Primary B-cell lymphoma of the renal pelvis following robotic nephroureterectomy: a case report
Thomas McMaster, Gabrielle Hoskin, Thomas Neerhut, Lauren Malacria, Matthew Farag, Luke Wang

TL;DR
A rare case of primary B-cell lymphoma in the kidney was diagnosed after surgery, highlighting challenges in distinguishing it from kidney cancer.
Contribution
This case report adds to the limited literature on primary renal lymphoma following robotic nephroureterectomy.
Findings
A renal pelvis mass initially suspected as urothelial carcinoma was diagnosed as diffuse large B-cell lymphoma post-surgery.
The case emphasizes the importance of biopsy for indeterminate renal lesions to avoid misdiagnosis.
Primary renal lymphoma presents clinical similarities to upper tract urothelial carcinoma, complicating diagnosis.
Abstract
We present a rare case of Primary Renal Lymphoma (PRL) diagnosed on histopathology following robotic nephroureterectomy. This case explores the diagnostic and management challenges urologists face, when treating renal masses. An 82-year-old male presented with recurrent macroscopic haematuria and a computed tomography intravenous pyelogram (CT IVP) reported renal papillary necrosis and an associated mass effect at the right renal pelvis. Urine cytology was inconclusive, whilst inpatient pyeloscopy revealed a renal pelvis tumour. This was biopsied and reported as suspicious for urothelial carcinoma. Multidisciplinary team discussion (MDT) recommended curative surgery. Following right nephroureterectomy, postoperative histology revealed a diffuse large B-Cell lymphoma (DLBCL) extending through the renal capsule into perirenal fat, renal vein and renal pelvis. We highlight the clinical…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
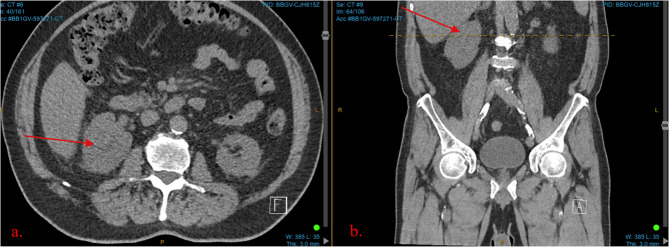 Figure 1
Figure 1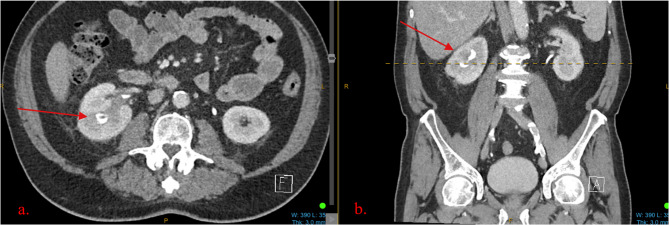 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLymphoma Diagnosis and Treatment · Multiple and Secondary Primary Cancers · Renal cell carcinoma treatment
Background
Primary Renal Lymphoma (PRL) is an exceptionally rare and aggressive form of extra-nodal non-Hodgkin’s lymphoma (NHL), accounting for less than 1% of all renal masses [1]. Its origin in the kidney is unusual due to the absence of native lymphoid tissue, and its pathogenesis remains poorly understood [1]. Owing to its rarity, published literature is limited and diagnosis is frequently missed or delayed. PRL often mimics more common renal malignancies such as Renal Cell Carcinoma (RCC) or upper tract urothelial carcinoma (UTUC), leading to unnecessary surgical interventions and delayed systemic therapy [2–4]. Accurate histopathological diagnosis, typically via renal biopsy, is essential for appropriate management and improved outcomes.
We report a rare case of PRL, identified post-operatively following robotic nephroureterectomy. This work has been reported in line with the CARE guidelines [5].
Case presentation
An 82-year-old man presented with recurrent macroscopic haematuria and right flank pain. A non-contrast computed tomography (CT) scan was initially ordered, reporting a loss of clarity of the right upper pole renal sinus (see Fig. 1). A follow up CT intravenous pyelogram (CT IVP) reported renal papillary necrosis at the right upper pole with associated mass effect at the renal pelvis and appearances suggestive of parapelvic cysts (see Fig. 2). CT chest was unremarkable and urine cytology was negative for high grade urothelial carcinoma. Given the radiological findings, an inpatient pyeloscopy was performed, revealing a macroscopic lesion of the renal pelvis. This was biopsied at the time; however, the sample was deemed insufficient for conclusive histopathological analysis. Clusters of atypical epithelioid cells without unequivocal features of malignancy were noted. This was later verified by another pathologist who reported the sample as suspicious for urothelial carcinoma. The case was discussed at a multi-disciplinary team (MDT) meeting, noting that during pyeloscopy, the lesion was observed to be a tumour consistent with the typical macroscopic appearance of high grade invasive primary urothelial carcinoma.
Fig. 1. Non-contrast CT Kidney, ureter and bladder. **a ** An axial view demonstrating loss of clarity of right upper pole renal sinus. b A coronal view demonstrating the same
Fig. 2CT Intravenous pyelogram. a An axial view demonstrating renal papillary necrosis at the right upper pole with underfilling, associated mass effect at the renal pelvis. b A coronal view demonstrating the same
Following the MDT, the patient was consented and booked for a right robotic nephroureterectomy, with peri-operative medicine and anaesthetic review prior. He was deemed a high-risk surgical candidate, with comorbidities including ischaemic heart disease, diabetes and hypertension, however, cardiac investigations did not preclude surgery. The robotic assisted procedure was uncomplicated, however, in the post-operative period, the patient suffered a type two myocardial infarction, that was conservatively managed.
