Endoscopic ultrasound-guided enterocolostomy for small bowel obstruction following radical cystectomy with ileal neobladder reconstruction
Ting Wen, Xiaoming Wang

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Fig. 1
Fig. 1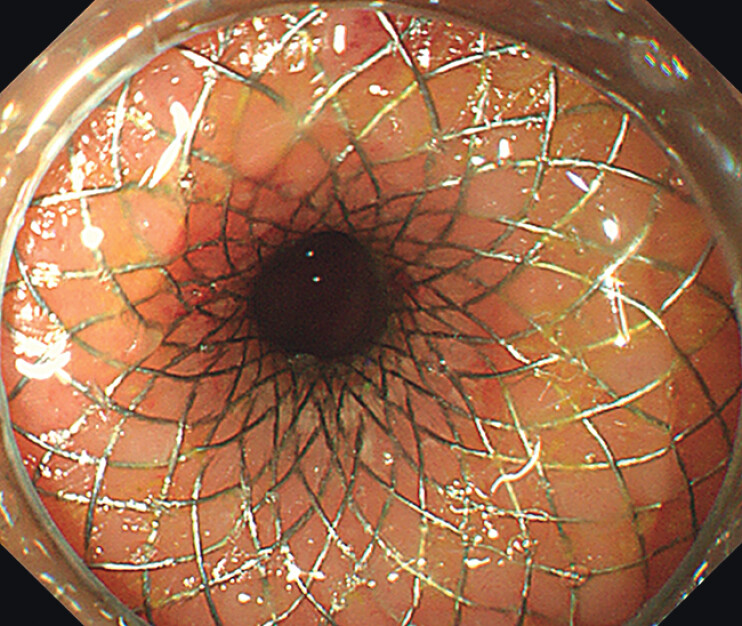 Fig. 2
Fig. 2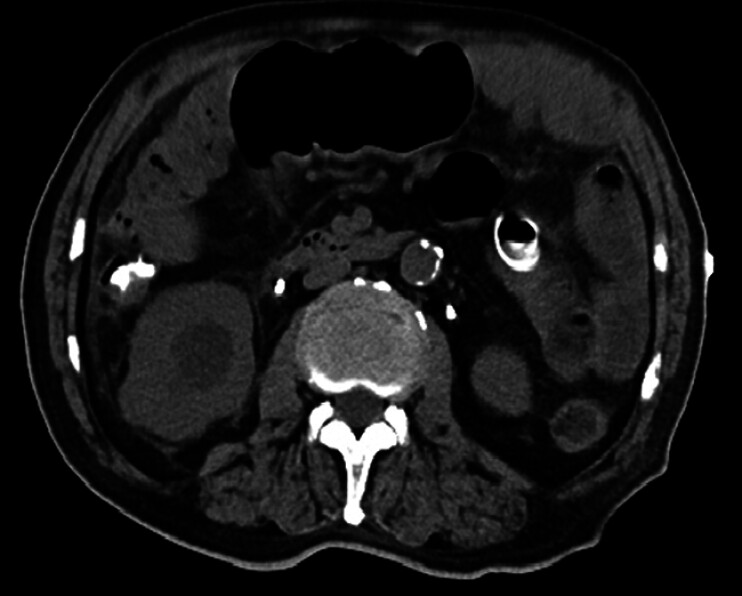 Fig. 3
Fig. 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBladder and Urothelial Cancer Treatments · Intestinal and Peritoneal Adhesions · Intraperitoneal and Appendiceal Malignancies
A 77-year-old male, who was previously diagnosed with bladder cancer, underwent radical cstyectomy and ileal neobladder reconstruction. The abdominal computed tomography (CT) imaging revealed incomplete small bowel obstruction ( Fig. 1 ).
The abdominal CT imaging revealed incomplete small bowel obstruction. CT, computed tomography.
Given the patient’s cachectic state, the endoscopic ultrasound-guided enterocolostomy (EUS-EC) with a lumen-apposing metal stent (LAMS) for palliation of small-bowel obstruction was chosen ( Video 1 ). A guidewire was placed in the intestinal lumen via colonoscopy, and an ultrasound colonoscope was inserted along the guidewire. The puncture site was determined where the distance between the sigmoid colon and the dilated plane above the small intestinal obstruction was less than 1 cm. A 19-G needle was used to puncture the dilated intestinal lumen from the localization point, and the intestinal fluid was visible in the retraction, which was reconfirmed by iodinohydrol contrast as a dilated small bowel. A 15 mm × 10 mm LAMS was placed using the 150-W pure-cut mode ( Fig. 2 ).
Endoscopic ultrasound-guided enterocolostomy with LAMS for palliation of small-bowel obstruction. LAMS, lumen-apposing metal stent.Video 1
The LAMS was placed Successfully through EUS-EC. LAMS, lumen-apposing metal stent.
A follow-up abdominal CT imaging on the second postoperative day showed that the small bowel obstruction was significantly reduced compared with the previous one ( Fig. 3 ). The patient’s abdominal pain and bloating were significantly relieved. He was able to take oral nutritional supplements, and was gradually transitioning to a liquid diet.
The follow-up abdominal CT imaging showed that the small bowel obstruction was significantly reduced. CT, computed tomography.
There are already relevant literature reports on common bile duct-duodenal anastomosis for obstructive distal common bile duct, gastrointestinal anastomosis for gastric outlet obstruction, and jejunojejunostomy for bypass surgery-induced stenosis 1 2 3 . This is the first instance of small bowel obstruction following radical cystectomy and ileal neobladder reconstruction treated with EUS-EC. This case confirms the feasibility of EUS-EC treatment for small bowel obstruction, but caution should be exercised when selecting the puncture site.
Endoscopy_UCTN_Code_TTT_1AS_2AG
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1French JB Coe AW Pawa R Endoscopic ultrasound-guided choledochoduode-nostomy with a lumen-apposing, self-expandable fully covered metal stent for palliative biliary drainage Clin J Gastroenterol 20169798510.1007/s 12328-016-0634-y 26956721 · doi ↗ · pubmed ↗
- 2Khashab MA Kumbhari V Grimm ISEUS-guided gastroenterostomy: the first U.S. clinical experience (with video)Gastrointestinal Endoscopy 20158293293810.1016/j.gie.2015.06.01726215646 · doi ↗ · pubmed ↗
- 3Majmudar K Wagh MSEUS-guided jejuno-jejunostomy with lumen-apposing metal stent for complete jejunal obstruction after gastric bypass Gastrointestinal Endoscopy 20168485385410.1016/j.gie.2016.06.00727307302 · doi ↗ · pubmed ↗