Adrenal causes of endocrine hypertension in childhood or adolescence
Bianca Pellegrini, Ilaria Bonaventura, Valeria Hasenmajer, Chiara Simeoli, Claudia Pivonello, Davide Ferrari, Sabrina Criscuolo, Alessandra Tomaselli, Andrea M. Isidori, Ashley B. Grossman, Andrea Lenzi, Maria Cristina De Martino, Martin O. Savage

TL;DR
This paper reviews adrenal-related causes of high blood pressure in children and adolescents, focusing on genetic disorders and their clinical implications.
Contribution
The paper provides a comprehensive review of adrenal causes of secondary hypertension in pediatric populations, emphasizing genetic factors and diagnostic challenges.
Findings
Adrenal disorders such as Congenital Adrenal Hyperplasia and Familial Hyperaldosteronism are significant causes of secondary hypertension in children.
Genetic mutations in genes like CYP11B1, CYP17A1, and others are linked to endocrine hypertension in pediatric patients.
A systematic diagnostic approach for adrenal-related hypertension in children is currently lacking and requires further development.
Abstract
Arterial hypertension is characterised by elevated blood pressure (BP) leading to cardiovascular morbidity and mortality, and organ damage. Its prevalence in childhood is around 5% and children should be screened from 3 years of age. Hypertension in childhood or adolescence requires exclusion of a secondary cause. Adrenal disorders frequently underlie secondary hypertension. presenting with imbalances of BP and pleiotropic clinical presentations. Examples are rare genetic defects leading to increased mineralocorticoid activity such as Congenital Adrenal Hyperplasia (CAH) due to 11β-hydroxylase gene (CYP11B1) or 17-hydroxylase gene (CYP17A1) mutation, and Familial Hyperaldosteronism (FH), due to 11β-hydroxylase 1 (CYP11B1) and 11β-hydroxylase 2 (CYP11B2) gene fusion, or to mutations of other genes involved in aldosterone production such as those codifying the chloride-voltage gated…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
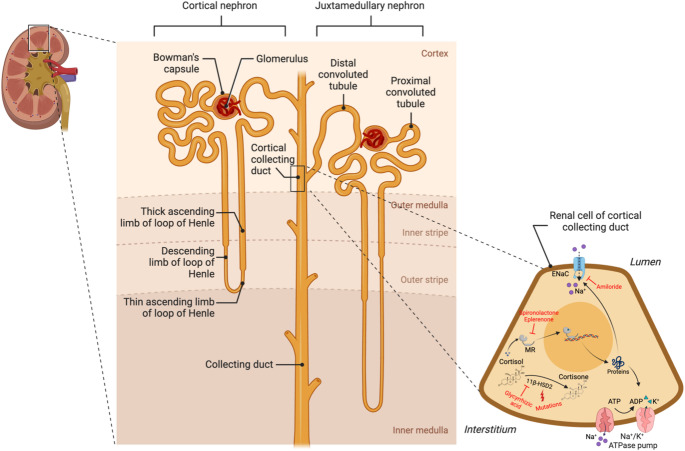 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHormonal Regulation and Hypertension · Adrenal and Paraganglionic Tumors · Adrenal Hormones and Disorders
Introduction
Arterial hypertension is a widespread, chronic condition and represents a primary contributor to the global burden of non-communicable diseases, leading to cardiovascular morbidity and mortality, renal disease, and damage to several other organs and tissues [1]. While standardised BP ranges are commonly employed to define hypertension in adults, BP displays a trend to progressive increase with age and body size during childhood and the transition age, complicating the establishment of singular cut-offs for diagnosis of hypertension in this age range. According to the European Society of Hypertension, hypertension is diagnosed in children and adolescents aged 3–15 years when BP levels exceed the 95th percentile of the normative BP distribution for age, sex and height percentiles across at least three different measurements [2–4]. From 16 years of age, diagnostic criteria align with those for adults, with a cutoff of 140 mmHg for systolic BP and 90 mmHg for diastolic BP [3]. Consequently, the expected prevalence of hypertension in childhood is approximately 5%.
However, these diagnostic criteria are inconsistently applied across different countries and the normative data are somewhat outdated, making it challenging to accurately determine the prevalence of hypertension in childhood. In the American continent, the estimates range from 0.3 to 4.5% [5], but the prevalence vertiginously increases in the presence of concomitant overweight or obesity [6]. European studies report a prevalence ranging from 2 to 13% in children and adolescents [7, 8]. An Italian study evaluated 415 Italian children and adolescents referred for obesity, and found that 23.6% showed elevated BP levels [9]. The development of hypertension in childhood and adolescence is linked to an increased risk of adult age hypertension [10]. Therefore, it is recommended that BP be screened in children starting from 3 years of age for early exclusion of hypertension [2].
When hypertension is identified in children and during the transition to adulthood, the search for a secondary cause should always be made. The spectrum of potential causes of hypertension at these ages is broad, encompassing conditions such as coarctation of the aorta, renal parenchymal diseases and nephron-vascular hypertension, and other more rare causes including monogenic disorders, systemic arteritis and neurological diseases [2].
Endocrine disorders frequently underlie secondary hypertension. Indeed, the mechanism regulating BP levels are intricately intertwined with the endocrine system at various levels [11]. Notably, the adrenal glands play a pivotal role in BP regulation. Adrenocortical steroids, especially glucocorticoids and mineralocorticoids, act as BP regulators through receptor-mediated signalling pathways in the kidneys, cardiovascular system and several other organs and tissues [12, 13]. Similarly, catecholamines from the adrenal medulla target adrenergic and dopamine receptors, influencing BP both peripherally and centrally by acting on arterial smooth muscle and myocardial tissue [14]. Given the adrenal glands’ central role in BP regulation, it is not surprising that most of the adrenal disorders present with an imbalance in BP.
In this review, our investigation will focus on the characteristics encountered in diagnosing hypertension of adrenal origin during childhood and the transition to adulthood, considering variations in prevalence, clinical presentation, genetic predisposition, and therapeutic strategies.
Rare forms of congenital adrenal hyperplasia causing
Adrenal steroidogenesis relies on enzymatic reactions leading to the synthesis of the three main groups of adrenal hormones: glucocorticoids, mineralocorticoids and androgens. Enzymatic defects throughout the pathway characterise different forms of congenital adrenal hyperplasia (CAH). They can lead to an absolute or relative deficiency of one or more hormones, and the lack of negative feedback control of pituitary adrenocorticotropic hormone (ACTH) secretion results in increased precursors that impact the clinical presentation. Hypertension due to accumulating mineralocorticoid precursors is characteristic of 11β-hydroxylase (CYP11B1) and 17-hydroxylase (CYP17A1) deficiency [15].
11β-Hydroxylase deficiency
Diagnosis
The identification of 11β-hydroxylase deficiency as a cause of congenital hypertensive hyperandrogenism was first proposed in the 1950 s [16], and accounts for approximately 5% of CAH cases [15]; 11β-hydroxylase is encoded by CYP11B1 on chromosome 8q21 and more than 100 mutations have been described, including chimeric CYP11B1/CYP11B2 forms [17] and uniparental disomy [18], but there appears to be little correlation between genotype and phenotype [19].
Defective 11β-hydroxylase activity due to mutations in the CYP11B1 gene affects the final step of cortisol secretion, leading to accumulation of 11-deoxycortisol and other precursors in the zona fasciculata, while in the zona glomerulosa, the conversion from 11-deoxycorticosterone (DOC) to corticosterone, an aldosterone precursor, is impaired. The accumulating precursors cause clinical and biochemical hyperandrogenism and the increased DOC levels lead to hyporeninaemic hypertension. Cortisol deficiency impairs the physiological pituitary and hypothalamic feedback control, resulting in excess unregulated ACTH secretion [20].
Clinical presentation
The classical form of the condition are characterised by variable degrees of hypokalaemic hypertension and hyperandrogenism, resulting in virilisation in 46XX patients and increased androgenisation in 46XY patients, together with accelerated linear growth and peripheral premature puberty. Approximately two thirds of patients develop hypertension, often during childhood [21], or even at birth in one case report [22]. In a case series, a correlation between age of diagnosis and severity of hypertension is reported [23]. Hypertension is usually of mild-to-moderate severity, despite a few cases of malignant hypertension [24, 25]even requiring salvage adrenalectomy [24]. Accordingly, left ventricular hypertrophy, retinopathy, hypertensive nephropathy, ischaemic heart disease, cerebrovascular accidents, and deaths are reported [24–27] The age of diagnosis is very variable and often sex-related, since genital ambiguity in females is detected at birth and leads to earlier evaluations compared to males. In the largest studied cohort from a multicentre study, age at diagnosis ranged between birth and 17 years [28]. In untreated males, testicular adrenal rest tumours (TART) may develop [29–32].
Non-classical forms of CAH due to 11β-hydroxylase deficiency have also been described [33]^,^ mimicking polycystic ovary syndrome and representing a potentially understudied phenotype of this rare condition.
Treatment
Management includes appropriate glucocorticoid replacement as required, along with additional anti-hypertensive therapy if needed [34]. Preferred therapies are Mineralocorticoid Receptor (MR) Antagonists (MRAs), such as spironolactone and eplerenone, and epithelial sodium channel (ENaC) blockers such as amiloride [2]. For the treatment of androgen excess, glucocorticoid replacement is usually able to at least partially normalise levels of androgen precursors; however, other therapeutic strategies, such as anti-androgen therapies, might be required in severe virilisation. Synthetic long-acting steroids are not routinely recommended to achieve ACTH suppression. Adrenalectomy, on the other hand, remains an option in uncontrolled cases.
17-Hydroxylase/17,20-lyase deficiency
Diagnosis
The first case of 17-hydroxylase deficiency was reported in 1966 [35], describing a 46XX woman, aged 35 years old, with hypertension, prepubertal breast tissue and lack of axillary and pubic hair: 17-hydroxylase/17,20-lyase deficiency is rare, accounting for approximately 1% of CAH. Moreover, complete 17-hydroxylase/17,20-lyase deficiency and the much rarer isolated 17,20-lyase deficiency have been described as separate conditions [36]. Overall, 17-hydroxylase/17,20-lyase deficiency is more common in certain regions such as Brazil [37, 38] Japan [39] and China [40]^,^ and more than 90 mutations have been identified.
