Neonatal Brucellosis in an Extremely Preterm Infant: A Fatal Case Report
Muhammad Takhman, Orabi Hajjeh, Moath Hattab, Reem Shihab, Hadeel Atout, Rabee Adwan, Mamoun A. T. Ibaideya

TL;DR
A preterm infant died from congenital brucellosis, highlighting the difficulty in diagnosing and treating this rare neonatal infection.
Contribution
This case report adds to the limited literature on fatal congenital brucellosis in extremely preterm infants.
Findings
Congenital brucellosis can present with symptoms similar to neonatal sepsis, leading to delayed diagnosis.
Despite antimicrobial therapy, the infant succumbed to multiple organ failure due to complications of brucellosis.
Early recognition and targeted treatment are critical for improving outcomes in neonatal brucellosis.
Abstract
Brucellosis is a globally significant zoonotic disease, but congenital brucellosis remains exceedingly rare. It is primarily transmitted transplacentally from an infected mother to the fetus, often presenting with nonspecific signs that mimic neonatal sepsis. The condition poses diagnostic and therapeutic challenges, particularly in endemic regions where early identification is crucial to improving neonatal outcomes. We report the case of a 19-year-old gravida 1, para 0 female with a history of treated Brucella infection at 12 weeks of gestation. She experienced preterm premature rupture of membranes (PPROM) at 24 weeks and 2 days and delivered a female infant via spontaneous vaginal delivery. The neonate, weighing 725 g at birth, presented with cyanosis, respiratory distress, and unstable vital signs. Initial workup suggested early onset sepsis, prompting empirical antibiotic therapy.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1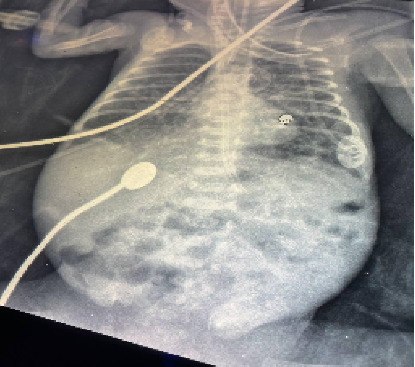 Figure 2
Figure 2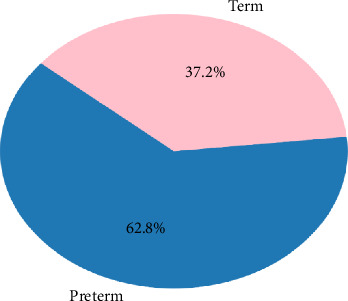 Figure 3
Figure 3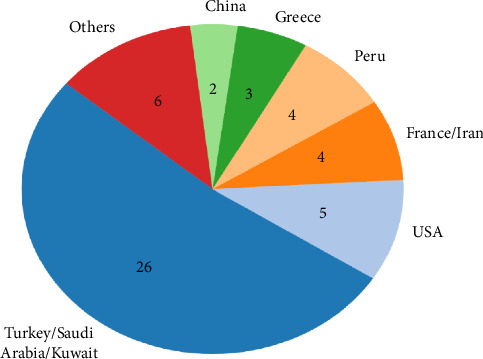 Figure 4
Figure 4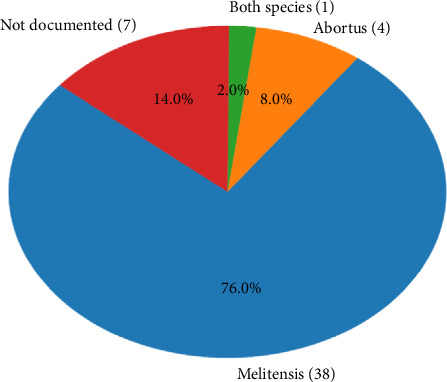 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBrucella: diagnosis, epidemiology, treatment · Zoonotic diseases and public health · Animal Diversity and Health Studies
1. Case Presentation
A 19-year-old asymptomatic gravida 1, para 0, female experienced preterm premature rupture of the membranes (PPROM) at 24 weeks and two days of gestation and was admitted to hospital. The pregnancy was uneventful except for documented Brucella infection at 12 weeks of gestation and prescribed a 6-week course of antibiotics consisting of a combination of doxycycline and rifampin. However, the patient was noncompliant and discontinued the medications after a short period, without completing the full course or attending follow-up. The pregnancy was uneventful except for documented Brucella infection at 12 weeks' gestation treated with a 6-week course of antibiotics with no complaint. She delivered a female infant by spontaneous vaginal delivery. The infant had cyanosis on initial presentation along with irregular breathing, Apgar scores at birth were 6 and 8, after 1 and 5 min, respectively. So, the infant had to be intubated and transferred to the neonatal intensive care unit (NICU) for further management (Figure1). On initial examination, the patient had weight, 725 g; head circumference, 26 cm; length, 38 cm; and unstable vital signs. The patient was connected to mechanical ventilation on synchronized intermittent mandatory ventilation (SIMV) mode, first dose of surfactant was given, and she was on paracetamol and caffeine for apnea prophylaxis. Blood