A Case of Rare Adipocytic Tumor of the Tongue: Lipoblastoma-Like Tumor With RB1 Gene Deletion
Yoshihiko Sugita, Hiromasa Hasegawa, Rita R Roy, Katsumitsu Shimada, Takanaga Ochiai, Motohiko Nagayama, Hatsuhiko Maeda

TL;DR
A rare case of a lipoblastoma-like tumor on the tongue in an elderly woman is reported, with a genetic deletion in the RB1 gene and distinct histopathological features.
Contribution
This paper presents a novel case of a lipoblastoma-like tumor of the tongue with RB1 gene deletion, expanding the known clinical and molecular spectrum of these tumors.
Findings
The tumor exhibited a hemizygous deletion of the RB1 locus in 36% of cells.
Immunohistochemistry showed positivity for S100 but negativity for CD34, PLAG1, BCL-2, MDM2, CDK4, and DDIT3.
The tumor showed no recurrence five years after surgical removal.
Abstract
Lipoblastoma-like tumors (LLTs) are benign adipocytic tumors characterized by an admixture of lipoblasts within the myxoid stroma, primarily affecting the vulvovaginal area in young patients. Rare cases have been reported in other locations, including the orofacial region. Here, we present a unique case of LLT of the tongue in a 62-year-old woman with a slowly developing painless nodule. The tumor showed no signs of recurrence five years after surgery. Histopathological examination revealed a myxo-fatty lobulated lesion with numerous uni- and multi-vacuolated lipoblasts and prominent chicken-wire capillaries. Immunohistochemistry showed positivity for S100, whereas the tumor was negative for cluster of differentiation 34 (CD34), pleomorphic adenoma gene 1 (PLAG1), B-cell lymphoma 2 (BCL-2), mouse double minute 2 homolog (MDM2), cyclin-dependent kinase 4 (CDK4), and DNA damage-inducible…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1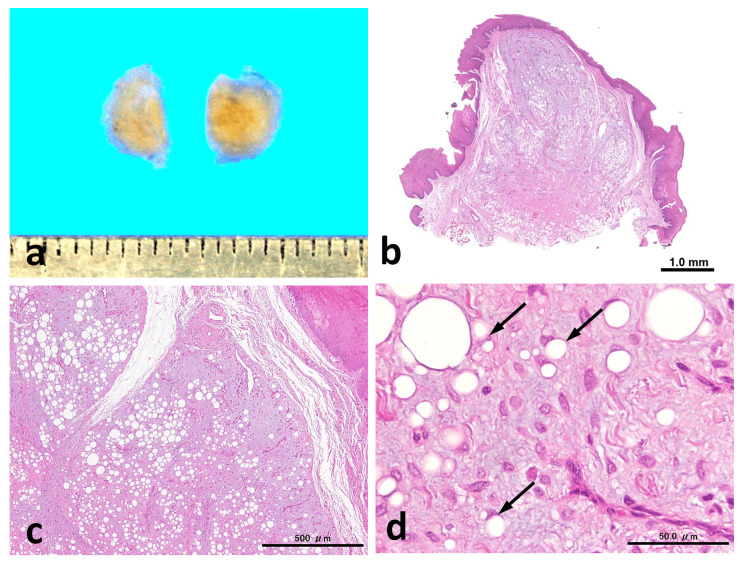 Figure 2
Figure 2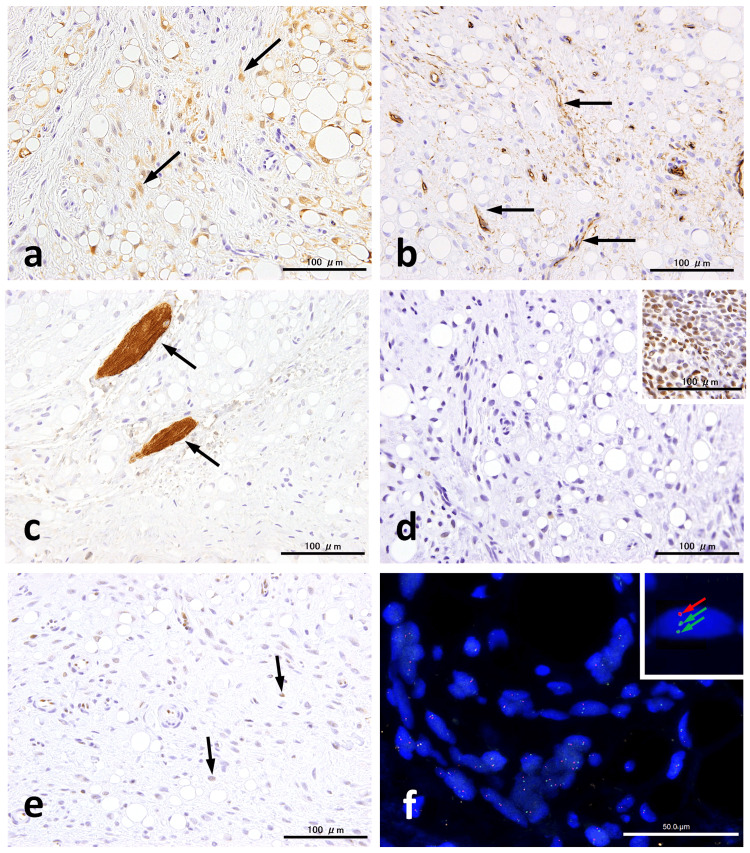 Figure 3
Figure 3| Findings | Lipoblastoma | Lipoblastoma-like tumor | Spindle cell lipoma | Myxoid liposarcoma |
| Age | Children* | Adult | Adult | Adult |
| Lobulation | Present | Present | Absent | Present |
| Lipoblasts | Abundant | Abundant | Scant | Scant |
| Myxoid | Abundant | Abundant | Variable | Abundant |
| Capillary network | Abundant | Abundant | Scant | Abundant |
| CD34 | Negative | Negative/focal | Positive | Negative |
| S100 | Positive | Positive | Focal | Focal |
| PLAG1 | Positive | Negative | Negative | Negative |
| Desmin | Positive | Negative | Negative | Negative |
| pRB loss | Negative | Mosaic | Positive | Negative |
| DDIT3 | Negative | Negative | Negative | Positive |
| Gene alteration | PLAG1 | Variable gains and losses# |
