduce IBL [29, 51, 53]. Finally considering pancreas-specific factors, soft gland texture, non-pancreatic cancer or pancreatitis disease pathology were positively associated with low IBL [47, 53].
To reduce intraoperative bleeding, the anticipatory dissection approach should be applied, with proper exposure of the field and vessels control, as well as accurate hemostasis using all available devices (suture ligation, cautery, staplers) [51, 53, 63]. Some of them have proven to provide a more stable hemostatic seal and a reduction in operative time [64, 65]. Moreover, specifically in pancreatic surgery, the artery first approach might also provide not only better oncologic outcomes but also reduced intraoperative bleeding [66].
It is important to note that in this meta-analysis, we attempted to perform a subgroup analysis of the association between IBL and POPF by considering potential risk factors such as pancreatic duct size and gland texture. However, due to inconsistencies in reporting and the lack of stratification in the included studies, conducting a detailed, separate analysis based on these factors was not achievable.
The present review has several limitations. First, most of the included studies were retrospective and therefore characterized by the inherent risk of heterogeneity. Furthermore, the meta-analysis examining the relationship between IBL and POPF, the funnel plot reveals asymmetry, suggesting potential publication bias with possible overestimation of the association. This highlights the need for more comprehensive reporting of both positive and negative results in future studies of IBL and POPF.
Conclusion
This review confirmed that IBL is an important risk factor for POPF, and it must be considered as a quality indicator in pancreatic surgery. Despite this pronounced clinical relevance in contributing to postoperative outcomes, not all studies in the literature reported median IBLs in complication-group compared with standard postoperative course. In the future, in addition to further efforts to minimize blood loss, it will be necessary to emphasize the need for IBL reporting in all HPB papers, and identify a standardized, universal definition of IBL to allow accurate comparisons across studies and increase the clinical utility of existing risk scores.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary Material 1
Supplementary Material 2