The human CYP17A1 gene is located on chromosome 10q24.3 and is transcribed both in the adrenals and gonads. It catalyses both 17-hydroxylase and 17,20-lyase activities, allowing transformation of pregnenolone and progesterone into 17-OH-pregnenolone and 17-OH-progesterone, respectively, while 17,20-lyase is needed to produce C19 sex steroids [41]. Due to the description of a few cases of isolated 17,20-lyase deficiency with preserved 17-hydroxylase function, the two activities were assumed to be related to two different enzymes, but further studies have identified P45017a as a single polypeptide catalysing both reactions [42]. Isolated 17,20-lyase has been attributed to mutations in the binding regions of P45017α with cytochrome P450 oxidoreductase and microsomal cytochrome b5. These cofactors are considered “redox partners” for P45017α, and are needed to catalyse the 17,20-lyase reaction. Mutations of the POR gene encoding for cytochrome P450 oxidoreductase, affecting its binding to P45017α, have been described, and are phenocopies of CYP17A1 mutations causing isolated 17,20-lyase deficiency [43, 44].
Thus, defective CYP17A1 activity leads to increased mineralocorticoid precursors, while the cortisol and sex steroid pathways are blocked, the latter in the gonads as well. The overproduction of DOC leads to hypokalaemic hypertension in this condition. Due to the increased levels of corticosterone, glucocorticoid activity is usually preserved, but with altered ACTH feedback.
Clinical presentation
Diagnosis is often delayed due to the lack of adrenal insufficiency and an elusive clinical picture during childhood. In fact, the profound androgen and oestrogen deficiency due to altered 17,20-lyase activity leads to abnormal sexual differentiation with external female genitalia in 46XY individuals and a lack of breast development and primary amenorrhoea in 46XX individuals, even though the phenotypic spectrum is rather broad, as described by several case series [45]. Accordingly, most patients are diagnosed during adolescence [46].
In 46XX patients, ovarian cysts, amenorrhoea and infertility are common, due to persistently high progesterone levels, increased FSH and LH and low oestrogen [47]. Ovulation induction and successful pregnancies through medically-assisted reproduction techniques have been described in patients with complete and incomplete 17-hydroxylase/17,20-lyase deficiency [47, 48]. On the other hand, reports on fertility preservation in 46XY males with this condition have not been published. Hypertension in 17-hydroxylase/17,20-lyase deficiency, similarly to 11β-hydroxylase deficiency, is due to salt retention and volume expansion caused by excess mineralocorticoid precursors, and is usually mild. Due to the delay in diagnosis, hypertension is most commonly described during adolescence [49]. Severe hypertension can be an unusual presenting symptom, leading to earlier diagnosis, as described in a case series of 12 patients [46]. Malignant hypertension, even leading to encephalopathy and death, has also been described [46, 50].
Treatment
Glucocorticoid replacement is usually not required due to high corticosterone production and might lead to hypothalamo-pituitary-adrenal (HPA) axis suppression with increased risk for adrenal crises. MRAs are usually successful in achieving target BP levels [51] and, due to lack of virilisation, side effects in the 46XY population such as gynaecomastia and erectile dysfunction are usually absent. Hormonal replacement therapy is usually required in 46XX patients, along with testosterone therapy for 46XY patients, reared or reassigned as males by patient and family preference.
Familial hyperaldosteronism (FH)
Primary Aldosteronism (PA) is the most common cause of secondary hypertension in the paediatric and transitional age. In approximately 5% of cases, it is hereditary and is referred to as familial hyperaldosteronism (FH) [52]. Within the definition of FH, some disorders present with heterogeneous clinical features and age at diagnosis ranging from the first months of life to the transitional age, indeed the current guidelines establish < 20 years as the cut-off age for clinical suspicion of FH [53]. In addition to type 1 FH or glucocorticoid-remediable aldosteronism, three other forms of FH are currently known.
FH1 is caused by a chimeric 11β-hydroxylase 1 (CYP11B1)−11β-hydroxylase 2 (CYP11B2) gene, which leads to ACTH-stimulated synthesis of aldosterone. The other types of FH are due to altered function of anion or cation channels which are involved in the regulation of aldosterone production. In-depth study of the molecular alterations underlying FH, their pathophysiological implications, and the clinical characterisation of affected families, has allowed precise predictions of genotype-phenotype correlations, although much remains to be understood about the pathogenesis and clinical manifestations of FH [54].
FH1
Pathogenesis and diagnosis
FH1, the first monogenic form of FH identified, is also known as glucocorticoid-remediable aldosteronism [55] and accounts for 1% of PA cases and 3.1% of cases of hypertension onset between ages 4 and 15 [55, 56]. Inherited as an autosomal dominant disorder, it is caused by an unequal crossover between the CYP11B1 and CYP11B2 genes, which are 95% homologous, on chromosome 8 (locus 8q24). The resulting chimeric gene contains the promoter of CYP11B1 and the coding portion of CYP11B2. In the zona fasciculata of the adrenal cortex, this results in abnormal activity of 11β-hydroxylase-aldosterone synthase under non-physiological ACTH stimulation [57, 58]. Although a wild-type copy of the aldosterone synthase gene is present, aldosterone production is not responsive to angiotensin stimulation so the hybrid gene’s function predominates over the persistently deficient wild-type gene [59, 60]. Furthermore, ACTH stimulation activates cortisol C-18-hydroxylation and C-18-oxidation by aldosterone synthase, resulting in the over-secretion of 18OH-cortisol and 18-oxo-cortisol [61].
Clinical presentation
The clinical presentation of FH1 is highly variable, being generally characterised by arterial hypertension before the age of 20 (mean age 18 ± 17.6 years) [62] and rarely accompanied in early childhood by cerebellar infarction or intracranial haemorrhage [55, 62].A recent systematic review revealed that among individuals with a confirmed genetic diagnosis of FH1, about 77% were hypertensive and about 42% were hypokalaemic [62].
Hypertension in FH1 is often resistant to polypharmacotherapy and accompanied by early micro/macrovascular complications, such as vascular dissections (sometimes as early as age 10), retinopathy (mean age 16.5 years), nephropathy, cardiac remodelling with left ventricular hypertrophy (mean age 15 years), and increased risk of acute myocardial infarction and stroke at a young age (before age 40 years) [62, 63]. Males tend to present with a more severe phenotype and worse long-term cardiovascular prognosis compared to females [64].
A good clinical response to glucocorticoid administration strongly suggests the diagnosis of FH1. To confirm the diagnosis, dexamethasone suppression tests for aldosterone and measurements of hybrid steroids, particularly 18-oxo-cortisol, have been suggested. The levels of 18-oxo-cortisol seem to correlate with the “mean day curve control” achieved with medical therapy [60, 65]. However, studies on large populations of FH1 patients have shown that the aldosterone-renin ratio (ARR) remains probably the more reliable biochemical marker of the disease, with no significant differences in biochemical parameters between subjects with mild and severe phenotypes. Definitive diagnostic confirmation requires molecular analysis to detect the chimeric gene [64].
However, different possible locations of the crossover breakpoints have been described and probably result in considerable genotypic variability. Indeed, some studies have shown that the hybrid gene, considered pathognomonic, can be detected only in a minority of FH1 patients, and that the use of plasmids containing a large fragment of the wild-type CYP11B2 gene and the chimeric gene - including segments where the most frequent breakpoints occur - could represent more sensitive tools for the molecular diagnosis of FH1 [66, 67]. The adrenal morphological findings on imaging are variable and include normal adrenal glands, bilateral adrenal hyperplasia, and adrenal adenomas [56].
Treatment
Current guidelines recommend a low-dose, long-acting glucocorticoid taken before bedtime to suppress ACTH, with the addition of MRAs such as spironolactone if no satisfactory clinical response is achieved. The goal of medical therapy is to adequately balance the benefit of controlling BP and electrolytes with the risk of excessive corticosteroid exposure and, in the case of some MRAs, undesirable effects such as gynaecomastia in males. Overall, safer partial suppression of ACTH might be sufficient for disease control [62].
FH2
Pathogenesis and diagnosis
Initially, all non-FH1 cases of FH were described as FH2 [58]. This broad definition included a large number of heterogeneous cases from chemical, biochemical, and radiological perspectives, sometimes indistinguishable from sporadic PA [68]. At the same time, it entailed a significant risk of overestimating the prevalence of FH2. Indeed, considering the high prevalence of PA in the general population there is a non-negligible probability that at least two cases of sporadic PA could coexist in the same family [56, 69]. In recent decades, gene sequencing has enabled the identification of genes whose mutations are responsible for different types of FH. Currently, experts suggest that the definition of FH2 should refer only to forms due to germline mutations of CLCN2, codifying the chloride-voltage gated channel 2 (ClC2). FH2 represents around 5% of PA cases.
CLCN2 is a highly conserved gene among different species, located on the long arm of chromosome 3 (locus 3q27.1) [56]. ClC2 is expressed in various human organs and tissues, including the brain, intestine, lung, and adrenal cortex [56]. Immunohistochemical studies have demonstrated a predominant localization of ClC2 in the zona glomerulosa of the adrenal cortex [70]. Moreover, somatic mutations of CLCN2 have been observed in aldosterone-producing adenomas in association with more severe biochemical hyperaldosteronism, thus suggesting the important role of ClC2 in determining aldosterone synthesis [54, 71, 72].
The ClC2 channel is a homodimer, each subunit containing a conduction pore. Gate opening can occur with a rapid activation of individual subunits or with a slow combined activation of the two subunits. ClC2 undergoes slow activation at potentials more negative than the chloride equilibrium potential. At the resting potential of zona glomerulosa cells, ClC2 is slowly activated. The increased sodium efflux leads to a faster cell depolarisation, followed by the activation of voltage-dependent calcium channels, which results in the overexpression of genes involved in aldosterone synthesis, including CYP11B2 [70, 73].
Currently, six mutated variants of ClC2 have been identified in patients with FH2:
- pSer865Arg: at the C-terminal end; modifies channel gating, especially with increased fast gate opening.
- pArg175Gln: at the cytosolic end of the D-helix; through interaction with the C-terminal end, alters anionic selectivity and gating.
- pLys263del: in-frame deletion at the loop between helices J and K; facilitates gate opening.
- pGly24Asp,* pMet22Lys*,* pTyr26Asn*: at the N-terminal end in the inactivation domain; causes greater current flows at the resting potential [74].
Biochemical investigations show elevated aldosterone, suppressed renin, and hypokalaemia. Given the absence of pathognomonic clinical features or specific biochemical markers of FH2, definitive diagnostic confirmation requires molecular investigations identifying germline mutations of CLCN2 [69].
