Effect of radioiodine treatment for Graves’ disease on the generation of TSH anti-receptor stimulating antibodies (TSI)
Lia B. Fiorin, Teresa S. Kasamatsu, Cléber P. Camacho, Gilberto K. Furuzawa, Melissa Furlaneto, Mario Luiz V. Castiglioni, Luiza K. Matsumura, Reinaldo P. Furlanetto, Marcelo C. Batista, Rui M. B. Maciel, Carlos E. S. Ferreira, Carolina C. P. S. Janovsky, João Roberto M. Martins

TL;DR
Radioiodine treatment for Graves' disease increases TSI levels, which can stay high for over a year in many patients, affecting treatment and management decisions.
Contribution
This study shows that TSI levels rise after radioiodine therapy and remain elevated in over half of patients for up to 12 months.
Findings
TSI levels increased in 72% of patients after radioiodine therapy.
TSI remained higher than baseline in 58% of patients at 12 months.
Persistent TSI was more common in patients with thyroid eye disease, longer disease duration, or higher baseline TSI.
Abstract
It is well established that serum levels of TSH receptor antibodies (TRAb) rise after radioiodine (131I) therapy for Graves’ disease (GD). However, it remains unclear whether these post-therapy autoantibodies are predominantly TSH receptorstimulating immunoglobulins (TSI) and how their persistence might affect treatment outcomes. In this prospective study, 39 patients with GD underwent 131I therapy. Serum TRAb (measured by competitive electrochemiluminescence, ECLIA) and TSI (measured by an IMMULITE® 2000/2000 XPi TSI assay) were evaluated at baseline and at 1, 2, 3, 6, 9, and 12 months post-therapy. More than 7% increase from baseline was considered a significant rise. At diagnosis, all 39 patients tested positive for TRAb, while 38 tested positive for TSI. Both TRAb and TSI levels rose significantly between months 2 and 4 post-131I, followed by a progressive decline by months 9 to…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
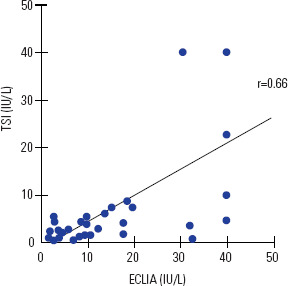 Figure 1
Figure 1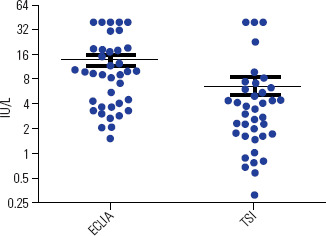 Figure 2
Figure 2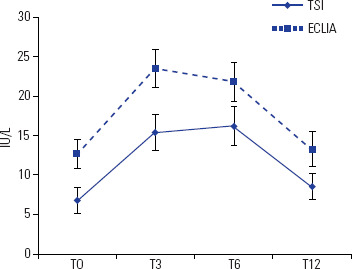 Figure 3
Figure 3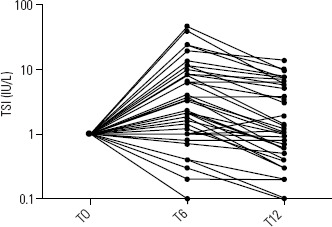 Figure 4
Figure 4| Parameters | |
|---|---|
| Age (years-old) | 39.6 ± 15.1 |
| Gender (F:M) | 30:9 |
| Time of diagnosis (years) | 3.1 ± 1.9 |
| Smoking (yes/no) | 9/30 |
| Dose of radioiodine (mCi) | 16.3 ± 3.6 |
| Presence of TED (yes/no) | 33/6 |
| Thyroid volume (mL) | 41.6 ± 28.7 |
| TSH (mIU/L) | 0.48 ± 1.99 |
| Free T4 (ng/dL) | 5.4 ± 1.7 |
| Total T3 (ng/mL) | 346.0 ± 234.75 |
| ATG (IU/mL) | 218.1 ± 326.2 |
| ATPO (IU/mL) | 503.4 ± 194.5 |
| TRAb (IU/L) | 14.3 ± 13.1 |
| TSI (IU/L) | 24.9 ± 18.2 |