specimens for cultures were obtained, then the neonate was treated empirically with ampicillin (18 mg intravenous [IV] every 12 h) and gentamicin (3.5 mg IV every 48 h) as a result of early onset of sepsis suspicion. Blood tests were significant for high C-reactive protein. Complete blood count (CBC) and random blood sugar were normal. On Day 5, the patient's white blood cell (WBC) count was elevated to 42 × 10^9^/L, prompting an upgrade in antibiotics to piperacillin/tazobactam (35 mg IV every 12 h) and amikacin (5 mg IV every 24 h), to provide broader Gram-negative and anaerobic coverage.
Echocardiography was done for the patient and was free apart from small patent foramen ovale. On Day 7, blood cultures revealed the presence of Brucella. The father confirmed a maternal history of treated Brucella infection before 3 months of delivery. The mother was advised to avoid breastfeeding the baby. Targeted therapy for brucellosis was initiated by adding rifampicin (14.5 mg orally every 24 h) and gentamicin (3 mg IV every 36 h) to the existing antibiotic regimen, while amikacin was discontinued to minimize aminoglycoside toxicity and avoid redundancy in coverage. It is important to note that the first blood culture, taken from the baby on Day 1, was conducted before breastfeeding began and prior to the administration of any antibiotics. Test results revealed the following: blood culture showed growth of Brucella melitensis (titer 1/320) and Brucella abortus (titer 1/320). The maternal Brucella IgM titer was 41 (normal value: < 11), while the baby's IgM titer was 3. The low Brucella IgM titer in the infant is consistent with the known limitations of serological testing in neonates, particularly in extremely preterm infants who may have an underdeveloped immune response. Despite the low IgM, blood cultures confirmed active infection, which remains the gold standard for diagnosis [1].
On Day 11, the patient had intraventricular hemorrhage (IVH) grade III detected on transfontanelle ultrasound (TFU) and persisted throughout his course. The day after, feeding was withheld due to vomiting and abdominal distension that was later revealed to be necrotizing enterocolitis (Figure 2). During the patient course, she had seven blood transfusions for anemia, and she also had many changes in her antimicrobial drug following elevation in inflammatory markers multiple time for sepsis of bacterial and fungal sources. On Day 38, the patient had cardiac arrest but was resuscitated and started in dopamine infusion, perforated necrotizing enterocolitis was detected on x-ray, and intra-abdominal drain was applied. On the next day, she had another arrest but she was resuscitated after 2 cycles and calcium gluconate infusion. Tragically, she suffered another cardiac arrest, and despite administering three dopamine boluses, resuscitation efforts were unsuccessful. The patient was pronounced dead.
2. Introduction
Brucellosis, a common worldwide zoonotic infection, transmitted form animals to humans through contact with infected animals or contaminated animal product. Congenital brucellosis on the other hand is extremely rare and occurs through transplacental transmission from the mother to the fetus. Congenital brucellosis represents a diagnostic challenge especially in the endemic areas, as the clinical manifestations are usually nonspecific mirroring a sepsis-like picture pointing out the importance of detailed history of the maternal history of ingesting unpasteurized milk or contact with animals.