Clinical presentation
The clinical presentation of FH2 is variable and may include hypertension with onset at a young age, often before 20 years, and sometimes hypokalaemia [75]. As in FH1, autosomal dominant inheritance with incomplete penetrance has been hypothesised, as many individuals are heterozygous and some cases of patients with a normal aldosterone/renin ratio or spontaneous improvement of hypertension with increasing age have been observed [56]. Adrenal morphology is variable (normal glands, adenomas, bilateral hyperplasia).
Treatment
Generally, a good clinical response, with improvement of hypertension and hypokalaemia when present. is achieved with medical therapy using MRAs as spironolactone or amiloride [56, 69].
FH3
Pathogenesis and diagnosis
FH3 is defined as FH due to germline mutations of potassium inwardly rectifying channel subfamily J member 5 gene (KCNJ5), which is estimated to account for 8% of FH cases and 0.6% of PA cases [56]. The KCNJ5 gene is located on the long arm of chromosome 11 (Locus 11q24.3) and encodes the potassium channel KIR3.4 [76]. Therefore, FH3 can be considered a veritable channelopathy [77].
In humans, KIR3.4 is expressed in various organs and tissues, including the heart, central and peripheral nervous system, and adrenal cortex [78]. Immunohistochemical studies on the adrenal cortex have demonstrated predominant localisation of KIR3.4 in the zona glomerulosa [79]. Next-generation sequencing analyses have identified somatic mutations of KCNJ5 in about 40% of aldosterone-producing adrenocortical adenomas, associated with more severe hyperaldosteronism, suggesting a direct role of KCNJ5 in determining aldosterone overproduction and proliferation of the zona glomerulosa cells [58, 80].
KIR3.4 can assemble in homotetramers or heterotetramers with KIR3.1 [81]. At the resting potential of the zona glomerulosa cells of the adrenal cortex, KIR3.4 helps to maintain membrane hyperpolarisation, thanks to high conductance potassium efflux [76]. Mutations in KCNJ5 responsible for FH3 cause reduced channel selectivity, resulting in increased sodium influx and membrane depolarisation, followed by the activation of voltage-dependent calcium channels, increased intracellular calcium, and the upregulation of genes that contribute to aldosterone synthesis [82].
Currently, 9 mutated variants of KIR3.4 have been identified in patients with FH3:
- Thr158Ala,* Gly151Arg*,* Ile157Ser*,* Gly151Glu*,* Glu145Gln*,* Tyr152Cys*,* pThr149Del*, with substitutions or deletions of amino acids in or near the selectivity filter.
- Val259Met and Tyr348Asn near the C-terminal cytoplasmic end [78, 79, 83, 84].
Clinical presentation
Considerable clinical heterogeneity has been documented among families affected by FH3. A classification of FH3 into two subtypes has been proposed: the more severe type A and the milder type B [85]. Furthermore, specific genotypes underlying the milder/more severe phenotypes have also been suggested. Indeed, some KCNJ5 mutations cause more marked alterations in KIR3.4 permeability to sodium and may be potentially lethal for zona glomerulosa cells [58]. The latter mutations are associated with clinical presentations characterised by less severe hyperaldosteronism and the absence of marked adrenal hyperplasia [82].
A more severe clinical presentation with young age-onset hypertension resistant to pharmacological treatment, hypokalaemia, polyuria, nocturia, polydipsia, myalgia, and in one case, growth retardation, has been described in patients with mutated variant Thr158Ala,* Gly151Arg*,* Glu145Gln* or Ile157Ser [78, 86–88]. In these cases the imaging of the abdomen shows massive bilateral adrenal hyperplasia, often with a macronodular aspect. Histological examination reveals a loss of zonation and difficulty distinguishing zona glomerulosa cells, confirmed by co-expression of CYP17,* CYP11B1*, and CYP11B2 in some cells on immunohistochemistry [89].
Milder clinical presentations have been observed in patients with the variants of Gly151Glu and Tyr152Cys, presenting with severe hypertension at a young age and hypokalaemia showing favourable disease progression during growth, and later-onset hypertension in some cases. Radiological findings do not show significant adrenal hyperplasia, except in one case of germline mosaicism of KCNJ with bilateral adrenal hyperplasia [90]. Good clinical and biochemical control is achieved with pharmacological therapy: MRAs such as spironolactone or canrenone and other anti-hypertensives such as ACE inhibitors or β-blockers. verapamil or amiloride [78, 91].
Patients with Val259Met and Tyr348Asn variants present with hypertension after age 50, normal aldosterone-renin ratio values, but ACTH-stimulated aldosterone hypersecretion, in the presence of normal adrenal glands on abdominal imaging [92]. The only one patient with pThr149Del variant developed hypertension at age 11 complicated by organ damage, alkalosis, and hypokalaemia, which was well controlled with medical therapy. Adrenal MRI showed unilateral pseudo-nodular thickening [76].
Treatment
Medical treatment with MRAs is generally described as the first treatment in children or adolescents affected by FH3, eventually in combination with β-blockers, ACE-inhibitors or other anti-hypertensive drugs if BP is not adequately controlled [78]. In most severe cases, when hypertension and hypokalaemia are resistant to medical treatment, adrenalectomy may be required to achieve clinical control [69].
FH4
Pathogenesis and diagnosis
FH4 is defined as FH due to germline mutations of the calcium voltage-gated channel subunits α 1 H gene (CACNA1H) and is inherited as an autosomal dominant disorder [93, 94].
The CACNA1H gene is located on the short arm of chromosome 16 (Locus 16p13) and encodes the α subunit of the T-type voltage-dependent calcium channel Cav3.2 [56]. CACNA1H is widely expressed in the zona glomerulosa of the adrenal cortex, where it is involved in the regulation of CYP11B2 expression and aldosterone production in response to membrane potential fluctuations, including the nervous system. Indeed, independently of hyperaldosteronism, CACNA1H variants have already been associated with absence epilepsy and idiopathic generalised epilepsy [58].
In vitro studies have demonstrated that gain-of-function variants of CACNA1H, when stimulated by potassium, lead to over-expression of CYP11B2. The prevalence of somatic CACNA1H mutations in aldosterone-producing adrenocortical adenomas is 4%, and it is unclear whether these mutations play a role in cell proliferation in aldosterone-producing adrenocortical adenomas besides determining the hormonal hypersecretion [58, 95, 96].
Currently, five variants of Cav3.2 due to mutations in highly conserved regions of CACNA1H and responsible for FH4 are known:
- Met1549Val: in a portion of the transmembrane segment S6 of repeat domain 3, leading to channel activation with calcium influx at less negative potentials and slow inactivation [97].
- Ser196Leu: in the voltage sensor region, in the transmembrane segment S4 of repeat domain 1.
- Pro2083Leu: in the C-terminal cytoplasmic domain.
- Val1951Glu and Met1549Ile: in the C-terminal cytoplasmic domain, likely involved in the channel activation [98].
Despite autosomal dominant inheritance, cases of subjects carrying CACNA1H mutations with no hypertension even in adult age, or without biochemical evidence of hyperaldosteronism, have been described. Incomplete penetrance due to genetic mosaicisms or a tendency for the clinical picture to ameliorate with increasing age could be suggested [58].
Clinical presentation
The clinical presentation typically associated with the Met1549Val mutation includes the onset of hypertension before the age of 10 years, without a history of epilepsy or neuropsychiatric disorders, while patients with the Met1549Ile variant have shown mental retardation and learning disorders [97, 98]. In one patient with the Met1549Val mutation, growth retardation has been described [99].
Interestingly, a de novo missense germline mutation in the transmembrane voltage sensor domain was described in a 31-year-old patient with PA and no family history of hypertension or hypokalaemia. This mutation caused a loss of function of Cav3.2 and reduced whole-cell current, indicating that the pathogenic role of CACNA1H is still not fully understood [99].
Radiological findings show normal adrenal glands in the majority of cases, particularly in association with the Met1549Val and Met1549Ile variants. Gland thickening without nodules, single or bilateral adrenal nodules, are associated with the variants Pro2083Leu,* Val1951Glu*, and Ser196Leu, respectively [94].
Treatment
The goal of FH4 therapy is clinical control of hyperaldosteronism, generally achieved with MRAs and, if necessary in the presence of aldosterone-producing adrenocortical adenomas, adrenalectomy.
CACNA1D-related hyperaldosteronism
Pathogenesis and diagnosis
In addition to the monogenic forms of PA described above, germline mutations of the calcium voltage-gated channel subunits α 1 D gene (CACNA1D) can cause PA in early childhood. The CACNA1D gene, located on the short arm of chromosome 3 (Locus 3p14.3), encodes the pore-forming α1 subunit of the L-Type voltage-dependent calcium channel Cav1.3 [58, 100]. In humans, Cav1.3 is expressed in the zona glomerulosa of the adrenal cortex, in the brain, in pancreatic β cells, in the sinoatrial node, and in cochlear hair cells [101–103].
Clinical presentation
Homozygous mutations in CACNA1D lead to severe cardiac conduction disorders and congenital deafness, while heterozygous mutations can lead to various clinical presentations, including neuropsychiatric disorders, neonatal hyperinsulinaemic hypoglycaemia, and PA [102, 103].
Somatic mutations of CACNA1D are among the most frequent mutations in aldosterone-producing adrenocortical adenomas, particularly in the absence of KCNJ5 mutations, where the gain of function of Cav1.3 is responsible for aldosterone production [104, 105]. Germline mutations of CACNA1D, some of which are identical to somatic mutations in aldosterone-producing adrenocortical adenomas, cause PA with epilepsy and neurological abnormalities in early infancy (the so-called primary hyperaldosteronism-seizures-neurological abnormalities syndrome) [106].
Currently, 4 mutated variants of Cav1.3 responsible for childhood PA are known:
- Gly403Asp.
- Ile770Met.
- Phe767Leu.
- Thr776Ala.
These mutations involve domains responsible for channel opening, in highly conserved regions of Cav1.3, and channel activation at less depolarised potentials and interfere with channel inactivation [106].
The clinical presentation includes neurological disorders (epilepsy, cerebral palsy, cerebral blindness etc.), cardiac abnormalities (ventricular hypertrophy, atrial septal defects), and PA with arterial hypertension and hypokalaemia. Hypertension onset has been described at 1–3 months of life associated with the Gly403Asp and Thr776Ala variants, and at age 5 associated with the Ile770Met variant [104, 107].Recently, a case of de novo mosaicism of the Phe767Leu variant was described in a patient with Chiari malformation, chorea, developmental delay, neonatal hypoglycaemia, and low renin levels [102].