Despite a presumed diagnosis of invasive upper tract urothelial carcinoma, histopathology revealed a Diffuse Large B-Cell Lymphoma (DLBCL), extending through the renal capsule into perirenal fat, renal vein and renal pelvis. The patient was then referred to the haematology team, who discussed both the role of formal staging with Positron Emission Tomography (PET) imaging as well as the rationale for chemotherapy. After sufficient counselling, the patient declined all further investigations and management, instead, opting for palliation and a referral for consideration of voluntary assisted dying.
Discussion
PRL is a rare diagnosis, accounting for less than 1% of renal masses [1]. Its clinical and radiological overlap with UTUC makes differentiation challenging, often leading to misdiagnosis and unnecessary surgery. This is particularly significant in elderly or comorbid patients, where avoiding invasive procedures may improve outcomes.
Epidemiology
PRL shows a slight male predominance and occurs more frequently in white, middle-aged to elderly individuals [4]. UTUC, similarly more common in older men, is strongly associated with tobacco exposure and peaks between ages 70–90 [6].
Clinical presentation
PRL often presents unilaterally and is asymptomatic in up to 50% of cases [1]. When symptomatic, younger patients tend to report flank pain, whilst older individuals may present with haematuria or weight loss [4]. Constitutional features of lymphoma, such as, fever or elevated LDH may also be seen. UTUC commonly presents with haematuria and flank pain, symptoms that also correlate with disease progression [6].
Investigation
Imaging
CT remains the mainstay radiological investigation for both PRL and UTUC. PRL may appear as a solitary or multifocal mass, with or without nodal involvement, and sometimes demonstrates atypical features like necrosis or infiltration [7]. 18 F-FDG PET CT may aid diagnosis and staging [7]. CT urography offers high diagnostic accuracy for UTUC, though distinguishing it from other renal masses (e.g., renal cell carcinoma (RCC), other metastases, focal xanthogranulomatous pyelonephritis (XGP), or PRL) can be difficult, particularly when the renal architecture is distorted [3, 8].
Diagnostic procedures
When imaging and urine cytology are inconclusive, diagnostic ureteroscopy (dURS) with biopsy allows visualisation and sampling of upper tract lesions [8]. Although dURS carries a potential risk of tumour seeding, it remains a valuable tool in selecting appropriate management pathways.
Management
Due to its rarity, there is no standardised treatment for PRL, but systemic chemoimmunotherapy agents, such as R-CHOP (rituximab, cyclophosphamide, vincristine, prednisolone), remain the cornerstone of B cell PRL treatment [9]. Some reports suggest benefit from surgical resection followed by adjuvant therapy [10], though evidence is limited. Conversely, UTUC management is well-established and guided by risk stratification: low-risk disease may be managed conservatively, while high-risk cases typically require radical nephroureterectomy and systemic therapy [9].
Conclusion
We have reported a rare case of PRL diagnosed on histopathology following robotic nephroureterectomy. PRL is a rare and often misdiagnosed renal malignancy, easily mistaken for more common pathologies such as UTUC. This case underscores the importance of physicians maintaining a high index of suspicion for rare pathologies, particularly when standard investigations are inconclusive or clinical presentations are atypical.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bokhari MR, Rana UI, Bokhari SRA, Renal Lymphoma. [Updated 2023 Jul 10]. In: Stat Pearls. Treasure Island (FL): Stat Pearls Publishing; 2025. Available from: https://www.ncbi.nlm.nih.gov/books/NBK 526034/.
- 2Zhao K, Zhang Q, Cong R, Wang Y, Wang Z, Song N. Primary renal lymphoma: a case report and review of the literature. AME Case Rep. 2020. 10.21037/acr.2019.12.03.10.21037/acr.2019.12.03PMC 722132232420531 · doi ↗ · pubmed ↗
- 3EAU guidelines on upper urinary tract urothelial cell carcinoma - uroweb. European Association of Urology. (n.d. -a). https://uroweb.org/guidelines/upper-urinary-tract-urothelial-cell-carcinoma/chapter/epidemiology-aetiology-and-pathology.10.1016/j.eururo.2015.06.04426188393 · doi ↗ · pubmed ↗
- 4EAU guidelines on upper urinary tract urothelial cell carcinoma - uroweb. European Association of Urology. (n.d.-a). https://uroweb.org/guidelines/upper-urinary-tract-urothelial-cell-carcinoma/chapter/diagnosis.10.1016/j.eururo.2015.06.04426188393 · doi ↗ · pubmed ↗
- 5EAU guidelines on upper urinary tract urothelial cell carcinoma - uroweb. European Association of Urology. (n.d.-a).https://uroweb.org/guidelines/upper-urinary-tract-urothelial-cell-carcinoma/chapter/disease-management.10.1016/j.eururo.2015.06.04426188393 · doi ↗ · pubmed ↗
- 6Witkowska M, Romejko-Jarosińska J, Giza A, Drozd-Sokołowska J, Mikulski D, Hałka J, et al. Primary Renal Lymphoma: Report of 32 Cases—A Retrospective Multicenter PLRG Analysis. Biomedicines. 2025;13(3):548.10.3390/biomedicines 13030548 PMC 1194005240149524 · doi ↗ · pubmed ↗