Here, we present the case of a 24-week-old infant with respiratory distress and a sepsis-like presentation, ultimately diagnosed with congenital brucellosis through blood culture.
3. Discussion
Congenital brucellosis is an invisible threat, especially in brucellosis-endemic areas where Brucella species are transferred from infected mothers to unborn children through transplacental transmission with deadly consequences including spontaneous abortions, intrauterine fetal deaths, and prematurity (Figure 3) [2].
Although pregnant women in endemic regions (Figure 4) are at risk of Brucella exposure, congenital brucellosis remains an exceptionally rare condition, with only 44 cases reported globally up to 2017 [2]. A search of subsequent publications revealed 7 additional cases reported since then, making this the 51st case (Table 1). The transmission mechanisms, clinical manifestations, and long-term outcomes associated with congenital brucellosis remain underexplored in the current literature.
Congenital brucellosis is thought to occur through transplacental transmission from a bacteremic mother or through exposure to maternal blood, urine, or genital secretions during delivery. Half of the reported cases were bacteremic at birth, supporting transplacental transmission as a likely mechanism [2]. While Brucella transmission via breast milk and blood transfusion has been documented in the literature [10, 11], our patient's positive blood culture, with the absence of breastfeeding or transfusion, points strongly to transplacental transmission as the probable route. While the clinical course and eventual outcome in our case were likely driven by the complications of extreme prematurity, the potential role of maternal Brucella infection in precipitating PPROM and subsequent preterm delivery cannot be overlooked. Several studies have identified an association between maternal brucellosis and adverse obstetric outcomes, including spontaneous abortion, intrauterine fetal demise, and preterm birth [2, 12, 13]. In this case, the incomplete treatment and absence of follow-up may have contributed to persistent bacteremia, thereby increasing the risk of vertical transmission and possibly triggering premature labor. However, due to the lack of placental histopathology or maternal serologic follow-up, a definitive causal link cannot be established.
The clinical presentation of congenital brucellosis is nonspecific, frequently manifesting as premature rupture of membranes, respiratory distress, or a sepsis-like picture with hepatosplenomegaly or jaundice as a common exam finding. Less common presentations, including myocarditis and hydrocephalus, have also been documented. These varied manifestations underscore the importance of a high index of suspicion among clinicians, especially in endemic regions or when there is a maternal history of ingesting unpasteurized milk or contact with animals. Recognizing these risk factors early can aid in early diagnosis and management [12, 13]. Noncompliance with the prescribed antibiotic regimen during pregnancy, as seen in our case, may contribute to persistent maternal bacteremia and increase the risk of vertical transmission. This highlights the importance of thorough counseling, close monitoring, and follow-up in pregnant women diagnosed with brucellosis, especially in endemic areas.
Diagnosis of neonatal brucellosis depends primarily on positive blood cultures that isolate the Brucella organism, most commonly Brucella meltinesis (Figure 5), although serological tests showing elevated or rising antibody titers in either the mother or neonate and history of exposure to livestock or ingesting raw milk can also provide important diagnostic clues. In rare cases, Brucella has been recovered from blood cultures of children who have negative or insignificant antibody titers (< 1:160), making bacteremia a more reliable indicator of infection. Serological tests (serum agglutination test) are helpful in diagnosing and monitoring the disease, and titers of 1:160 or higher are significant. However, the value of these tests is low because bacteremia provides unequivocal evidence of infection. Nevertheless, the diagnosis by microbiology is delayed as Brucella grows slowly. In this context, prompt identification and early antibiotic treatment will lower the risk of serious complication, which highlights the need of knowing clinical features of neonatal brucellosis for appropriate management [1, 12, 14]. Other rapid diagnostic techniques, such as polymerase chain reaction (PCR), are emerging as valuable tools, offering improved sensitivity and faster results [15].