| FUS-DDIT3 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSoft tissue tumor case studies · Sarcoma Diagnosis and Treatment · Tumors and Oncological Cases
Introduction
A lipoblastoma-like tumor (LLT) is a benign adipocytic tumor characterized by an admixture of lipoblasts, myxoid stroma, and spindle cells, which is reminiscent of lipoblastoma, myxoid liposarcoma, or spindle cell lipoma (SCL). Originally, LLTs were considered lesions that primarily affected the vulvovaginal area in young patients [1,2]. However, rare instances of LLTs affecting the paratesticular region have been reported, indicating that LLTs are not limited to the vulvo-inguinal region in women [3]. Anatomical sites of LLTs have included the retroperitoneum, pelvis, shoulder, and forearm in both women and men [4,5]. Across reported series, lesions typically enlarge slowly, occasionally exceeding 20 cm [2,4,5]. LLTs generally behave in an almost entirely benign manner [4] but exhibit local recurrence in half of the cases with positive excision margins [2,5]. Exceptionally, one case of vulvar LLT that developed pulmonary metastasis was reported among 28 cases of LLTs [5].
Oral cavity involvement is exceedingly uncommon, with only three sporadic cases of the lip and tongue documented to date [6-8]. Two cases of LLT originating from the lip [6,7] did not exhibit the characteristic features of LLTs, such as spindle cells, myxoid stroma, and chicken-wire capillaries [1]. Nevertheless, the presence of lobules containing mature adipocytes and lipoblasts was consistent with LLTs. The other, involving the tongue, harbored an IDH1 mutation, a hitherto undescribed molecular alteration [8]. However, no additional cases of LLT affecting the intraoral mucosa have been reported.
The principal differential diagnoses of LLTs include myxoid liposarcoma, lipoblastoma, and SCL [1,2]. Ancillary testing aids in discrimination. Myxoid liposarcoma harbors FUS/EWSR1-DDIT3 fusions, and nuclear DNA damage-inducible transcript 3 (DDIT3) immunoreactivity is a highly sensitive and specific marker [9]. Lipoblastoma typically occurs in infants and children and often shows pleomorphic adenoma gene 1 (PLAG1) overexpression and PLAG1/HMGA2 rearrangements, with frequent cluster of differentiation 34 (CD34) and desmin expression [10,11]. SCL commonly exhibits diffuse strong CD34 and B-cell lymphoma 2 (BCL-2) staining and shows the loss of retinoblastoma protein (pRB) expression with 13q14/RB1 alterations in a substantial subset [12-15]. In contrast, LLT generally lacks PLAG1 expression/rearrangement and may show the complete or mosaic reduction of pRB, leading some authors to suggest a relationship with the SCL family while emphasizing distinct morphological and site predilections [2,4,5,15].