Treatment
As demonstrated by preclinical studies and clinical experience, given the central pathogenic role of altered calcium signalling in PASNA syndrome, good control of both PA and neurological symptoms can be achieved with dihydropyridine calcium antagonists [104, 108].
Paediatric cushing’s syndrome
Pathogenesis
Cushing’s syndrome (CS) is caused by prolonged exposure to elevated circulating levels of cortisol [109–112]. The majority of cases, 70–80%, of endogenous CS are due to hypersecretion of ACTH by the pituitary gland at all ages [109–114]. This excessive ACTH production stimulates the adrenal glands to overproduce cortisol, a condition known as pituitary-dependent CS or Cushing’s disease (CD). On the other hand, ACTH-independent adrenal production of cortisol by an adrenocortical adenoma, carcinoma or rare forms of bilateral adrenal disease, accounts for the remaining percentage of cases of endogenous CS [109–112].
However, in children aged less than 5 years, CD is extremely rare and the most common cause of CS in this age group is ACTH-independent CS (due to adrenocortical adenoma, carcinoma or bilateral adrenal hyperplasia) [113, 114]. Lastly, although extremely rare in the paediatric age range, an extra-pituitary tumour that secretes ACTH or, even more rarely, corticotropin-releasing hormone (CRH), causes ectopic CS [115]. Endogenous CS is rare in children and adolescents, compared to its frequency in adults. The annual incidence in the general population is estimated to be between 0.7 and 2.4 cases per million individuals, and only 10% of new cases occur in children each year [113, 114]. In prepubertal paediatric patients, CD is commoner in boys than in girls, with the sex incidence equalising during puberty and then assuming the adult female dominant pattern after puberty [113, 114, 116].
Albeit rare, several genetic mutations are responsible for syndromes associated with paediatric CS [117, 118]. McCune-Albright syndrome results from somatic mutations of the GNAS gene, specifically mutations in the cAMP-regulating protein, Gsα, that is constitutively activated [117, 119]. McCune-Albright syndrome is characterised by the clinical triad of fibrous dysplasia, café-au-lait skin pigmentation, and precocious puberty, and may include other endocrine abnormalities, such as CS, excess growth hormone secretion, and hyperthyroidism [119]. In McCune-Albright syndrome, the adrenal glands develop a unique form of adrenal hyperplasia, termed primary bimorphic adrenocortical disease, characterised by multiple nodules arising from adrenocortical cells with fetal characteristics [120].
Primary pigmented nodular adrenocortical disease (PPNAD) is a genetic disorder usually associated with Carney complex, a syndrome of multiple endocrine gland abnormalities caused by inactivating germline mutations of the PRKAR1A gene, leading to constitutive activation of the cAMP–PKA pathway by increasing the availability of the PKA catalytic subunits [121]. The adrenal glands in PPNAD are characterised by multiple pigmented nodules that autonomously secrete cortisol and are surrounded by an atrophic cortex [121]. Primary bilateral macronodular adrenal hyperplasia (PBMAH) is frequently a genetic disorder, most often caused by inactivating mutations of ARMC5, a putative tumour suppressor gene [117, 122]. Histologically, PBMAH is composed of numerous nodules measuring > 1 cm each and in more than 90% of cases PBMAH is characterised by varying degree of hypercortisolism [122–124].
Multiple endocrine neoplasia type 1 (MEN 1) is an autosomal dominant disorder due to mutations in the MEN1 gene, which codes for the protein menin. It is characterised by neuroendocrine tumours, mainly affecting the parathyroid glands, pancreatic islet cells and anterior pituitary. Although rare, CD can occasionally be associated with MEN 1 [125].
The most prevalent somatic mutations in paediatric CD occur in the USP8 gene, which have been detected in 31–63% of corticotroph adenomas. The USP8 gene encodes a deubiquitinase enzyme responsible for regulating tyrosine kinase receptors, such as the epidermal growth factor receptor (EGFR) [118]. Deubiquitination of EGFR prevents its degradation in lysosomes, thereby maintaining downstream signalling pathways [126, 127]. While biochemical markers of hypercortisolism, tumour size, and the frequency of cavernous sinus invasion, show no significant differences between subjects with and without USP8 mutations, individuals with these mutations have a higher risk of CD recurrence following transsphenoidal surgery (TSS) compared to those without mutations [126].
Childhood adrenocortical carcinomas (ACC) may be associated with Li-Fraumeni and Lynch syndromes [128]. Genetic diagnosis of Li-Fraumeni syndrome is usually made by germline analysis for variants in TP53 [129]. Evaluation for Lynch syndrome can be initiated by immunohistochemistry for MSH2, MLH1, PMS2, MSH6 and microsatellite instability testing, or by direct germline genetic analysis for MSH2,* MLH1*,* PMS2*,* MSH6 and EPCAM* [130]. All children diagnosed with ACC should undergo a systematic search for germline TP53 pathogenic variants, as 50–90% of childhood ACC is associated with such variants [128].
Hypertension is common at diagnosis (36–71%) and its severity is mainly related to the duration and intensity of elevated cortisol levels, due to the induction of the mineralocorticoid response mediated by cortisol excess [3, 131–136]. Specifically, the MR is activated by the saturation of the enzyme 11β-hydroxysteroid dehydrogenase type 2 (11β-HSD2), which converts cortisol to inactive cortisone, thus protecting it from cortisol binding [135, 136]^127^. As a result, cortisol binds to the MR, mimicking the action of aldosterone, leading to renal sodium uptake and potassium excretion, resulting in blood volume expansion and hypertension [136–138]. Moreover, glucocorticoids modulate the synthesis and the vascular response to catecholamines, resulting in an enhanced pressor response to β-adrenergic agonists and impaired cardiac sympathetic autonomic modulation [136].
In addition, hypercortisolism enhances the vascular response to vasoconstrictors, leading to increased BP levels [136]^126^. Additionally, cortisol exerts an indirect effect on BP and the vasculature through the systemic complications of CS, such as the metabolic syndrome, and obstructive sleep apnoea [132, 139]. Typically, the loss of physiological nocturnal BP decreases to the extent that non-dipping hypertension is one of the main cardiovascular manifestations in patients with CS, reflecting the impairment of circadian cortisol secretion [132, 139]. Given the high prevalence of hypertension in these patients, an early diagnosis of CS is advisable in order to reduce the cardiovascular complications to which these patients are predisposed [3, 131].
Diagnosis
In paediatric patients with suspected CS, exclusion of exposure to exogenous glucocorticoids prior to biochemical evaluation is mandatory. After an initial evaluation that includes assessment of auxological parameters, pubertal stage, virilisation and bone age, documentation of hypercortisolism is crucial, usually using 24-hour urinary free cortisol (UFC), late night salivary cortisol (LNSC) or sleeping midnight serum cortisol determination, and dexamethasone suppression testing (DST). Due to imperfect diagnostic accuracy and limitations, multiple tests are often required to confirm hypercortisolism [140, 141]. Once hypercortisolism has been diagnosed, it is important to differentiate ACTH-dependent from ACTH-independent CS using hormonal assays and imaging. CD typically shows detectable morning plasma ACTH, whereas primary adrenal disease shows suppressed levels (ACTH < 5 pg/mL) [141]. In the latter case, imaging of the adrenal glands is indicated. The CRH stimulation test may show an exaggerated cortisol response in pituitary adenomas, suggesting a diagnosis of CD [142], although due to a lack of availability desmopressin may be used instead. Pituitary Magnetic Resonance Imaging (MRI) assists in this diagnosis but has limited accuracy, revealing an abnormal pituitary image in approximately 60% of cases of CD. Bilateral inferior petrosal sinus sampling (BIPSS) is recommended along with CRH or desmopressin stimulation in paediatric cases with a negative MRI and confirmed hypercortisolism to rule out ectopic [143].
Clinical presentation
Key diagnostic features in children with CS, are facial rounding, weight gain, growth retardation and increased virilisation [113, 114]. Facial changes occur gradually and are often initially unnoticed, while weight gain is more rapidly noticed by relatives [144]. Growth retardation does not always lead to short stature, but growth velocity is reduced [145]. Virilisation manifests as advanced Tanner stage pubic hair growth compared with breast development or testicular volume, although this can be difficult to detect in pubertal patients [144].
Other less specific symptoms include osteopenia, hirsutism, mood changes, striae, hypertension, acne, and delayed puberty [113, 114]. Despite short stature, bone age typically remains within the normal range due to increased adrenal androgen secretion [146]. Long-term hypercortisolism may lead to gonadotrophin deficiency, evidenced by decreased testicular volume or breast development along with advanced pubic hair growth [146].
Treatment
The primary treatment for CD in children is transsphenoidal surgical resection (TSS) of the pituitary tumour, with success rates of 70 − 100% in experienced centres [142]. However, surgery can fail, or CD can recur, with lower success rates for repeat TSS [147]. Complications after surgery include various hormonal imbalances and rare cases of mortality [148]. Hypopituitarism is a common consequence that requires frequent monitoring. Radiotherapy (RT) of the pituitary gland, commonly used in adults, is generally avoided in children due to potential complications, although it may be more effective in a shorter time-frame [149]. Innovative RT techniques such as stereotactic radiosurgery are promising, with high tumour control rates and potentially reduced side effects [150].
Medical treatment of paediatric CS is under-reported. Ketoconazole, a steroidogenesis inhibitor, is commonly used to relieve symptoms and await radiotherapy [151]. Low-dose mitotane, an adrenolytic drug used in adrenocortical carcinoma and in patients with very severe CS, showed promise but should be used with caution because of adverse events [152, 153]. Trials of osilodrostat, a 11β hydroxylase blocking agent, approved for adults, are ongoing in children [154]. Benign adrenal tumours are usually treated with surgical resection, while bilateral adrenocortical hyperplasia usually requires bilateral adrenalectomy [155]. Treatment guidelines for children with adrenal cancer are lacking because of the rarity of this condition.
In cases of ectopic CS, if the source of ACTH secretion can be identified, the treatment of choice is surgical removal of the tumour [156, 157]. If surgical resection is not feasible or the source of ACTH cannot be identified, medical therapy is indicated, as previously discussed [156, 157].