| TSI increased N = 28 | TSI did not increase N = 11 | p | |
|---|---|---|---|
| Gender | |||
| F/M | 20/8 | 10/1 | 0.4 |
| TED (yes/no) | 26/2 | 7/4 | 0.04 |
| Smoking (yes/no) | 6/22 | 3/8 | 0.69 |
| Resolution of hyperthyroidism (yes/no) | 24/4 | 10/1 | 1.0 |
| Positivity of ATPO (yes/no) | 21/7 | 8/3 | 1.0 |
| Positivity of ATG (yes/no) | 16/12 | 7/4 | 1.0 |
| Thyroid volume (mL) | 34.5 ± 26.3 | 28.5 ± 19.8 | 0.65 |
| Radioiodine (mCi) | 16.4 ± 3.8 | 15.9 ± 3.0 | 0.85 |
| TSH (mIU/L) | 0.09 ± 0.17 | 1.47 ± 3.67 | 0.15 |
| Total T3 (ng/mL) | 344.7 ± 239.5 | 349.4 ± 233.4 | 0.98 |
| Free T4L (ng/dL) | 3.1 ± 1.8 | 3.3 ± 2.2 | 0.95 |
| TSI (IU/L) | 3.2 ± 2.1 | 13.4 ± 14.8 | 0.06 |
| Initial TSI (Positive/Negative) | 28/0 | 10/1 | 1.0 |
| ECLIA (IU/L) | 10.8 ± 8.9 | 21.8 ± 16.8 | 0.13 |
| Age (years-old) | 38.2 ± 15.6 | 43.3 ± 13.5 | 0.20 |
| Time of GD (years) | 3.4 ± 2.1 | 2.0 ± 1.0 | 0.03 |
| ATPO (IU/mL) | 296.3 ± 252.4 | 243.0 ± 228.7 | 0.52 |
| ATG (IU/mL) | 241.8 ± 361.5 | 99.8 ± 127.8 | 0.52 |
- —Coordenação de Aperfeiçoamento de Pessoal de Nível Superior-Brasil
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsThyroid Disorders and Treatments · Thyroid Cancer Diagnosis and Treatment · Ophthalmology and Eye Disorders
INTRODUCTION
Graves’ disease (GD) is an autoimmune thyroid disorder characterized by TSH receptor antibodies (TRAb), which stimulate the TSH receptor and drive hyperthyroidism (^1,2^). Because TRAb are functionally heterogeneous, they may include stimulatory immunoglobulins (TSI), blocking immunoglobulins (TBII), or neutral antibodies (^3-6^). When TSI predominate, they activate adenylate cyclase, causing thyroid hyperfunction (^6,7^).
Radioiodine (^131^I) therapy is a common definitive treatment for GD (^8-11^). Its beta radiation destroys thyroid cells (actinic thyroiditis), triggering a surge in thyroid antigens and often raising levels of autoantibodies such as TRAb (^8,11-13^). TRAb levels typically peak around three months post-treatment and gradually decline, sometimes remaining elevated for five years or longer (^14^). The specific role of TSI within this antibody surge and the implications of persistent TSI levels remain uncertain.
Measurement of TRAb aids in diagnosing GD, predicting relapse of thyrotoxicosis, and guiding therapy (^2,7,15,16^). During pregnancy, assessing TRAb can distinguish GD from gestational hyperthyroidism, guide antithyroid medication choices, and evaluate the risk of fetal or neonatal hyperthyroidism (^15,17^). Conventional TRAb assays (e.g., ECLIA) detect total TSH receptor–binding immunoglobulins, while newer TSI assays measure only stimulatory antibodies (^18^).