We report a unique adipocytic tumor of the tongue that presented with characteristic findings of LLT but exhibited a mosaic pRB pattern and a hemizygous loss of the *RB1 *locus. This case highlights the diagnostic challenges at the LLT-SCL interface and underscores the need for a practical, stepwise approach that integrates morphology, immunohistochemistry, and targeted molecular assays for the diagnosis of oral adipocytic lesions. Accurate diagnosis is essential because it supports conservative management for benign entities, prevents unnecessary treatment of lesions that resemble malignant tumors, and requires careful follow-up given the scarce long-term prognostic data for rare tumors such as LLT.
Case presentation
Clinical summary
A 62-year-old woman presented with a painless nodule on her tongue covered by normal mucosa (Figure 1). The lesion developed slowly over seven years. The tumor was surgically resected under local anesthesia because it was clinically diagnosed as a lipoma. No sign of recurrence five years after surgery.
Clinical findingsThe intraoral manifestations present as an elevated lesion on the dorsal tongue
Pathological findings
The excised specimen measured 5 × 5.5 mm in size and had a yellowish cut surface with mucosal elevation (Figure 2a). Histologically, the lesion was relatively well-demarcated, unencapsulated, and lobulated with a grenz zone between the epithelium and the tumor. The lobules separated by fibrovascular septa predominantly consisted of myxoid stroma, accounting for approximately 60%-70% of the tumor, and scattered adipocytes. The adipocytes contained variably sized vacuoles resembling mature adipocytes and uni-, bi-, or multi-vacuolated lipoblasts. The myxoid stroma contained bland spindle cells without any atypical features. Numerous thin-walled branching capillaries with a chicken-wire appearance were observed within the myxoid stroma. Collagen fibers were scant, and no ropy collagen was observed (Figure 2b-2d).
Histopathological findingsThe cut surface of the tumor appears yellow (a). Histologically, the tumor is unencapsulated (b) and composed of myxo-fatty lobules (c) made up of bland spindle cells, mature adipocytes, lipoblasts (arrows), and branching capillaries (d). Scale bars: 1.0 mm (b), 500 µm (c), and 50.0 µm (d)
Immunohistochemically, the variably sized adipocytic cells and some spindle cells were positive for S100 (polyclonal) (Figure 3a). CD34 (clone QBEnd/10) staining highlighted numerous small vessels but was mostly negative in tumor cells (Figure 3b). No desmin-positive tumor cells (clone D33) were identified (Figure 3c). However, desmin-positive striated muscle fibers were intermingled within the tumor. In contrast to the nuclear positivity for PLAG1 (clone 3B7) observed in a pleomorphic adenoma (Figure 3d), which served as a positive control, the tumor cells were completely negative. Some spindle cells were negative for pRB (clone G3-245), showing a mosaic staining pattern (Figure 3e). Additionally, the cells were negative for BCL-2 (clone 124), mouse double minute 2 homolog (MDM2) (clone IF2), cyclin-dependent kinase 4 (CDK4) (clone DCS-31), and DDIT3 (clone 9C8) (data not shown).
Immunohistochemistry and FISH analysisImmunohistochemistry shows spindle cells partially positive for S100 (a, arrows), while most are negative for CD34, which highlights the presence of capillaries (b). Desmin is completely absent in tumor cells but highlighted intermingled striated muscle fibers (c). PLAG1 expression is negative in contrast to the positive control case (inset) (d). pRB positivity is limited to spindle cells (arrows) and exhibits a mosaic pattern (e). RB1 FISH demonstrates a hemizygous RB1 deletion, indicated by a single RB1 signal (red arrow) and two centromere signals (green arrows) (inset). Scale bars: 50 µm (f) and 100 µmFISH, fluorescence in situ hybridization; CD34, cluster of differentiation 34; PLAG1, pleomorphic adenoma gene 1; pRB, retinoblastoma protein
Fluorescence in situ hybridization (FISH) was performed using ZytoLight SPEC RB1/13q12 and MDM2/CEN 12 (ZytoVision GmbH, Bremerhaven, Germany) dual-color probes. The analysis revealed a hemizygous deletion characterized by an orange signal corresponding to the RB1 gene and two green centromere signals, indicating the presence of two chromosome copies in 36% of the analyzed tumor cells (Figure 3f). No MDM2 amplification was detected (data not shown).