Bilateral adrenalectomy may be considered for severe hypercortisolism and life-threatening clinical morbidities per se, or be performed when more definitive treatments, such as TSS, are not possible [142]. In addition, it can be considered a therapeutic option even in rare cases of ectopic CS, when the primary tumour is occult [156, 157]. Despite a remission rate of virtually 100%, complications such as Nelson’s syndrome, defined as radiological progression or new detection of a pituitary tumour on thin-section MRI associated with hyperpigmentation and increasing ACTH levels, may occur [158, 159]. When disease remission is achieved with reduced cortisol levels, complications mediated by excess cortisol also tend to improve. However, after cortisol normalisation, systolic BP remains elevated in more than 30% at 3 months after surgery and persists in more than 5% at 12 months after surgery [134]. A significant positive correlation was observed between systolic BP and disease duration [133, 134].
Phaeochromocytoma and catecholamine-secreting paraganglioma
The classification in 2017 of catecholamine-producing tumours from chromaffin cells of the adrenal medulla and sympathetic ganglia was developed by the World Health Organization (WHO): phaeochromocytoma (PCC) and catecholamine-secreting paraganglioma (PGL) [Data from: (Pathology and Genetics of Tumours of the Endocrine Organs. WHO Classification of Tumours, DeLellis RA, Lloyd RV, Heitz PU, Eng C (Eds), IARC press, Lyon, France 2004.)] [160]. According to the Endocrine Society recommendations, PCC and PGL are typically classed together and referred to as phaeochromocytomas and paragangliomas (PPGLs) [161]. The incidence of pheochromocytoma in children is approximately 1 in 1,000,000 per year, representing approximately 10% of all childhood adrenal tumours. Paragangliomas are even rarer and may be located in areas outside the adrenal glands, such as the neck, thorax, or abdomen. The majority of children are diagnosed before the age of 20, with a peak incidence in early childhood (3–5 years) for pheochromocytomas and later in adolescence for paragangliomas. PPGLs are probably seen in less than 0.2% of hypertensive adult patients [162, 163], while in children with hypertension the prevalence is higher and estimated at 1.7% [161]. Hereditary PPGLs can be divided into two cluster groups. Cluster 1 includes those due to mutations in genes encoding the von Hippel-Lindau (VHL) suppressor, the four-succinate dehydrogenase complex subunits (SDHA,* SDHB*,* SDHC and SDHD*) and, less commonly, the SDHA subunit flavinating enzyme (SDHAF2), and genes controlling fumarate hydratase, malate dehydrogenase2 and prolylhydroxylases 1 and 2 [164, 165].
The second cluster group comprises tumours caused by mutations in the neurofibromatosis type 1 (NF1) tumour suppressor gene, the rearranged during transfection (RET) proto-oncogene, the transmembrane protein 127 (TMEM127) gene and the MYC-associated factor X (MAX) gene [166–169]. These mutations cause dysregulation of cellular metabolism and the accumulation of intermediate metabolites, oncometabolites, which can contribute to tumour formation and progression. There is third cluster, which is extremely rare, involving mutation in then Wnt signalling pathway. There is a higher prevalence of extra-adrenal, multifocal, metastatic, recurrent, and hereditary PPGLs in children than adults [170–172]. Additionally, it establishes a correlation between these phenotypic features and a higher prevalence of noradrenergic and related cluster 1 hereditary tumours in pediatric patients compared to adults. However, in young people < 18 years, the distribution of germline mutations is significantly different, with VHL and SDHx mutations relatively more common, and MEN2 much less so [173].
Diagnosis
Clinical suspicion of PPGL should be raised in paediatric patients presenting with (a) signs and symptoms of catecholamine excess and (b) an incidentally discovered adrenal or extra-adrenal mass. Several investigations have demonstrated that assays of metanephrines, whether in plasma or urine, are superior to those of urine vanillylmandelic acid and homovanillic acid, or serum and urine catecholamines [174, 175].
Most importantly, metanephrines are secreted continuously from the tumours rather than the intermittent bursts of catecholamines. Biochemical testing for patients with a suspected PPGL should include plasma-free or urine (spot or 24-h) levels of normetanephrine and metanephrine. The assay should be conducted using liquid chromatography [174].Generally, plasma metanephrines have the highest sensitivity and specificity, but these are closely followed by urinary metanephrines. In the paediatric and adolescent age group, sample collection may be problematic. It is usually best to have the young person quietly recumbent for 20–30 min, with an in-dwelling cannula inserted after the use of a local anaesthetic cream [176, 177]. Most urinary collections are 24 h collections, usually acceptable for teenagers but difficult in a younger age group, when a random sample corrected for creatinine may be more suitable. Nowadays, measurement is best by LC-GCMS, which is least likely to be influenced by any concomitant medication, although these should always be borne in mind. Plasma or urinary samples collected during acute illness may give false positive results, while age-appropriate reference ranges should always be used, especially in the younger patient.
Imaging is often performed when biochemical testing shows an excess of catecholamine metabolites. The first step is computed tomography scan (CT) or MRI of the pelvis and abdomen are highly sensitive to detection 0.5 mm or larger cancers.
With MRI, phaeochromocytomas tend to appear hypo- or iso-intense on T1-weighted imaging and hyper-intense on T2-weighted imaging [178]. Functional imaging should be used to rule out metastases, screen for regional extension or multifocality, and diagnose incidental lesions that are highly suspect of being PPGL but have equivocal biochemical testing [178]. Various nuclear medicine techniques can be applied for functional imaging. Functional imaging techniques, such as scintigraphy with ^123^I-labelled meta-iodobenzylguanidine [MIBG] or positron-emission tomography [PET]–CT with ^68^Ga-labe classically led [Data from: ^(^Pathology and Genetics of Tumours of the Endocrine Organs. WHO Classification of Tumours, DeLellis RA, Lloyd RV, Heitz PU, Eng C (Eds), IARC press, Lyon, France 2004.)] [163, 164, 169] tetraazacyclododecane [Data from: (Pathology and Genetics of Tumours of the Endocrine Organs. WHO Classification of Tumours, DeLellis RA, Lloyd RV, Heitz PU, Eng C (Eds), IARC press, Lyon, France 2004.)] [163, 164, 169] -tetraacetic acid–octreotate [DOTATATE] or ^18^F-labeled l-dihydroxyphenylalanine [l-DOPA], are effective in localising PPGL, but where available ^68^Ga-dotatate scanning with CT or MRI is optimal [179].
Clinical presentation
About 50% of patients experience symptoms, which are often paroxysmal. The clinical presentation in children is often similar to adults, but there can be some variations. The condition is typically characterised by persistent or paroxysmal hypertension [180, 181], severe headache [181, 182] that may be localised to the temporal or occipital regions, palpitations, sweating and pallor. However, the range of clinical manifestations can be wide and include abdominal pain, tremors and weight loss [180, 182]. The symptoms can also be affected by the location of the tumour. Adrenal tumours that increase adrenaline and its metabolite product, metanephrine, commonly trigger an adrenergic response. Additional adrenal lesions mostly cause a noradrenergic response by secreting noradrenaline, and normetanephrine which is produced by intracellular metabolism of noradrenaline [183]. It should be noted that the presentation of phaeochromocytoma can vary widely among individuals. Some children may be asymptomatic or present with atypical symptoms. Diagnosis can be challenging as these symptoms are not specific to phaeochromocytoma and may require a high index of suspicion, especially in children.
Children versus Adults
While classically most patients were diagnosed on the basis of symptoms or with resistant or paroxysmal hypertension, increasingly in adults these are being picked up as incidentally-found adrenal tumours. In children and young adults, the diagnostic algorithm is rather different, with many being diagnosed on surveillance screening, the patient having been identified as contacts of index patients with a germline mutation. Indeed, germline mutations are seen in around 80% of patients in the younger age groups, as opposed to the 25–50% in adults, above the age of 25 years. These tumours are also more likely to be paragangliomas rather than phaeochromocytomas, and multifocal, and metastatic [171].
Treatment
Surgical removal is the primary treatment for PPGL. The decision to proceed with surgical intervention and the selected surgical approach should be discussed at a specialist multidisciplinary team meeting. The surgical procedure should be performed by a surgeon with expertise in the surgical management of PPGLs [174].However, it is important to note that during surgery, a large amount of catecholamines may be released, leading to a ‘catecholamine storm’. This can increase the risk of hypertensive crises, cardiac arrhythmias, myocardial ischaemia, pulmonary oedema, and stroke. The management of hypertension in children with phaeochromocytoma necessitates a comprehensive approach to regulate the BP while preparing the patient for surgical excision of the tumour. To manage hypertension and avoid hypertensive crises during surgery, it is common practice to begin with α-adrenergic blockade for at least 7–10 days. Phenoxybenzamine is the preferred α-blocker for use in children, although parenteral phentolamine may also be considered [184, 185]. In order to control tachycardia and palpitations, β-blockers may be added to the treatment regimen after adequate α-blockade has been achieved. It is important to note that β-blockers should not be initiated until α-blockade has been established, as unopposed α-adrenergic stimulation could worsen hypertension. Adrenergic blockade should be combined with a high-sodium diet of 5000 mg per day and a fluid intake of 2.5 L per day. In the event of hypertensive crises, it may be necessary to promptly intervene with short-acting anti-hypertensive medications such as sodium nitroprusside or nitroglycerine to rapidly lower BP and mitigate end-organ damage.
The initial surgical procedure for phaeochromocytoma involves an open laparotomy and total adrenal gland excision. This method is now the standard of care due to its many advantages, including reduced operation time, complication rates, and hospital stays [172]. Individuals with synchronous bilateral phaeochromocytomas who are having simultaneous bilateral adrenalectomy can benefit from a cortical-sparing strategy for patients with mainly benign disease, as in VHL or MEN-2, but is contraindicated where there is a metastatic tendency as in SDHx-mutated patients. Additional treatment methods, such as stereotactic radiosurgery and external radiation therapy, are often necessary when managing head-and-neck paragangliomas [186].
Metastatic PPGLs cannot currently be cured, but they may be indolent and survival for many years is not infrequent. Therefore, the treatment aims to alleviate symptoms caused by an excess of catecholamines, local mass effect, pain from metastases, and the overall burden of the tumour [187, 188]. This is especially the case for tumours seen in young people, with SDH-B mutated tumours most likely be metastatic. In such cases treatment may be delayed until there is clear progression, with increasingly early use of somatostatin analogues or peptide receptor radionuclide therapy (PRRT) with ^177^Lu-dotatate, which has increasingly replaced ^131^I-mIBG therapy. For more rapidly progressive disease or where the tumour is unsuitable for radionuclide therapy, temozolomide or CVD (cyclophosphamide/vincristine/dacarbazine) can be used.