Growing evidence indicates that TRAb – even many years after ^131^I therapy – can remain significantly elevated in some patients, including during pregnancy (^19-21^). For instance, very high maternal TRAb levels have been shown to predict neonatal hyperthyroidism or adverse pregnancy outcomes (^21,22^), with one study demonstrating that neonatal thyroid dysfunction occurs in ~5.5% of newborns of mothers who conceived within two years of ^131^I therapy (^23^). Moreover, several case reports highlight that TRAb titers can rise unexpectedly in the late second or even third trimester, sometimes leading to neonatal hyperthyroidism despite stable or low maternal thyroid hormone levels (^21,24^). These observations reinforce the importance of measuring TRAb (and ideally TSI, when available) in women with GD – particularly those with a history of radioiodine therapy – who are planning pregnancy or are already pregnant.
This study evaluated the post-^131^I behavior of both conventional TRAb and TSI in patients with GD, with special attention to whether persistent post-therapy TRAb reflect primarily stimulatory activity. We also discuss the clinical implications of persistent TSI, particularly in women of reproductive age and in patients with thyroid eye disease (TED).
SUBJECTS AND METHODS
Study population
We prospectively evaluated 39 consecutive patients (age range 18-70 years) with a clinical and biochemical diagnosis of GD who were referred for ^131^I therapy at our institution. The diagnosis was confirmed by clinical signs/symptoms of hyperthyroidism, diffuse goiter (with or without TED), suppressed TSH, and elevated free T4. TED was assessed using clinical score and NOSPECS and imaging techniques (ultrasound and MRI). None of the patients showed inflammatory activity at the initial presentation, and none of them received corticosteroid prophylaxis before radioiodine therapy. Patients received 10-30 mCi of ^131^I based on disease severity, thyroid size, and comorbidities. Patients received a dose of radioactive iodine due to the failure of medication treatment. All patients were referred to our service at least one and a half years after diagnosis and still in thyrotoxicosis. Those with toxic multi- or uninodular goiters were excluded.
All procedures were performed in accordance with institutional guidelines and the principles of the Declaration of Helsinki. The local Institutional Ethics Committee approved the study, and each patient provided written informed consent.
Follow-up protocol
Patients were evaluated at baseline (pre-^131^I) and at 1, 2, 3-, 6-, 9-, and 12-months post-therapy. Thyroid volume was measured by the same examiner using ultrasound (Philips Envisor HD, 12 MHz transducer). Levothyroxine was prescribed if TSH exceeded the upper limit of normal or if free T4 fell below normal.
Laboratory analyses
TRAb (ECLIA): Measured by a competitive electrochemiluminescence assay (Roche Elecsys and Cobas). The positivity cutoff was > 1.75 IU/L.TSI: IMMULITE^®^ 2000/2000 XPi TSI assay (Siemens), with a positivity cutoff of > 0.55 IU/L.TSH, free T4, total T3: Measured via electrochemiluminescence or immunofluorimetry (Roche, PerkinElmer), following established reference intervals.Anti-thyroid peroxidase (ATPO), anti-thyroglobulin (ATG): Measured by Roche Elecsys and Cobas kits. Values were considered positive if > 34 IU/mL for ATPO and > 40 IU/mL for ATG.
For both TRAb and TSI, an increase > 7% from baseline was considered significant.
Statistical analysis
Continuous variables were evaluated by the Mann-Whitney or ANOVA with Tukey’s post-test, as appropriate. Categorical variables were assessed by chi-square or Fisher’s exact test. Normality was checked using the D’Agostino-Pearson test. Significance was defined as p < 0.05.
Declaration of generative AI in scientific writing
In order to enhance the clarity and correctness of the language used in this manuscript, we employed ChatGPT version 01 (OpenAI, 2023) for grammar and linguistic revision. This AI-powered tool helped identify typographical errors and improve readability. Nevertheless, the authors take full responsibility for the content and final approval of the submitted version.
RESULTS
Baseline Characteristics
We studied 39 patients with an average age of 39.6 years, 76.9% of whom were female, diagnosed with Graves’ Disease on average 3.1 years ago, who received a dose of radioactive iodine due to the failure of medication treatment.