Discussion
The characteristic morphology of a lobulated myxo-fatty tumor affecting the tongue is similar to that of lipoblastoma. However, the diagnosis of LLT may be more appropriate given the patient’s age (62 years) compared to the age of lipoblastomas at diagnosis, which ranges from three months to 16 years, with 90% of cases diagnosed before 10 years [16]. Nevertheless, the morphological characteristics of this case included a complete set of LLTs, and the heterozygous loss of* RB1* should be carefully considered.
LLTs affect the external genitalia, particularly the vulva, but rarely other sites [3-5]. LLTs of the oral cavity are rare, with only three cases previously reported [6-8]. These showed a mixture of mature adipocytic cells separated by thin collagenous septa containing small vessels or striated muscles but lacking spindle cells and myxoid elements. However, the overall features of these cases, including CD34 negativity, were consistent with those of LLT.
The morphological features of LLT, rather than its clinical characteristics, suggest the need for a differential diagnosis, which includes myxoid liposarcoma, lipoblastoma, and SCL, as shown in Table 1 [1,2]. The FUS/EWSR1-DDIT3 fusion characteristic of myxoid liposarcoma can be distinguished from LLT using DDIT3 immunohistochemistry, in which nuclear anti-DDIT3 immunoreactivity is a highly sensitive and specific marker of myxoid/round cell liposarcoma [9].
Lipoblastomas typically occur in infants and children, and even in older children and adult patients, positivity for PLAG1, CD34, and desmin, along with PLAG1 and HMGA2 rearrangements, aids in diagnosis [10,11]. The histological findings in this case showed myxoid stroma, spindle cells, chicken-wire capillaries, and a mixture of mature adipocytes and lipoblasts, compatible with LLTs. Additionally, negative results for DDIT3, CD34, desmin, and PLAG1 support the diagnosis and help exclude myxoid liposarcoma and “adult” lipoblastoma [9-11].
Finally, differentiating between LLT and SCL is a significant issue in this case, as they share similar clinical characteristics except for their sites of occurrence [14,16]. Histologically, some SCLs with prominent lipoblasts closely resemble LLTs or lipoblastomas [17]. Additionally, desmin immunohistochemistry revealed that the tumor involved lingual muscle fibers, which may indicate the infiltrative nature of lipoblastoma rather than SCLs or LLTs [16].
From an immunohistochemical perspective, the absence of CD34 and BCL-2 expression in spindle cells suggests LLT, because SCLs typically exhibit diffuse and strong immunostaining for CD34 and BCL-2 [12,14]. Although pRB expression patterns in LLTs can vary, cases exhibiting complete loss or mosaic patterns are challenging to differentiate from SCL [4,18]. In this case, pRB demonstrated a mosaic pattern, which prompted us to perform *RB1 *FISH analysis. Contrary to our expectations, 36% of nuclei exhibited a hemizygous deletion of the RB1 locus. This result raises uncertainty as to whether the case is an LLT.
The frequencies of RB1 loss in SCLs vary, accounting for roughly 40%-60%, in contrast to the pRB deficiency observed in almost all cases [13]. Additionally, numerical and/or structural changes were found not only on chromosome 13 but also on chromosomes 1, 6, 11, and 12 [15]. Mirkovic and Fletcher reported that six cases of LLT of the vulva showed immunohistochemical loss of pRB but no expression of PLAG1, suggesting a relationship with the SCL tumor family [2]. However, molecular analyses were not performed in their study.