The long-term outcomes and quality of life for children with pheochromocytoma and catecholamine-secreting paraganglioma following surgical resection and medical therapy are influenced by a number of factors, including tumour characteristics, genetic predispositions and the necessity for ongoing monitoring. Surgical resection remains the primary treatment option, with long-term follow-up essential due to the risk of recurrence. It is recommended that children with a germline pathogenic or probable pathogenic variant in a PPGL predisposition gene be offered lifelong clinical follow-up [174].
Peripheral glucocorticoid and mineralcorticoid pathway disorders
Apparent mineralcorticoid excess
Epidemiology
Apparent mineralocorticoid excess (AME) is an extremely rare monogenic juvenile hypertensive syndrome with a prevalence that remains uncertain but estimated as < 1/1,000,000, although it probably varies between populations, depending on the level of kinship and endogamy [189]Data from: Orphanet Reports. www.orpha.net). Approximately one hundred AME cases have been described clinically and genetically worldwide and reported in the literature so far [189](Data from: Orphanet Reports. www.orpha.net) [190]. No sex predominance is reported for the disease [189].
Pathogenesis
Cortisol and aldosterone are secreted from the zona fasciculata and glomerulosa of the adrenal cortex, respectively. Cortisol is secreted in larger physiologic amounts than aldosterone, being in orders of magnitude 1000 to 2000 times higher [191, 192]. Both hormones display the same binding affinity for the MR, potentially modulating blood pressure. Endogenous cortisol availability in aldosterone target tissues, such as the distal nephron, the colon epithelial cells, and the salivary glands, is modulated by the action of the enzyme 11β-dehydrogenase type 2, whose gene, HSD11B2, is located on chromosome 16q22.1 [191, 193–195]. Indeed, 11β-HSD2 catalyses the conversion of cortisol to the less active metabolite cortisone, thus protecting the MR from illicit cortisol activation [191, 193–195]. Thus, compromised 11β-HSD2 activity leads to over-activation of the MR by endogenous cortisol with consequent induction of renal sodium retention and a salt-sensitive increase in BP. There are several causes of compromised 11β-HSD2 activity, including gene mutations or inhibition of this enzyme by xenobiotics such as the glycyrrhizic acid, an ingredient of liquorice.
AME is an inherited autosomal recessive disorder caused by homozygous or compound heterozygous loss-of-function mutations or deletions in the HSD11B2 gene, which has been mapped to chromosome 16q22 and consists of five exons (Data from: Orphanet Reports. www.orpha.net.) [190, 196]. Most of the known 51 mutations are found in exons 3, 4 or 5 of the HSD11B2 gene, rarely in exon 1 and exon 2 [197]. A few mutations were found to not alter the amino-acid sequence but were potentially implicated in aberrant splicing [198]. In all cases, these mutations lead to abolition or a marked decrease in the 11β-HSD2 activity. Furthermore, the presence of single nucleotide polymorphisms, variations in microsatellite regions and epigenetic modifications in the HSD11B2 gene, can affect its expression and thus prejudice the 11βHSD2 enzyme activity (Fig. 1) [192, 199, 200].Fig. 1. Cell mechanisms and therapy in Apparent Mineralcorticoid Excess. In renal cells of the cortical collecting duct (CCD), when 11β-HSD2 activity is decreased, as a consequence of inherited or acquired mutations, intracellular cortisol level increases, leading to activation of the MR. The binding of the mineralocorticoid receptor (MR) to its hormone response element on DNA increases the transcription of genes encoding specific aldosterone-inducible proteins, such as the rate-limiting subunits of the apical epithelial sodium channel (ENaC) and basolateral Na/K-ATPase, thus producing Na^+^ retention, volume expansion and hypertension. Spironolactone and eplerenone are MR antagonists. Amiloride is an ENaC blocker. Created with Biorender.com.
Diagnosis
Mutations in the HSD11B2 gene cause the AME [191, 193–195]. AME represents a rare form of pseudo-hyperaldosteronism characterised by very early-onset and severe hypertension, associated with low renin levels and hypoaldosteronism. Besides the clinical characteristics, the diagnosis is based on biochemical findings of hypokalaemia, metabolic alkalosis, hyporeninaemia, hypoaldosteronaemia, and the detection of a marked increase (10 to 100-fold) in the ratio of cortisol/cortisone and tetrahydrocortisol/tetrahydrocortisone in plasma and urine. Genetic sequencing or HSD11B2 gene mutations is available to confirm the milder form of AME (non-classical AME) characterizsed by less marked hypertension and only mild abnormalities of cortisol metabolism (Data from: Orphanet Reports. www.orpha.net.) [194].
Clinical presentation
Generally, in AME, compromised 11βHSD2 enzyme activity results in overstimulation of the MR by cortisol, causing sodium retention, hypokalaemia, and salt-dependent hypertension. However, patients with HSD11B2 mutations showed varying degrees of severity in terms of clinical and biochemical features, according to the residual in vivo activity of the mutant 11βHSD2 enzyme. Mutations can cause a spectrum of manifestations and severities of the disease and depending on AME phenotypic severity, two forms can be recognised: classic and non-classic AME. and non-classic AME.
Classical AME starts very early in childhood, and it is characterised by a severe phenotype with low birth weight, failure to thrive, poor growth, severe and refractory hypertension, hypokalaemia, suppressed plasma renin activity with hypoaldosteronemia, polyuria, polydipsia, metabolic alkalosis and nephrocalcinosis. Non-classical AME is commonly diagnosed in adolescents or adults who develop the disease much later. than children with classic AME. Patients with non-classical AME present milder phenotypes including slight hypertension, increased biomarkers of renal and endothelial damage, like microalbuminuria and plasminogen activator inhibitor-1, and increased inflammation parameters, such as C-reactive protein and TNF-α [196–198].
Treatment
Treatment of AME consists of the use of MRAs and ENaC blockers such as spironolactone or eplerenone and amiloride, respectively, along with dietary sodium restriction and potassium supplementation to ameliorate hypertension (Fig. 1) [191, 194].
Liddle syndrome
In the distal nephron, the two main Na-transporting cell types are the Distal Convoluted Tubule (DCT) and the Principal Cells (PS). In the first group of cells, the luminal Na-transporter is the thiazide sensitive sodium chloride (NaCl) cotransporter (NCC) [194, 201]. The electroneutral reabsorption of sodium, particularly in the early distal tubule, is predominantly facilitated by the phosphorylation of the thiazide-sensitive sodium chloride cotransporter (NCC) through a complex network of kinases, with regulation by angiotensin II and aldosterone through mechanisms that are still not fully understood [202].
In the Principal cell, sodium transportation is mediated by the ENaC [194], which is composed of three subunits, named α, β and γ. ENaC participates in a process that involves transepithelial ionic transport between the lumen of the renal collecting duct and the blood. Through its opening, Na + is actively transported across the basolateral membrane via the Na+/K+-ATPase, which operates in exchange for potassium ions [203]. At the physiological level, the channel is positively regulated by aldosterone and antidiuretic hormone [204].
Among monogenic forms of hypertension, mutations involving distal nephron Na + transport, such as Liddle Syndrome and Gordon Syndrome, play a significant role.
Epidemiology
Liddle syndrome (LS) is a juvenile form of genetic hypertension caused by point mutations of the ENaC, that cause aldosterone-independent sodium reabsorption in the distal nephron [205]. LS is a rare condition, and data describing formally diagnosed patients reported only 30 cases until 2008 [206]. Nevertheless, it may be considered the most common type of monogenic hypertension, being reported in many ethnic populations, including Caucasians, Asians, and Black people [194]. The prevalence across the general population of hypertensive young population is uncertainly reported at between 1.52% and 0.89% in two recent Chinese studies [207, 208].
Pathogenesis and Genetics
LS consists of a genetically determined defect in the distal tubular transport system, in which gain-of-function mutations of ENaC cause a constitutive activation of distal tubular sodium and water absorption [201]. This results in volume expansion and hypertension, onsetting at a young age. The disease is inherited in an Mendelian autosomal dominant fashion [209]. The causative point mutations are highly diverse, mostly involving the ENaC β (or SCNN1B) and γ (SCNN1G) subunits genes, located in 16p12 chromosome [210], although a mutation in SCNN1A encoding for the α-subunit was recently described [211]. To date, so far, the discovered mutations are reported as missense, nonsense and frameshift mutations, before or within the interested codon [210].
Depending on the affected ENaC subunit, LS is classified into three types: type 1 (β subunit, OMIM #177200), type 2 (γ subunit, OMIM #618114), and type 3 (α subunit, OMIM #618126) [201]. The pathogenetic mechanism consists of deletions or substitutions in a short proline-rich amino acid sequence of the C-terminus of SCNN1B and SCNN1G, which leads to inability of β and γ subunits to bind to an intracellular ubiquitin protein ligase (Nedd4) that physiologically removes the channel from the cell surface. Thus, the increased exposition of ENaC channels on the cell surface enhances sodium reabsorption, aldosterone-independently [210].
Diagnosis
Diagnosis relies on clinical suspicion, triggered by findings of normo/hypertension and hypokalaemia in a juvenile age. Low renin and aldosterone levels typically result from volume expansion due to increased sodium reabsorption [205, 212]. A negative family history should not be an exclusion criterion, as de novo mutations have also been identified. A good response to ENaC Blockers can be considered as diagnostic confirmation. Genetic sequencing can confirm the diagnosis [206].
Presenting features
Clinical features associated with LS can be recognised in an early-onset resistant arterial hypertension, associated with hypokalaemia and kaliuresis, metabolic alkalosis, suppressed plasma renin activity and low serum aldosterone levels [194, 201]. The clinical portrait of uncontrolled hypertension could also be associated with cardiovascular complications, such as premature stroke, myocardial infarction, sudden death in young age [191, 213]. LS types 1 and 2 usually present in late childhood or adolescence, but they can also occur in infancy. Indeed, patients can be diagnosed very early, thus any infant presenting with hypertension and metabolic alkalosis, with or without hypokalaemia, should raise the suspicion for LS [214].
Apart from the classical presentation, cases can also be asymptomatic, being diagnosed late in adulthood [194, 201, 205]. Particularly, since approximately 7–8% of patients diagnosed with LS are normotensive [205], and considering the incomplete penetrance of the disease, it is important to screen for this condition in individuals presenting with refractory hypertension or isolated hypokalaemia, particularly when suppressed aldosterone and renin levels are associated with a strong family history of severe or refractory hypertension and/or hypokalaemia [215]. Notably, genotype-phenotype correspondence is not always maintained, even within extremely severe phenotypes and mild forms within members of the same family, probably due to unknown environmental influences.