A treatment approach of intravenous aminoglycosides for 5–14 days with oral rifampicin and trimethoprim/sulfamethoxazole (TMP/SMX) for 6 weeks is commonly reported in literature review as a treatment for congenital brucellosis [12]. Not to forget the relative contraindication of TMP/SMX in children less than 2 months of age as it displaces indirect bilirubin from albumin, increasing the risk of jaundice and subsequent kernicterus highlighted in multiple studies.
New update in treatment for pediatric brucellosis depends on the age: where oral doxycycline and rifampicin are used for children above the age of 8. On the other hand, for those under 8 years old, a combination of oral trimethoprim, sulfamethoxazole, and rifampicin of a 6–8-week duration is advised [4]. The varying success rates of different brucellosis treatment approaches highlight the need for further research into optimal therapies for neonates. Additionally, the high recurrence rates, which can be partially attributed to incomplete eradication of the infection or reinfection through breast milk, along with the risk of complications, emphasize the importance of long-term follow-up for affected infants.
From a public health perspective, eradicating congenital brucellosis should be done through prevention and treatment. Antenatal screening in high-risk populations could facilitate early identification and management of maternal brucellosis, reducing the risk of congenital transmission. The information and awareness campaigns in the countries that suffer brucellosis should inform people on the dangers of eating unprocessed animal milk and contact with animals, as the majority of infected pregnant women reported a history of unpasteurized milk consumption or contact with animals [12]. Furthermore, improving the diagnostic methods in low-resourced areas with the use of PCR, e.g., or other rapid diagnostic measures may lead to earlier diagnosis and treatment, which would improve the health of the neonate.
In conclusion, congenital brucellosis is an extremely rare condition posing serious challenges in diagnosis, treatment, and follow-up to ensure complete eradication of the infection. Crucial efforts to implement preventative strategies and raise awareness among people and healthcare practitioners are required to minimize the disease's burden. Finally, a multidisciplinary approach that combines public health activities with clinical care will be critical to improve outcomes for afflicted newborns.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mosayebi Z. Movahedian A. H. Ghayomi A. Kazemi B. Congenital Brucellosis in a Preterm Neonate Indian Pediatrics 200542659960115995277 · pubmed ↗
- 2Alsaif M. Dabelah K. Featherstone R. Robinson J. L. Consequences of Brucellosis Infection During Pregnancy: A Systematic Review of the Literature International Journal of Infectious Diseases 201873182610.1016/j.ijid.2018.05.0232-s 2.0-8504875782729885371 · doi ↗ · pubmed ↗
- 3Xu D. Li X. Cheng B. Congenital Brucellosis: A Case Report Vector Borne and Zoonotic Diseases 202121972773010.1089/vbz.2021.001534534025 · doi ↗ · pubmed ↗
- 4Mohzari Y. A. Alshuraim R. A. Asdaq S. M. B. Congenital Brucellosis: A Case Report Journal of International Medical Research 20204812 p. 030006052097557610.1177/0300060520975576 PMC 772706433290133 · doi ↗ · pubmed ↗
- 5Al-Ayyadhi N. H. Al-Awadhi S. S. Al-Shammari F. J. Hassan H. A. A Rare Congenital Brucellosis Re-Emerging in Kuwait: A Case Report 2023 https://www.gavinpublishers.com/article/view/a-rare-congenital-brucellosis-re-emerging-in-kuwait-a-case-report
- 6Al-Faifi J. Ibrahim M. E. Congenital Brucellosis Associated With Subsequent Klebsiella pneumoniae Co-Infection in a Premature Neonate: A Rare Case Report Journal of Infection and Public Health 202215558658810.1016/j.jiph.2022.04.00935500542 · doi ↗ · pubmed ↗
- 7Zhao M. Huang F. Zhang A. Congenital Brucellosis in a Chinese Preterm Neonate: A Case Report Journal of International Medical Research 20194752296230110.1177/03000605198389212-s 2.0-8506616369130971153 PMC 6567740 · doi ↗ · pubmed ↗
- 8YetmişE. Congenital Brucellos in a Premature Infant http://hnhtipdergisi.com/jvi.aspx?un=HNHJ-78055