Table 1 summarizes the baseline clinical and laboratory characteristics. TRAb was positive in all 39 patients (100%) at diagnosis, while TSI was positive in 38/39 (97.4%).
The sensitivity of ECLIA for the diagnosis of GD was 100%, while for TSI it was 97.4%. There was a good correlation between the two methods (r = 0.66) (Figure 1). As expected, serum TSI levels were significantly lower than those measured by the conventional method (ECLIA) (Figure 2).
Figure 1. Correlation between the values of TSH anti-receptor antibodies (TRAb) measured by conventional method (ECLIA) and one evaluate only TSH receptor stimulating antibodies (TSI).
Figure 2. Measurements of TSH receptor antibodies as determined by the conventional method (ECLIA) or evaluated by TSH receptor stimulating antibodies (TSI).
Antibody Behavior After 131I
Both TRAb and TSI rose significantly between the second and fourth months (p = 0.0003 and p = 0.001, respectively), followed by a decline toward baseline from months 9 to 12 (Figure 3).
Figure 3. Evolution of TRAb (ECLIA) and TSI levels at different follow-up times
TSI levels generally remained elevated slightly longer than TRAb, but both approached pre-treatment values by 12 months (Figure 3).
Among the 39 patients, 28 (72%) showed an initial TSI rise; 93% of these exhibited a subsequent down- ward trend. However, 58% of the 28 still had higher TSI at 12 months compared to baseline (Figure 4).
Figure 4. Relative profiles of TSI after treatment with radioiodine.
Patients with TED, longer disease duration, or higher baseline TSI were more likely to display persistent TSI elevation. Importantly, TSI persistence did not prevent control of thyrotoxicosis; over 90% of patients attained euthyroidism or hypothyroidism by one-year post-therapy (Table 2).
Table 2: Clinical and laboratory characteristics of patients who did and who did not present increasing of TSI after radioiodine
DISCUSSION
Our findings confirm that ^131^I treatment induces an increase in TSH receptor antibodies in most patients with GD. Using both a conventional assay (ECLIA, which detects total TRAb) and a stimulatory-specific assay (TSI), we showed that much of the elevated TRAb activity post-^131^I reflects genuine stimulatory immunoglobulins. Despite this persistent elevation of TSI in many patients, nearly all achieved stable thyroid function by the end of follow-up.
These results dovetail with other investigations showing that the rise and persistence of TRAb (especially stimulatory TRAb) can have important clinical implications, particularly for pregnant women or those planning conception (^20,22^). However, not all studies have shown that TSI offers greater predictive value than conventional TRAb assays for certain GD-related complications. In a recent prospective study of 30 patients with newly diagnosed GD, Khamisi et al. likewise found no additional benefit of using TSI instead of TRAb in predicting or managing Graves’ orbitopathy over a 24-month period (^4^). Their data and ours both underscore that while TSI specifically measures stimulating immunoglobulins, the conventional TRAb assay often correlates strongly with TSI and may suffice for routine clinical monitoring.
From a pathophysiologic standpoint, the immune reconstitution or immunologic changes following ^131^I therapy may maintain TRAb production for extended periods, even in clinical remission. Therefore, women with GD treated with radioiodine who wish to become pregnant could be directly impacted (^22^). Our current data – showing frequent TSI elevation at 9-12 months post-^131^I – provide an additional rationale for carefully monitoring women of childbearing age who might become pregnant soon after definitive therapy. This aspect has been recently demonstrated in the study by Priyanka et al. involving 51 women with GD treated with radioiodine. In this study, TRAb levels of > 19.06 IU/L predicted adverse pregnancy outcomes with 100% sensitivity and 93.5% specificity. More importantly, third trimester maternal TRAb levels of > 7.99 IU/L and day three neonatal TRAb levels of > 5.03 IU/L predicted neonatal thyrotoxicosis with 100% sensitivity and 97.4% specificity (^23^).
