Immune-related osteitis mimicking femoral head osteonecrosis during dual checkpoint blockade: a case report
Enrica Teresa Tanda, Agostina Lagodin D’Amato, Giovanni Rossi, Maria Maddalena Latocca, Andrea Boutros, Andrea Zanirato, Matteo Formica, Silvia Bozzano, Bruno Spina, Francesco Spagnolo

TL;DR
A melanoma patient on immune therapy developed hip pain initially thought to be bone death, but it was actually immune-related bone inflammation.
Contribution
First documented case of immune-related bone inflammation without necrosis during checkpoint inhibitor therapy.
Findings
Hip pain in a melanoma patient was initially diagnosed as femoral head osteonecrosis.
Histopathology revealed immune-mediated osteitis with lymphoplasmacytic infiltrate and fibrosis.
This case highlights the need to recognize atypical immune-related adverse events in bone tissue.
Abstract
Immune checkpoint inhibitors (ICIs) have dramatically reshaped the therapeutic landscape of oncology, offering long-term survival benefits across multiple tumor types. However, ICIs are associated with a broad range of immune-related adverse events (irAEs), most of which are now well characterized and manageable. A subset of irAEs, however, remains rare, unpredictable, and poorly understood, both in terms of clinical presentation and pathogenesis. Here, we describe the case of a patient with advanced melanoma treated with combined anti-CTLA-4 and anti-PD-1 therapy who developed severe left hip pain during treatment. Imaging findings were initially suggestive of osteonecrosis of the femoral head. However, histopathological analysis of the resected femoral head revealed a dense lymphoplasmacytic infiltrate with fibrosis and vascular congestion, without evidence of bone necrosis,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
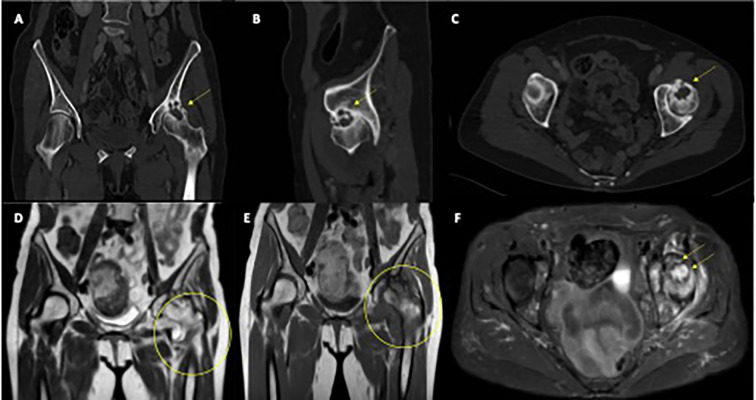 Figure 1
Figure 1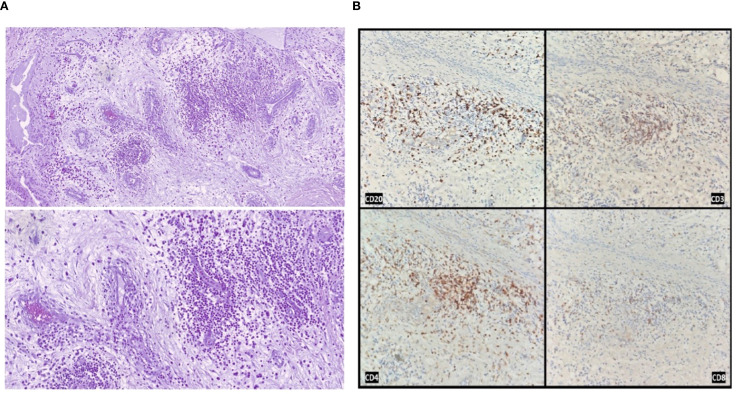 Figure 2
Figure 2| Feature | Classical osteonecrosis ( | Immune-mediated osteitis (this case) |
|---|---|---|
| Typical location | Femoral head, knee, proximal humerus* | Unknown |
| Pathogenesis | Ischemia due to vascular impairment (trauma, corticosteroids, alcohol) | Aberrant immune activation triggered by immune checkpoint inhibitors |
| Predisposing factors | Corticosteroids, alcohol, trauma, hematologic diseases | Immunotherapy with ICIs |
| Radiological features | Subchondral collapse, sclerosis, geodes, joint space narrowing | Bone marrow edema, joint effusion, synovial hypertrophy, no subchondral collapse |
| Histopathology | Empty osteocytic lacunae, trabecular collapse, absence of viable osteocytes | Dense lymphoplasmacytic infiltrates, fibrosis, preserved bone structure, neoangiogenesis |
| Inflammatory pattern | Minimal or absent | Active chronic inflammation with follicular lymphoid aggregates |
| Presence of neoplastic cells | Not applicable (unless metastasis present) | None (SOX10-negative, p40-negative, AE1/AE3-negative) |
| Clinical course | Progressive joint deterioration, high risk of collapse; surgical replacement often required | Symptom improvement after surgery; maintained oncological remission |
| Step | Orthopedic perspective | Practical notes for oncologists |
|---|---|---|
| When to suspect | New focal bone/joint pain (esp. load-bearing joints) during ICI; no trauma history; unusual MRI pattern (bone marrow edema without subchondral collapse) | Consider MRI early if pain persists >2–3 weeks |
