A self-made wire snare used in combination with a long transparent cap to remove an obstructive sigmoid fecalith
Ke Liu, Yulin Cheng, Lizhi Yi, Zhengyu Cheng, Huarong Qiu, Zhaojin Yang, Xianfei Zhong

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
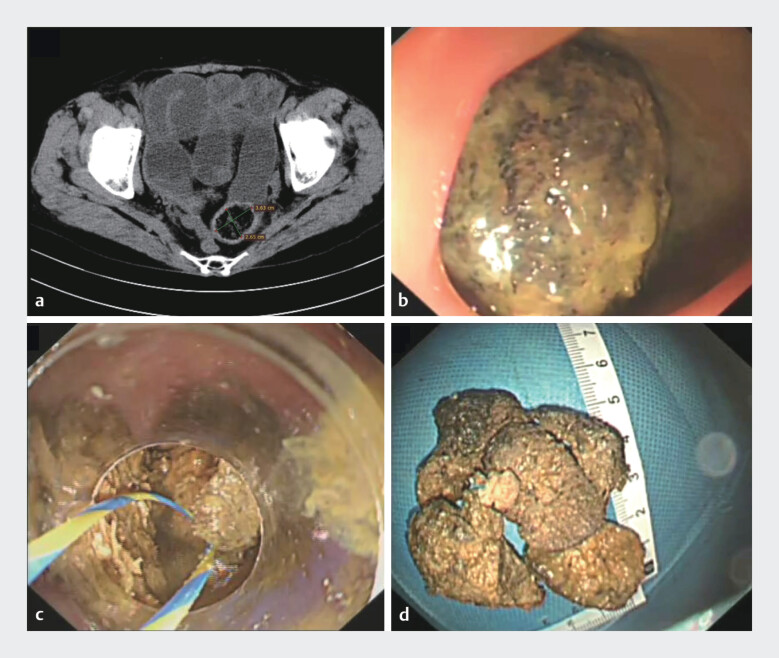 Fig. 1
Fig. 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsForeign Body Medical Cases · Gallbladder and Bile Duct Disorders · Esophageal and GI Pathology
A 68-year-old female was admitted to our hospital with a 5-day history of abdominal pain and vomiting. Computed tomography revealed a mixed-density mass measuring 3.63 cm × 2.65 cm in the sigmoid colon, containing sieve-like low-density areas, along with proximal colonic dilation and fluid accumulation, which are consistent with the presence of a sigmoid colonic fecalith accompanied by colonic obstruction ( Fig. 1 a ). The patient chose to undergo endoscopic intervention. Colonoscopy revealed a large black-brown fecalith situated in the sigmoid colon, resulting in complete luminal occlusion and preventing further advancement of the endoscope ( Fig. 1 b ). An initial attempt was made to remove the fecalith using a conventional snare; however, the procedure was unsuccessful due to the relatively large size and hardened consistency of the fecalith. Subsequently, a self-made snare fabricated from a zebra guidewire and integrated with a long transparent cap was utilized ( Video 1 ). The fecalith was successfully fragmented, and all resulting fragments were completely removed ( Fig. 1 c, d ). No postoperative bleeding or perforation was observed, and the patientʼs abdominal pain significantly improved. She resumed spontaneous bowel movements and was discharged on the second postoperative day.
a Computed tomography revealed a mixed-density mass measuring 3.63 cm × 2.65 cm in the sigmoid colon. b Colonoscopy revealed a large black-brown fecalith situated in the sigmoid colon. c A self-made snare fabricated from a zebra guidewire and integrated with a long transparent cap was utilized to remove the fecalith. d The fecalith was successfully fragmented, and all resulting fragments were completely removed.
A self-made wire snare used in combination with a long transparent cap to remove an obstructive sigmoid fecalith.Video 1
Fecalith-induced colonic obstruction is not uncommon. However, endoscopic management of fecaliths remains challenging due to their typically large size and hard consistency 1 . Although the combination of a self-made wire snare and a long transparent cap has been reported to be effective in the treatment of giant phytobezoars 2 , its application in the management of colonic fecaliths has not been previously documented. Compared with the stomach, the colon provides a more limited working space, particularly in cases of obstruction where endoscopic visualization is impaired. Our case demonstrates that a self-made snare incorporating a long transparent cap can effectively remove the obstructive sigmoid colonic fecalith.
Endoscopy_UCTN_Code_TTT_1AQ_2AH
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Yang D Wang X Tao K Endoscopic fenestration combined with catheterization in the treatment of a giant colonic fecalith causing bowel obstruction: a case report. Endoskopische Fenestration in Kombination mit Katheterisierung bei der Behandlung eines riesigen Kolonfäkalits, der einen Darmverschluss verursacht: Ein Fallbericht Z Gastroenterol 20236168068210.1055/a-1973-555436470287 PMC 10581091 · doi ↗ · pubmed ↗
- 2Yi L Qiu H Liu KA self-made wire snare used in combination with a long transparent cap to remove a giant phytobezoar Endoscopy 20245601 E 1065 E 106610.1055/a-2471-786139626785 PMC 11614571 · doi ↗ · pubmed ↗