Clinical implications
Pregnancy Planning: Because TSI can cross the placenta and potentially cause fetal hyperthyroidism (^19-25^), persistent TSI elevation raises the question of whether a 6-month waiting period after ^131^I is always sufficient before conception (^26^) . Measuring TSI at or near the time of antithyroid drug discontinuation or when counseling women about pregnancy could provide a more individualized risk assessment (^17,27-29^).Thyroid Eye Disease (TED): Patients with active or preexisting TED may be more susceptible to prolonged rises in TSI, which could exacerbate or increase the risk of worsening ophthalmopathy (^30-32^). Earlier recognition and possible prophylactic measures (e.g., glucocorticoids) may be warranted (^33,34^).Dynamics of TSI vs. TRAb: TSI tended to remain elevated slightly longer than total TRAb. Although levels eventually declined toward baseline in most patients, 58% showed values above pre-treatment levels at 12 months. This lingering stimulatory autoimmunity underscores the complexity of GD pathophysiology following ^131^I therapy (^4,6,18,35,36^).
Study limitations
Our main limitation is the relatively small sample size. Larger, prospective studies are needed to confirm these findings, determine optimal timing for TSI measurement, and clarify whether tailoring therapy based on TSI levels reduces fetal hyperthyroidism risk or TED progression.
In conclusion, radioiodine therapy leads to elevated TSI in a significant proportion of patients with GD, with many displaying higher-than-baseline levels one year post-treatment. Although this does not appear to compromise overall treatment success, these data may guide clinical decisions in cases where elevated TSI has critical implications – for instance, in planning pregnancy or managing TED. Our results, together with recent work by others (^23,24,36,37^), highlight the importance of monitoring TSI (or TRAb) for a prolonged period after ^131^I, especially in women of childbearing age.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Smith TJ Hegedüs L Graves’ Disease New Engl J Med.2016 Oct 203751615526510.1056/NEJ Mra 151003027797318 · doi ↗ · pubmed ↗
- 2Dwivedi SN Kalaria T Buch H Thyroid autoantibodies J Clin Pathol.2023 Jan 761192810.1136/jcp-2022-20829036270794 · doi ↗ · pubmed ↗
- 3Liu T Zhang X Long L Zhou L Chen J Li M Clinical evaluation of an automated TSI bridge immunoassay in the diagnosis of Graves’ disease and its relationship to the degree of hyperthyroidism BMC Endocr Disord.2022 Aug 3122121810.1186/s 12902-022-01114-336045442 PMC 9429690 · doi ↗ · pubmed ↗
- 4Khamisi S Lundqvist M Engström BE Larsson A Karlsson FA LjunggrenÖ Comparison Between Thyroid Stimulating Immunoglobulin and TSH-Receptor Antibodies in the Management of Graves’ Orbitopathy Exp Clin Endocr Diab.2023 Apr 13142364110.1055/a-2021-0596 PMC 1015862936706788 · doi ↗ · pubmed ↗
- 5Stan MN Algeciras-Schimnich A Murthy V Thapa P Araki N Diagnostic Utility of a New Assay for Thyroid Stimulating Immunoglobulins in Graves’ Disease and Thyroid Eye Disease Thyroid.2022 Feb 322170610.1089/thy.2021.029934714163 · doi ↗ · pubmed ↗
- 6Ochi Y Inui T Kouki T Yamashiro K Hachiya T Kajita Y Thyroid Stimulating Immunoglobulin (TSI) in Graves’ Disease Endocr J.1998 Dec 456701810.1507/endocrj.45.70110395224 · doi ↗ · pubmed ↗
- 7Kotwal A Stan M Thyrotropin Receptor Antibodies-An Overview Ophthalmic Plast Reconstr Surg.2018 Jul/Aug 344S Suppl 1S 20710.1097/IOP.000000000000105229771756 · doi ↗ · pubmed ↗
- 8Ross DS Radioiodine Therapy for Hyperthyroidism N Engl J Med.2011 Feb 1036465425010.1056/NEJ Mct 100710121306240 · doi ↗ · pubmed ↗