Red flags for thoracic endometriosis
Lorenzo Carriera, Roberto Lipsi, Angelo Coppola

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
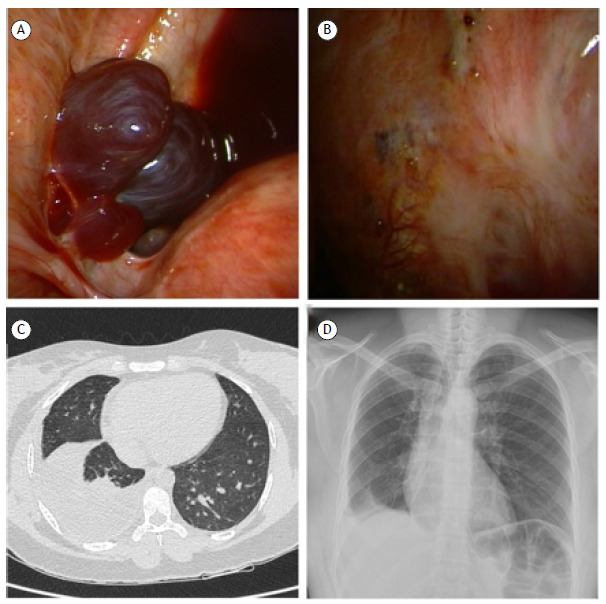 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEndometriosis Research and Treatment · Omental and Epiploic Conditions · Uterine Myomas and Treatments
A 38-year-old Brazilian woman with a previous diagnosis of pelvic inflammatory disease presented to our hospital with a two-month history of dyspnea, chest pain, and dry cough. Chest CT revealed right-sided basal pleural effusion. The QuantiFERON-TB test result was positive. On the basis of those findings and the symptoms, we suspected a diagnosis of pleural tuberculosis. An explorative thoracentesis was performed. The aspirated pleural fluid was hemorrhagic. The cytological examination showed a predominance of histiocytes and leukocytes, and no malignant cells were detected. At that point, we decided to perform medical thoracoscopy to obtain biopsy specimens from the parietal pleura. The procedure revealed thickened pleura and small, wine-red lesions on the diaphragm and parietal pleura (Figure 1), findings suggestive of pleural endometriosis. Histopathological analysis confirmed the presence of epithelial glandular elements, and immunohistochemical staining was positive for CD10 and estrogen receptors. Thoracic endometriosis presents nonspecific symptoms, making the diagnosis challenging. In women of reproductive age presenting with chest pain and pleural effusion, endometriosis should be considered as a possible cause.1 Hormone suppression therapy with gonadotropin-releasing hormone analogs can help alleviate symptoms as well as improving the overall quality of life and daily functioning.2 Early recognition and multidisciplinary care are key to achieving better outcomes.3
Figure 1A) Wine-red nodules on the diaphragm visualized during medical thoracoscopy; B) Small punctiform wine-red lesions on the parietal pleura; C) Chest CT at admission, showing right-sided basal pleural effusion; D) Chest X-ray 1 month after the initiation of gonadotropin-releasing hormone therapy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Nezhat C Lindheim SR Backhus L Vu M Vang N Nezhat A Thoracic Endometriosis Syndrome A Review of Diagnosis and Management JSLS 2019233 e 201910.4293/JSLS.2019.00029 PMC 668433831427853 · doi ↗ · pubmed ↗
- 2Ciriaco P Muriana P Lembo R Carretta A Negri G Treatment of Thoracic Endometriosis Syndrome A Meta-Analysis and Review Ann Thorac Surg 2022113132433610.1016/j.athoracsur.2020.09.06433345783 · doi ↗ · pubmed ↗
- 3Nezhat C Amirlatifi N Najmi Z Tsuei A Thoracic Endometriosis Syndrome A Comprehensive Review and Multidisciplinary Approach to Management J Clin Med 202413247602760210.3390/jcm 1324760239768527 PMC 11678721 · doi ↗ · pubmed ↗