Another study showed that LLTs immunohistochemically exhibited a mosaic pRB pattern, and no evidence of RB1 regional gain or loss was identified using FISH [18]. As reported by Gross et al., several chromosomal abnormalities were noted, including gains on chromosomes 7 and 9, losses at 17q, and copy-neutral loss of heterozygosity at 11p, in three of eight cases tested using a chromosomal microarray [4]. Chromosomal aberrations were not observed on chromosome 13. Additionally, individual cases of LLT harboring mutations in MTOR, IDH1, PIK3CA, CSF1R, and* CDKN2A/B*,* *on chromosomes 1, 2, 3, 5, and 9, respectively, have been reported [4,5,8]. Given that these molecular aberrations vary between SCLs and LLTs, both lesions are heterogeneous with respect to chromosomal abnormalities. The hemizygous RB1 deletion in this case suggests an unusual variant of SCL that lacks CD34 and BCL-2. However, the morphological and immunohistochemical characteristics supported the diagnosis of LLT with RB1 loss.
This case highlights the challenge of distinguishing between LLT and SCL when confronted with conflicting immunohistochemical and genetic data. As mentioned above, we cannot completely rule out the possibility that this case represents an atypical example of SCL. Except for the presence of a hemizygous RB1 deletion, the morphological and immunohistochemical features were consistent with those of an LLT. Although LLT is not currently listed in the WHO classification of soft tissue tumors [19], likely due to its rarity and morphological overlap with established entities, the well-documented features of LLTs support the use of the term “lipoblastoma-like” for this diagnosis, as shown in the original report [1].
A limitation of this case report is the lack of a comprehensive molecular analysis, which hinders the provision of precise diagnostic information. Given the heterogeneity of the molecular characteristics of LLTs and SCLs, this case should be provisionally diagnosed based on the available morphological and immunohistochemical findings. Accumulating more cases involving extragenital areas is essential in further elucidating their nature and improving diagnostic accuracy.
Conclusions
This case illustrates that an LLT of the tongue can display classic morphology with hemizygous RB1 loss. Despite this genetic finding, the overall profile, DDIT3-negative, PLAG1-negative, and CD34/BCL-2-negative, supports an LLT over SCL. The clinical significance of RB1 alterations in LLTs is unknown. Broader molecular profiling across sites and larger cohorts is needed to clarify the boundaries between LLT and SCL and refine the terminology and criteria for these overlapping entities.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lipoblastoma-like tumour of the vulva: report of three cases of a distinctive mesenchymal neoplasm of adipocytic differentiation Histopathology Lae ME Pereira PF Keeney GL Nascimento AG 5055094020021204776010.1046/j.1365-2559.2002.01409.x · doi ↗ · pubmed ↗
- 2Lipoblastoma-like tumor of the vulva: further characterization in 8 new cases Am J Surg Pathol Mirkovic J Fletcher CD 129012953920152592935310.1097/PAS.0000000000000448 · doi ↗ · pubmed ↗
- 3A lipoblastoma-like tumour of the paratesticular region - male counterpart of lipoblastoma-like tumour of the vulva Histopathology Droop E Orosz Z Michal M Melegh Z 6286307620203162250210.1111/his.14020 · doi ↗ · pubmed ↗
- 4Lipoblastoma-like tumor and fibrosarcoma-like lipomatous neoplasm represent the same entity: a clinicopathologic and molecular genetic study of 23 cases occurring in both men and women at diverse locations Mod Pathol Gross JM Perret R Coindre JM 1002463620233730787410.1016/j.modpat.2023.100246 PMC 10530403 · doi ↗ · pubmed ↗
- 5Expanding the clinicopathologic and molecular spectrum of lipoblastoma-like tumor in a series of 28 cases Mod Pathol Anderson WJ Mariño-Enríquez A Trpkov K Hornick JL Nucci MR Dickson BC Fletcher CD 1002523620233735515310.1016/j.modpat.2023.100252 · doi ↗ · pubmed ↗
- 6Lipoblastoma-like tumour of the lip in an adult woman Acta Derm Venereol Jeong TJ Oh YJ Ahn JJ Shin MK Kim NI 5375389020102081464110.2340/00015555-0904 · doi ↗ · pubmed ↗
- 7Intradermal lipoblastoma-like tumor of the lip in an adult woman Actas Dermosifiliogr Val-Bernal JF Hermana S Sánchez R 889010720162635849810.1016/j.ad.2015.05.013 · doi ↗ · pubmed ↗
- 8Lipoblastoma-like tumor of the tongue with IDH 1 mutation: a case report and literature review Head Neck Li D Li G Wang Y Shi H Wang S Zhan X 07647202510.1002/hed.2810439925152 · doi ↗ · pubmed ↗