Treatment
Amiloride is an ENaC blocker and the use of this drug is highly effective in treating LS, as well as triamterene, at a dosage of 2.5–40 mg daily for amiloride and 50–100 mg daily for triamterene. Conversely, MRAs such as spironolactone or eplerenone are ineffective, since ENaC constitutive activation is aldosterone-independent, the lack of response is also highly informative in the diagnostic context [212]. Dietary sodium intake restriction (typically less than 2 g NaCl daily) could improve the efficacy of ENaC blockers, and should be initiated as an additional therapy in all patients with LS. Along with hypokalaemia and hypertension, cardiac, neurological, renal, and ophthalmic sequelae of hypertension are common. Therefore, they should be assessed and treated when necessary [205].
Gordon syndrome (or Pseudo-hypoaldosteronism type II or Familial hyperkalaemic Hypertension)
Gordon Syndrome (GS), a rare form of monogenic familial hypertension, typically associated with hyperkalaemia, which sets it apart from other syndromic forms of hypertension, which lead to hypokalaemia.
Epidemiology
GS is defined as a rare form of hypertension. Its true prevalence is unknown.
Pathogenesis and Genetics
Four genes associated with the regulation of the NaCl cotransporter NCC (thiazide-sensitive sodium chloride cotransporter in distal convoluted tubule cells) have been associated with Gordon phenotypes: WNK1 and WNK4, which encode a family of WNK (with-no-lysin) kinases, and KLHL3 and CUL3, encoding Kelch-like 3 protein and Cullin 3, respectively [216]. No activating mutations in the NCC itself have been found so far. Inheritance occurs mostly in an autosomal dominant fashion [217].
Five subtypes of PHAII have been described, designated A to E. Type IIA has been associated with chromosome region 1q31-q42 with no gene yet identified, PHAII-B with specific variations in the WNK4 gene (OMIM # 601844) (17q21), and PHAII-C by mutations in the WNK1 gene (OMIM # 605232) (12p12.3.). Moreover, germline mutations in KLHL3 (OMIM # 605775) (5q31.2) and CUL3 (OMIM # 603136) (2q36) are related to PHAII-D and E, respectively [218]. De-novo mutations have been also described.
Mutations in all these genes, with various mechanisms, constitutively activate NCC, resulting in abnormal increased salt reabsorption in distal tubule and salt-sensitive hypertension. Furthermore, hypertension in GS is not solely linked to an increase in sodium and fluid reabsorption. Indeed, vascular endothelial dysfunction should be taken into account, due to an increased vascular smooth muscle tone, mediated by CUL3 deletion [219].
Presenting features
Diagnostic features, in addition to hypertension (not always present), are severe hyperkalaemia (reaching 8–9 mmol/L), which can lead to periodic paralysis, and metabolic hyperchloraemic acidosis without renal failure. Biochemical dosages show plasma renin activity suppression and variable aldosterone levels. The severity of hypertension, hyperkalaemia and metabolic acidosis varies according to different mutations [220], with an evident phenotype-genotype correlation, and some families or sporadic cases presented with milder symptoms [191]. Hypertension generally occurs in adolescence to adulthood. Rarely, neonatal presentations have been reported [221]. Notably, Spitzer-Weinstein syndrome in children is currently considered an early manifestation of GS in infancy, due to their similar clinical features [194].
Particularly in WNK4 mutations, hypercalciuria is also frequently found, even prior to development of hypertension [222], along with a decreased bone mineral density and without elevated parathyroid hormone or serum calcium [206, 216]. Furthermore, patients might show short stature and abnormal growth rate [223], dental abnormalities and intellectual disability [224].
Diagnosis
While PHA types 2 A, 2B, and 2 C are usually diagnosed in adolescence and adulthood, defects in CUL3 (type 2E) and autosomal recessive KLHL,3 mutations can present in infancy [225]. There are no formal diagnostic criteria for PHA II, with genetic investigations confirming the diagnosis.
Treatment
Hypertension in GS is strongly sensitive to salt restriction (20 mmol/d) [191], which can reverse symptoms [212]. Notably, since thiazide diuretics have a direct inhibitory effect on NCC, with low doses (50% of the age- and weight-adjusted dosage) being sufficient to achieve an excellent clinical and biochemical response, even for a long-term treatment [226].
Familial or sporadic primary generalised glucocorticoid resistance or Chrousos syndrome
Allostasis through a defective glucocorticoid receptor
At the cellular level, the actions of glucocorticoids are mediated by the glucocorticoid receptor (GR). The human GR (hGR) belongs to the steroid/thyroid/retinoic acid superfamily of nuclear receptors, and functions as a ligand-dependent transcription factor that regulates the expression of glucocorticoid responsive genes positively or negatively. The hGR is expressed by the NR3C1 gene, which is located on chromosome 5 (5q31.3), and contains 10 exons [227, 228]. Within the target cell, glucocorticoids signal through their cognate receptor, which is located mainly in the cytoplasm, and forms a protein complex with immunophillins and heat shock proteins. The structure of the receptor changes, allowing the GR to move to the nucleus. In the nucleus, the ligand-activated hGRα forms dimers (homo-or heterodimers) that bind to specific DNA sequences, which are known as glucocorticoid response elements (GREs). GREs are located in the regulatory or promoter regions of glucocorticoid-responsive genes, therefore modulating their expression.
In humans, the glucocorticoid signal transduction pathway exerts its functions in inverted U-shaped activity-effect curve. The optimal effect contributes to homeostasis or eustasis and is achieved in the middle of glucocorticoid signalling activity. Suboptimal effects may be present on each side of the inverted U-shaped curve and can cause insufficient adaptation. This state is termed allostasis or cacostasis [228]. These conditions may present with clinical manifestations of glucocorticoid resistance. Mutations of the NR3C1 gene can cause a rare familial or sporadic condition known as Chrousos syndrome, characterised by generalised or partial, target-tissue insensitivity to glucocorticoids, which leads to compensatory activation of the HPA axis and hypersecretion of ACTH in the systemic circulation. In Chrousos syndrome the clinical manifestations range from asymptomatic cases to severe cases of mineralocorticoid and/or androgen excess. In 2018, Vitellius et al. provided an estimation of the prevalence of NR3C1 mutations in 100 patients with bilateral adrenal hyperplasia, increased arterial pressure, and/or hypercortisolism, but without any stigmata of Cushing’s syndrome. They found that five of these patients (5%) carried novel heterozygous NR3C1 mutations [229].
Pathogenesis
The molecular basis of Chrousos syndrome has been ascribed primarily to mutations in the hGR gene, encoded by the NR3C1 gene, which is located on the short arm of chromosome 5, and contains 10 exons. Many different mutations were identified, and in vitro studies showed that each mutation can present with: impaired ability to bind to DNA, more time required to translocate into the nucleus following ligand-induced activation, lower affinity for the ligand than the wild-type receptor, decreased ability to transactivate glucocorticoid-responsive genes, and a marked delay to translocate into the nucleus and interacted with the GRIP1 coactivator mostly through its AF-1 domain. This results in impairment of the molecular mechanisms of hGR action and decreased tissue sensitivity to glucocorticoids [228, 230].
Clinical presentation
The decreased tissue responsiveness to glucocorticoids leads to compensatory activation of the HPA axis causing hypersecretion of ACTH. Adrenal cortex hypertrophy results and activates the biosynthetic pathway of cortisol, adrenal androgens [androstenedione, dehydroepiandrosterone (DHEA), and DHEA-sulfate (DHEAS)], and steroid precursors with mineralocorticoid activity (deoxycorticosterone and corticosterone).
Therefore, patients may be asymptomatic or may present with clinical manifestations of mineralocorticoid excess (hypertension and/or hypokalaemic alkalosis) and/or androgen excess (ambiguous genitalia in karyotypic females, precocious puberty, acne, hirsutism, male-pattern hair loss, and hypofertility in both sexes, oligo-amenorrhoea and menstrual irregularities in women, and oligospermia in men).
Diagnosis
In addition to documenting various clinical manifestations, gathering personal and family medical history is crucial. The endocrine assessment involves measuring serum cortisol levels at 08:00 AM, plasma ACTH, plasma renin activity (while recumbent), serum aldosterone, androgens (testosterone, androstenedione, DHEA, DHEAS), and insulin. The biochemical evaluation includes determining levels of total cholesterol, HDL, LDL, triglycerides, and fasting glucose. The 24-hour urinary free cortisol (UFC) excretion should be measured over 2 or 3 consecutive days. Serum cortisol levels can be up to seven times higher than the upper limit of the normal range, while 24-hour UFC excretion can be up to fifty times higher than the upper normal range. ACTH levels may be normal or elevated.
The dexamethasone suppression test involves administering increasing doses of dexamethasone (0.3, 0.6, 1.0, 1.5, 2.0, 2.5, 3.0 mg) orally at midnight on alternate days, with serum cortisol and dexamethasone levels measured at 08:00 AM the following morning. It is also important to consider measuring serum dexamethasone levels concurrently to rule out non-adherence to treatment, increased metabolic clearance, or reduced absorption of the medication.
Two primary molecular biology methods confirm the diagnosis of Primary Generalised Glucocorticoid Resistance: dexamethasone-binding assays and thymidine incorporation assays [228, 231].
Therapy
The main objective in Chrousos syndrome is to suppress ACTH, thus lowering the increased production of adrenal steroids with mineralocorticoid and androgenic activity. Treatment consists of the administration of high doses of dexamethasone (1–3 mg given once daily at night), which suppress the endogenous secretion of ACTH in affected subjects. Dexamethasone should be carefully titrated according to the clinical manifestations and biochemical profile of the patients. It is crucial to achieve adequate suppression of the HPA axis to prevent the development of an ACTH-secreting adenoma [231].