| Initial workup | Focused history (trauma, alcohol, corticosteroids), exam for joint effusion; screen infection/inflammation | Basic labs (CBC, CRP/ESR) to exclude infection; plain X-ray as first line where appropriate |
| Differential diagnosis | Avascular necrosis, metastasis, septic arthritis, inflammatory arthritis, metabolic bone disease | Maintain broad ddx early; involve ortho/rheum/radiology as needed |
| Key imaging clues | Preserved bone structure, marrow edema, synovial hypertrophy, absence of necrotic bone on MRI | Coordinate radiology-orthopedic review. Ask radiology to comment explicitly on features arguing against AVN and metastasis |
| Histopathology clues | Dense lymphoplasmacytic infiltrate, fibrosis, vascular congestion, preserved trabeculae | Biopsy/surgical specimen only when infection or metastasis cannot be ruled out or surgery is indicated |
| Management principles | Symptom control; joint-preserving options vs arthroplasty depending on structural damage; avoid empiric antibiotics if infection unlikely | Multidisciplinary review (oncology, orthopedics, radiology, pathology ± rheumatology) |
| ICI management | Orthopedic input on structural risk; defer ICI decisions to oncology | Case-by-case decision on ICI hold/resume based on cancer status and severity of bone involvement, but mainly cease ICI |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBone and Joint Diseases · Bone health and treatments · Osteomyelitis and Bone Disorders Research
Introduction
The introduction of immune checkpoint inhibitors (ICIs) has revolutionized the treatment landscape of advanced melanoma (1). Recent 10-year results from the KEYNOTE-006 and CheckMate 067 trials have confirmed that approximately 50% of patients with advanced melanoma achieved long-term overall survival (OS) benefit with single agent PD-1 blockade or combined CTLA-4 and PD-1 blockade, respectively, marking an unprecedented shift in the natural history of this disease (2, 3).
Following these successes in advanced melanoma, ICIs have been rapidly integrated into the management of multiple solid and hematological malignancies, across both early and advanced disease settings.
Alongside the expanding indications for ICIs, oncologists have had to recognize and manage immune-related adverse events (irAEs), a spectrum of toxicities arising from immune hyperactivation and loss of self-tolerance.
Overall, irAEs are observed in up to 60–85% of patients receiving anti-PD-1/PD-L1 monotherapy and in over 90% of those treated with dual checkpoint inhibition (4). The most frequently involved systems include the skin (30–50%), gastrointestinal tract (15–30%), and endocrine glands (10–20%) (4).
Musculoskeletal irAEs, although less common (5–10%), typically manifest as inflammatory arthritis, polymyalgia-like syndromes, or myositis (4).
Despite the growing awareness of rheumatologic irAEs, bone tissue has historically been considered relatively spared from direct immune-mediated injury.
Only isolated cases of immune-mediated osteonecrosis of the jaw have been described, mostly in association with head and neck cancer treatments, and always histologically confirmed as true bone necrosis (5–8).
Here, we present the case of a patient with metastatic melanoma treated with combined anti-CTLA-4 and anti-PD-1 therapy, who developed a femoral head lesion initially suggestive of osteonecrosis on imaging. However, histopathological analysis revealed the absence of necrosis and the replacement of normal bone architecture by dense lymphoplasmacytic infiltration and fibrotic tissue.
