Active appendiceal bleeding recorded by choledochoscopy
Chenyang Jiao, Cuixia Liu, Yi Gao, Long Yang, Yiwei Fu

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
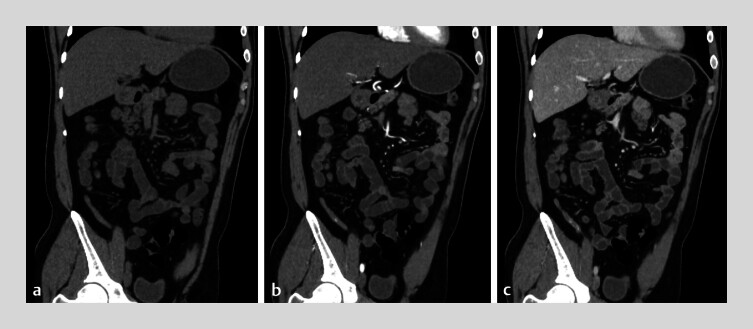 Fig. 1
Fig. 1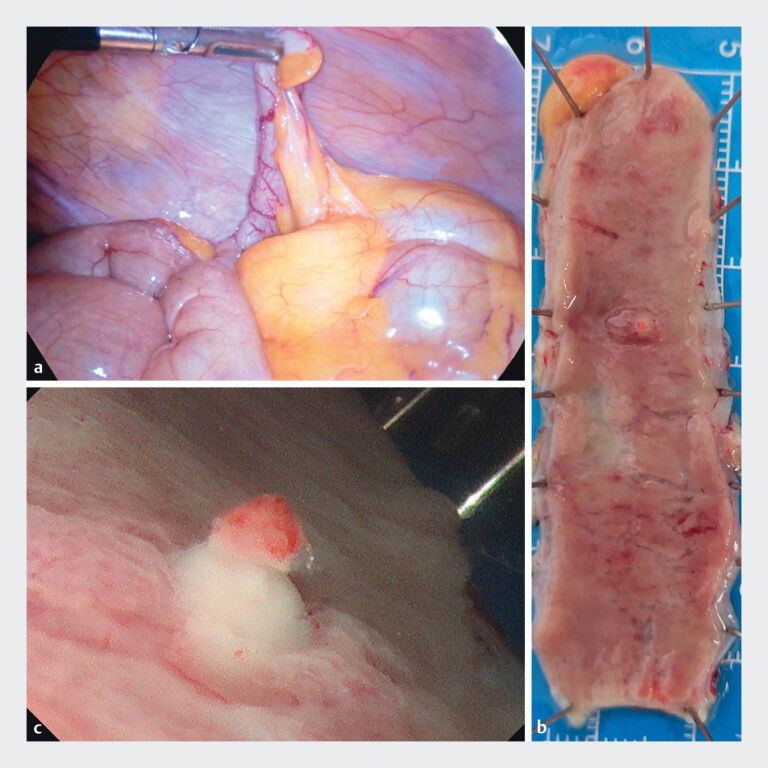 Fig. 2
Fig. 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Gastrointestinal Bleeding Diagnosis and Treatment · Appendicitis Diagnosis and Management
A 34-year-old man presented with painless hematochezia for 3 days. Colonoscopy performed at a secondary hospital was advanced to the terminal ileum, where a small amount of fresh blood was observed. The patient was initially diagnosed with small intestinal bleeding. On day 4 of illness, hematochezia persisted, and he was referred to our institution. Computed tomography angiography performed on admission, and no contrast medium was observed within the appendix on plain CT ( Fig. 1 a ); punctate contrast enhancement was noted during the arterial phase ( Fig. 1 b ), with further accumulation in the venous phase ( Fig. 1 c ). However, due to the extreme rarity of this finding, the intraluminal contrast within the appendix was not recognized during the initial image interpretation. On day 5, the patient continued to pass small amounts of bloody stool. On day 6, single-balloon enteroscopy was performed. On advancing the scope into the distal ileum, approximately 40 cm proximal to the ileocecal valve, yellowish intestinal fluid was encountered. Upon withdrawal to the cecum, active blood flow was observed emanating from the appendiceal orifice. A colonoscope was introduced into the cecum, and a choledochoscope was advanced through the biopsy channel. Bleeding from an appendiceal ulcer is not continuous but rather manifests as sporadic, pulsatile bleeding or oozing ( Video 1 ). Laparoscopic exploration revealed the appearance of the appendix is basically normal. Appendectomy was performed, and gross examination of the resected specimen demonstrated an ulcer located in the mid-portion of the appendix. Upon gross examination after appendiceal resection, an ulcer within the appendix was identified ( Fig. 2 ). The patient experienced no further bleeding after the surgery.
CT images of appendiceal hemorrhage. a CT plain scan of the appendix. b Arterial phase of the appendix. c Venous phase of the appendix.
CT scans and colonoscopy observed active bleeding in the appendix, and the insertion of a choledochoscopy into the appendiceal lumen revealed mucosal ulcers with active bleeding in the appendix.Video 1
Laparoscopic and postoperative images of the appendix. a Laparoscopic exploration of the appendix. b Mucosal ulcer of the appendix. c Close-up observation of the appendiceal ulcer.
Appendiceal hemorrhage is a rare condition, predominantly observed in males, typically presenting with painless hematochezia 1 2 3 . There have been reports of patients with recurrent unexplained gastrointestinal bleeding who underwent multiple endoscopic examinations without identifying the bleeding source, ultimately being diagnosed with appendiceal bleeding 4 . This case represents the first reported instance of active appendiceal bleeding diagnosed and documented via cholangioscopy, providing direct evidence for the confirmation of appendiceal bleeding. Bleeding from an appendiceal ulcer is not continuous but rather manifests as sporadic, pulsatile bleeding or oozing. Choledochoscopy has the potential to become the gold standard for diagnosing appendiceal bleeding.
Endoscopy_UCTN_Code_TTT_1AQ_2AZ
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Vesa TS Hosseini-Carroll P Manas K Diverticular hemorrhage of the appendix Gastroenterol Hepatol (N Y)20141039439525013394 PMC 4080878 · pubmed ↗
- 2Dung LT Hung ND Phuong LTH Appendiceal hemorrhage: An uncommon cause of lower gastrointestinal tract bleeding and intraluminal contrast extravasation Radiol Case Rep 2023182232223610.1016/j.radcr.2023.03.03537123041 PMC 10139855 · doi ↗ · pubmed ↗
- 3Takahashi M Sawada T Fukuda T Complete appendiceal intussusception induced by primary appendiceal adenocarcinoma in tubular adenoma: a case report Jpn J Clin Oncol 20033341341510.1093/jjco/hyg 07614523063 · doi ↗ · pubmed ↗
- 4Xing XC Yang JL Xiao X Clinical features, treatments and prognosis of appendiceal bleeding: a case series study BMC Gastroenterol 20232337710.1186/s 12876-023-03025-637924017 PMC 10625278 · doi ↗ · pubmed ↗