Conclusions
The diagnosis and management of endocrine hypertension during childhood and transition age still represent a significant clinical challenge today [232]. Biochemical and clinical aspects to be considered in the differential diagnosis of adrenal causes of hypertension, and brief hints about treatment are summarised in Table 1. [23]. Arterial hypertension can lead to cardiovascular morbidity, mortality, and organ damage, and when it occurs during childhood or the transition to adulthood, secondary causes of hypertension have to be investigated, diagnosed early and treated.Table 1. Summary table adrenal causes of hypertension during childhood and adolescenceAdrenalDisorderGerminal mutations geneAge at hypertension onsetGender prevalenceK^+^ReninAldosteronCortisolACTHOther suggestive biochemical aspectsSuggestive clinical aspectTreatmentReferences11β-hydroxylase deficiencyCYP11B1Variable:0–17 yrs–↓↓↓N/↓↑↑ DOC, Increased 17 OH PRG, 11-deoxycortisol, androstenedione, testosterone, DHEA-SAmbiguous genitalia, Virilization/PCOS phenotype in F,Precocious puberty, short stature, TART in MMRAs, ENaCiCortisol substitution if neededAntiandrogens if neededK^+^implementation if needed15–34, 23517-hydroxylase/17,20-lyase deficiencyCYP17A1Variable:Mainly adolescence–↓↓N/↑↓↑↑ Corticosterone↑ DOC↑ Pregnenolone↑ Progesterone↓/N androstenedione ↓/N testosterone↓/N DHEA-S↓/N 17OHprogesteroneAbnormal sexual differentiation in MLack of breast development, Ovarian cysts, Amenorrhea and Infertility in FMRAsTe in MEP in F35–51FH1CYP11B1-CYP11B2**Chimeric geneVariable:< 20 yrs–N/↓↓↑NN↑ 18-oxo-cortisolMicro/macro vascular complications, cardiac remodeling, Myocardial infarction and stroke at young ageLow dose GCsMRAsK^+^implementation if needed55–67, 235FH2CLCN2Variable:< 20 yrs–N/↓↓↑NNAlkalosisMRAsK^+^implementation if needed, adrenalectomy if needed56–57,68–75,FH3KCNJ5Variable:5yrs-adult age–N/↓↓↑NNAlkalosisSevere phenotype:Early-onset drug resistant hypertension,Polyuria, Polydipsia, Myalgia, Growth retardationMilder phenoptype: milder/later-onset hypertension showing favorable disease progression during growthMRAs and other antihypertensive drugsK^+^implementation if needed, Adenalectomy if needed56–57,69,76–92FH4CACNA1HVariable:< 10 yrs-adult age–N/↓↓↑NNAlkalosisSevere phenotype: Mental retardation, growth retardation, learning disordersMilder phenotype:no PA/PA in adult ageMRAsK^+^implementation if needed56–57,93–99CANCA1D- related hyperaldosteronismCACNA1DVariable:0-5yrs–↓↓↑NNHyperinsulinemia hypoglycemiaAlkalosisCardiac abnormalities, Congenital deafness, Neonatal hypoglycemiaDihydropyridine Ca^++^ antagonists57,100–108CSPRKAR1,GNAS,* MEN1*,* TP53*,* MSH2*,* MLH1*,* PMS2*,* MSH6*,* EPCAMVariable:(if < 5 yrs consider mainly CS)F > MN/↓NN↑↓ in CS N/↑ in CD↑24 h UFC↑ LNSC↑midnight serum cortisol↑morning serum cortisol after DSTCushingoid phenotype: facial rounding, weight gain, growth retardation and increased virilizationSteroidogenesis inhibitors (Ketoconazole, Osilodrostat)Low dose mitotane(Caution in use of medical treatments: surgery to be preferred when feasible)109–130,141–155, 235PPGLSDHx*,* VHL*,* SDH*,* MEN2*,* NF1Variable–NNNNN↑ Plasma metanephrines↑ Urine metanephrinesSevere headache, Palpitations, Sweating,Pallor,Abdominal pain, Tremors,Weight lossPerioperative treatment:Phenoxybenzamine or Phentolamine, ꞵ-blockers if neededHypertensive crisis:Sodium nitroprusside, Nitroglycerin or other antyhypertensive drugs164–188Apparent mineralcorticoid excessHSD11B2*Variable:Very early childhood/adolescent/adult ageNoN/↓↓↑NNAlkalosisSevere phenotype:Low birth weight, Failure to thrive, Poor growth, Alkalosis, Nephrocalcinosis, Polyuria, PolydipsiaMild phenotype: Slight/late onsethypertensionMRAs/ENaCiK^+^implementation if needed192–194, 196, 199
Among the potential causes of hypertension at these ages, adrenal disorders such as enzyme defects in steroidogenesis, FH and CS, lead to an accumulation of hormones or steroidogenesis metabolites with mineralocorticoid activity, resulting in various degrees of severity of hypertension associated with hypokalaemia and sometimes alkalosis. The forms of congenital adrenal hyperplasia causing hypertension may mask inadequate glucocorticoid secretion, leading to the risk of adrenal crises under stress conditions, and therefore deserve attention for the evaluation of possible glucocorticoid replacement therapy.
If the steroidogenetic pathway leading to the production of androgens is enhanced, a clinical picture of congenital genital ambiguity with virilisation in females and hyperandrogenism can occur. On the contrary, when the deficient enzymatic step is necessary for the production of sexual steroids, genital ambiguity with feminisation in the male and amenorrhea and a PCOS-like syndrome in the female can occur.
A picture of hypertension accompanied by genital ambiguity at birth or alterations of puberty in males or amenorrhoea in females must therefore raise the suspicion of CAH. The various forms of familial hyperaldosteronism can present with a notable variability in the severity of hypertension, of the associated hypokalemia and cardiovascular damage, with incomplete penetrance or various patterns of mosaicism contributing to the heterogeneity of the clinical and biochemical characteristics.
The presence of peculiar clinical characteristics such as hyperinsulinaemic hypoglycaemia at birth or neuropsychiatric manifestations such as those of PASNA or congenital cardiac anomalies can direct investigations towards the diagnostic suspicion of a specific type of FH. The response to medical treatment can also influence the type of FH (good clinical response to GCS or CA antagonists). Definitive diagnosis requires genetic tests aimed at searching for the above-mentioned germline mutations.
The early diagnosis and the extension of molecular investigations to family members, even if asymptomatic, are necessary as the onset of FH can be late and FH can expose the risk of cardiovascular events at a young age. The presence of a Cushingoid phenotype, often associated with excessive obesity but poor growth, especially in association with a dysmetabolic pattern, must raise clinical suspicion of endogenous hypercortisolism, and early diagnosis and treatment are essential, given the long-term comorbidities associated with chronic hypercortisolism. Morphological investigation should be performed in all cases of hypercortisolism to exclude the rare malignancies and to identify specific morphological adrenal characteristics such as pigmented nodular adrenocortical disease.
Phaeochromocytomas and paragangliomas, quite frequent in children with hypertension, present with a peculiar clinical picture compared to other forms of adrenal hypertensions and require a multidisciplinary approach in evaluating the appropriate treatment and in-depth biochemical and molecular investigations to exclude a systemic genetic syndrome. Prompt identification of adrenal causes of secondary hypertension is crucial for timely and effective management, addressing systemic manifestations such as electrolyte imbalances and early cardiovascular events associated with hypertension. In conclusion, this review underlines the importance of recognising the clinical characteristics suggestive of adrenal pathologies causing endocrine hypertension and of promptly directing these patients to referral centres for the advanced diagnosis and the personalised treatment of these rare pathologies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Stergiou GS, Palatini P, Parati G, O’Brien E, Januszewicz A, Lurbe E et al (2021) 2021 European Society of Hypertension practice guidelines for office and out-of-office blood pressure measurement. J Hypertens [Internet]. [cited 2024 Oct 9];39:1293–302. Available from: https://journals.lww.com/10.1097/HJH.000000000000284310.1097/HJH.000000000000284333710173 · doi ↗ · pubmed ↗
- 2Rao G, Diagnosis Epidemiology, and Management of Hypertension in Children. Pediatrics [Internet]. 2016 [cited 2024 Oct 9];138:e 20153616. Available from: https://publications.aap.org/pediatrics/article/138/2/e 20153616/52413/Diagnosis-Epidemiology-and-Management-of 10.1542/peds.2015-361627405770 · doi ↗ · pubmed ↗
- 3Dormanesh B, Arasteh P, Daryanavard R, Mardani M, Ahmadi M, Nikoupour H (2023) Epidemiology of obesity and high blood pressure among school-age children from military families: the largest report from our region. BMC Pediatr [Internet]. [cited 2024 Oct 9];23:37. Available from: https://bmcpediatr.biomedcentral.com/articles/10.1186/s 12887-023-03839-z 10.1186/s 12887-023-03839-z PMC 986849136683049 · doi ↗ · pubmed ↗
- 4Maldonado J, Pereira T, Fernandes R, Santos R, Carvalho M (2011) An approach of hypertension prevalence in a sample of 5381 Portuguese children and adolescents. The AVELEIRA registry. Hypertension in Children. Blood Press [Internet]. [cited 2024 Oct 9];20:153–7. Available from: http://www.tandfonline.com/doi/full/10.3109/08037051.2010.54264910.3109/08037051.2010.54264921142582 · doi ↗ · pubmed ↗
- 5Chiolero A, Cachat F, Burnier M, Paccaud F, Bovet P (2007) Prevalence of hypertension in schoolchildren based on repeated measurements and association with overweight. J Hypertens [Internet]. [cited 2024 Oct 9];25:2209–17. Available from: https://journals.lww.com/00004872-200711000-0000710.1097/HJH.0b 013e 3282 ef 48b 217921814 · doi ↗ · pubmed ↗
- 6Viggiano D, De Filippo G, Rendina D, Fasolino A, D’Alessio N, Avellino N et al Screening of Metabolic Syndrome in Obese Children: A Primary Care Concern. J Pediatr Gastroenterol Nutr [Internet]. 2009 [cited 2024 Oct 9];49:329–34. Available from: https://onlinelibrary.wiley.com/doi/10.1097/MPG.0b 013e 31819 b 54b 710.1097/MPG.0b 013e 31819 b 54b 719590449 · doi ↗ · pubmed ↗
- 7Jacobs DR, Woo JG, Sinaiko AR, Daniels SR, Ikonen J, Juonala M et al (2022) Childhood Cardiovascular Risk Factors and Adult Cardiovascular Events. N Engl J Med [Internet]. [cited 2024 Oct 9];386:1877–88. Available from: http://www.nejm.org/doi/10.1056/NEJ Moa 210919110.1056/NEJ Moa 2109191 PMC 956382535373933 · doi ↗ · pubmed ↗
- 8De Silva T, Cosentino G, Ganji S, Riera-Gonzalez A, Hsia DS Endocrine Causes of Hypertension. Curr Hypertens Rep [Internet]. 2020 [cited 2024 Oct 9];22:97. Available from: https://link.springer.com/10.1007/s 11906-020-01108-310.1007/s 11906-020-01108-333079272 · doi ↗ · pubmed ↗