To our knowledge, this represents the first reported case of an immune-mediated osteitis-like reaction involving bone during checkpoint inhibitor therapy.
Case report
A 76-year-old woman presented to the Emergency Department in May 2023 with severe anemia. Her past medical history included hypertension, mild osteoporosis managed with calcium and vitamin D supplementation, first-degree atrioventricular block, a previous bilateral hystero-oophorectomy for benign disease, and multinodular thyroid goiter.
A contrast-enhanced CT scan revealed a 65 × 35 mm vegetating gastric lesion, along with multiple secondary pancreatic nodules located in the head (11 mm), isthmus (11 mm), and body (12 mm) of the pancreas, findings later confirmed by abdominal MRI.
Esophagogastroduodenoscopy (EGDS) identified a mammillary, ulcerated lesion in the gastric fundus. Histological analysis of biopsy samples demonstrated metastatic melanoma, BRAF wild-type (assessed by PCR and Sanger sequencing), and PD-L1 negativity (TPS <1%).
To stabilize her condition, the patient first received hemostatic radiotherapy targeting the gastric lesion to control bleeding. Subsequently, in June 2023, she initiated first-line immunotherapy with the standard combination of nivolumab (1 mg/kg) plus ipilimumab (3 mg/kg) administered every 21 days for four cycles, followed by maintenance nivolumab (480 mg) every 28 days.
The treatment was generally well tolerated, with iatrogenic hypothyroidism emerging as the sole significant irAE, effectively managed with levothyroxine replacement.
First restaging scans demonstrated complete radiologic regression of both the gastric and pancreatic lesions. Incidentally, imaging also revealed severe left coxarthrosis characterized by joint space narrowing, coarse geodes, and femoral head deformation (Figures 1A–C).
Radiological features of left femoral head osteitis during immunotherapy. (A–C) CT scans show progressive deformation and sclerosis of the left femoral head (yellow arrows). (D, E) Coronal T1-weighted MRI images demonstrate diffuse bone marrow edema and joint effusion (yellow circles). (F) Axial T2-weighted MRI highlights extensive marrow edema and synovial hypertrophy (yellow arrows).
The patient continued anti-PD-1 maintenance therapy with excellent tolerance and maintained a complete pathological response, confirmed through multiple negative EGDS-guided biopsies.
In March 2024, she developed new-onset severe left hip pain radiating to the ipsilateral lower limb.
Pelvic and spinal imaging revealed marked progression of left hip arthropathy, raising suspicion for an osteonecrotic process (Figures 1D–F). MRI of the left hip showed features consistent with osteonecrosis, including diffuse bone marrow edema, focal osteochondral lesions of the acetabular roof, abundant joint effusion, synovial hypertrophy, and adjacent muscle edema (Figures 1D–F).
An urgent orthopedic consultation led to the decision to perform left total hip replacement, which was carried out in July 2024.
Intraoperatively, a pink, soft, non-bleeding tissue was noted extending from the femoral neck to the acetabulum, associated with extensive bone erosion.
Given the patient’s history, a suspicion of metastatic melanoma prompted the surgical team to submit the femoral head for histopathological analysis.
Microscopic examination revealed areas of fibrosis with dilated, congested vessels and a dense lymphoplasmacytic infiltrate, without any evidence of bone necrosis (Figures 2A, B).
Histological and immunohistochemical analysis of the resected femoral head. (A) Hematoxylin and eosin staining showing areas of fibrosis with neoangiogenesis, vascular congestion, and dense lymphoplasmacytic inflammatory infiltrates, in the absence of bone necrosis (original magnification 100× and 200×). (B) Immunohistochemical staining demonstrating the immune infiltrate composition: CD20-positive B cells, CD3-positive T cells, with a predominance of CD4-positive over CD8-positive T lymphocytes.
Immunohistochemical staining confirmed the absence of melanoma metastasis (SOX10 negative) and ruled out other carcinomatous lesions (p40 and AE1/AE3 cytokeratin pool negative).
Samples from the acetabulum showed fibrous tissue partially covered by synovial lining, with prominent lymphocytic follicular aggregates and marked vascular congestion.
Postoperatively, a restaging CT scan performed in July 2024 confirmed the persistence of complete radiologic response in the chest, abdomen, and brain. Following hip replacement, the patient reported complete resolution of pain and resumed normal activities. She expressed gratitude for the combined oncological and surgical care, stating she ‘can now walk again without agony’.
At her latest follow-up in January 2025, the patient remained well, reporting complete resolution of symptoms, excellent functional recovery after hip arthroplasty, and ongoing complete response of her metastatic melanoma. Anti-PD-1 therapy has not yet been resumed.
Discussion
IrAEs are a recognized consequence of ICI therapy, stemming from immune hyperactivation and loss of self-tolerance. While a wide spectrum of organ systems can be involved, musculoskeletal irAEs are relatively uncommon and have been primarily characterized by inflammatory arthritis, myositis, or polymyalgia-like syndromes (4, 9, 10).
Direct immune-mediated injury targeting bone tissue, however, has not been previously reported.
Previous reports have described skeletal irAEs characterized by osteoporosis and resorptive bone lesions, often associated with systemic inflammatory features and inflammatory arthritis (11). Moreover, previous reports have also described and hypothesized immune-related osteonecrosis occurring during checkpoint inhibitor therapy. However, in these cases, true histological documentation was limited, and when available, findings were consistent with bone necrosis rather than active immune-mediated infiltration (5–8). Notably, no prior case reports have demonstrated dense lymphoplasmacytic infiltration replacing bone tissue in the femoral head without necrosis or tumor, as observed in our patient.
In this case, a patient with metastatic melanoma treated with combined CTLA-4 and PD-1 blockade developed progressive left hip pain, with imaging findings suggestive of osteonecrosis of the femoral head. Histopathological examination of the surgically resected femoral head, however, revealed a completely different pattern: the absence of bone necrosis, replaced by dense lymphoplasmacytic infiltration, fibrosis, and vascular congestion, without evidence of bone cell death or trabecular collapse.
This histological profile was highly suggestive of an active immune-mediated inflammatory process, an “osteitis “, rather than classical ischemic avascular necrosis (AVN).
Moreover, the patient had no known risk factors typically associated with AVN, such as chronic corticosteroid use, alcohol abuse, trauma, or hematologic conditions (12). The combination of clinical, radiological, and histopathological findings strongly supports the hypothesis of an immune-mediated mechanism triggered by checkpoint inhibition.
Beyond clinical presentation, important histopathological and pathophysiological differences distinguish AVN from the immune-mediated osteitis observed in our patient.
Classical AVN is characterized by ischemic bone infarction, leading to trabecular collapse, empty osteocytic lacunae, and eventual joint destruction, typically without significant inflammatory infiltration. In contrast, immune-mediated osteitis presents with preserved bone structure, dense lymphoplasmacytic infiltrates, neoangiogenesis, and active chronic inflammation without evidence of bone necrosis. These fundamental differences, summarized in Table 1, support the interpretation of this event as a novel skeletal irAE distinct from both classical AVN and medication-related osteonecrosis of the jaw (ONJ). In selected cases, ^99m^Tc-methylene diphosphonate (MDP) bone scintigraphy may provide additional diagnostic information. In fact, early AVN often presents as a photopenic (“cold”) lesion due to impaired blood supply, whereas immune-mediated osteitis is expected to show increased radiotracer uptake reflecting enhanced bone turnover. Although not performed in our patient, this modality could be considered when MRI findings are inconclusive, and its absence represents a limitation of our report.
One alternative hypothesis could be that of a solitary melanoma bone metastasis undergoing complete pathological response following immunotherapy. However, several elements argue against this possibility.
In fact, baseline staging scans revealed no evidence of skeletal involvement, and no other bone lesions were detected throughout follow-up. Histopathological analysis showed no residual neoplastic cells, confirmed by negative staining for melanoma markers (SOX10) and epithelial markers (p40, AE1/AE3).
Furthermore, in cases of complete pathological response of melanoma metastases, the expected histological findings would typically include fibrotic tissue and occasional melanosis - remnants of regressed tumor - but not an organized, dense, lymphoplasmacytic inflammatory infiltrate (13).
The presence of active, structured chronic inflammation, with follicular aggregates and vascular congestion, is much more consistent with an ongoing immunologic process than with scar tissue from tumor regression. Nonetheless, the possibility of an isolated melanoma metastasis undergoing complete immune-mediated regression cannot be completely ruled out. Given the broad spectrum of femoral head pathologies, we acknowledge that this inflammatory process could be unrelated to ICI therapy. However, the strong temporal association, absence of conventional risk factors, and distinctive histopathological features make an immune-mediated mechanism the most plausible explanation in this case.
This case highlights a previously unrecognized manifestation of checkpoint inhibitor toxicity, suggesting that bone tissue can be a direct target of immune-mediated inflammation (14). Recognition of this phenomenon is crucial because it may mimic more common conditions such as osteonecrosis but has a fundamentally different pathogenesis and implications for management.
To our knowledge, this is the first reported case of immune-mediated osteitis during ICI therapy. Although a causal link cannot be definitively proven and an unrelated etiology cannot be excluded, the temporal association, absence of conventional risk factors, and distinctive histopathological findings make an immune-mediated mechanism the most plausible explanation. Given the shared mechanism of action of ICIs, a class effect cannot be ruled out. Table 2 summarizes key features, differential diagnoses, and practical management considerations. Further research is needed to clarify its incidence, pathogenesis, and optimal management.
Conclusions
In conclusion, we describe what appears to be the first reported case of an immune-mediated osteitis involving the femoral head, likely induced by combined anti-CTLA-4 and anti-PD-1 therapy.
This adverse event may be significantly underdiagnosed or underreported, given that hip arthroplasty is a common procedure among elderly patients, including those with a history of cancer, and femoral heads are not routinely subjected to detailed histopathological analysis.
Recognition of such atypical immune-related events is crucial for improving our understanding of the full spectrum of skeletal toxicities associated with immune checkpoint inhibitors.
Further studies are warranted to elucidate the pathogenesis of this phenomenon and to define optimal strategies for diagnosis and management.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Boutros A Croce E Ferrari M Gili R Massaro G Marconcini R . The treatment of advanced melanoma: Current approaches and new challenges. Crit Rev Oncol Hematol. (2024) 196:104276. doi: 10.1016/j.critrevonc.2024.104276, PMID: 38295889 · doi ↗ · pubmed ↗
- 2Wolchok JD Chiarion-Sileni V Rutkowski P Cowey CL S Chadendorf D Wagstaff J . Final, 10-year outcomes with nivolumab plus ipilimumab in advanced melanoma. N Engl J Med. (2024) 392(1):11–22. doi: 10.1056/NEJ Moa 2407417, PMID: 39282897 PMC 12080919 · doi ↗ · pubmed ↗
- 3Long GV Carlino MS Mc Neil C Ribas A Gaudy-Marqueste C Schachter J . Pembrolizumab versus ipilimumab for advanced melanoma: 10-year follow-up of the phase III KEYNOTE-006 study. Ann Oncol Off J Eur Soc Med Oncol. (2024) 35:1191–9. doi: 10.1016/j.annonc.2024.08.2330, PMID: 39306585 · doi ↗ · pubmed ↗
- 4Haanen J Obeid M Spain L Carbonnel F Wang Y Robert C . Management of toxicities from immunotherapy: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol. (2022) 33:1217–38. doi: 10.1016/j.annonc.2022.10.001, PMID: 36270461 · doi ↗ · pubmed ↗
- 5Owosho AA Scordo M Yom SK Randazzo J Chapman PB Huryn JM . Osteonecrosis of the jaw a new complication related to ipilimumab. Oral Oncol. (2015) 51:e 100–1. doi: 10.1016/j.oraloncology.2015.08.014, PMID: 26421864 PMC 4784100 · doi ↗ · pubmed ↗
- 6Decaux J Magremanne M . Medication-related osteonecrosis of the jaw related to epacadostat and pembrolizumab. J Stomatol Oral Maxillofac Surg. (2020) 121:740–2. doi: 10.1016/j.jormas.2020.05.001, PMID: 32413422 · doi ↗ · pubmed ↗
- 7Pennings I Moskowitz A Shah G Estilo C Huryn JM Yom SK . Osteonecrosis of the jaw associated with pembrolizumab. Oral Surg Oral Med Oral Pathol Oral Radiol. (2023) 136:e 11–4. doi: 10.1016/j.oooo.2022.12.013, PMID: 36804060 PMC 10395506 · doi ↗ · pubmed ↗
- 8Patel V Carey B . Pembrolizumab related osteonecrosis of the jaw. Br J Oral Maxillofac Surg. (2023) 61:704–6. doi: 10.1016/j.bjoms.2023.08.241, PMID: 37957097 · doi ↗ · pubmed ↗