Risk factors of pressure injury in elderly inpatients: a systematic review and meta-analysis
Qingyi Wu, Nini Cheng, Fanfan Cao, Huan Wen, Mei Sun

TL;DR
This study identifies key risk factors for pressure injuries in elderly hospitalized patients and highlights their preventability.
Contribution
A comprehensive meta-analysis revealing eight major risk factors for pressure injury in elderly inpatients.
Findings
Immobility and incontinence show the highest odds ratios for pressure injury development.
Nutritional risk and diabetes are significant contributors to pressure injury prevalence.
Longer hospital stays and ICU durations increase the risk of pressure injuries.
Abstract
The aim of this systematic review is to systematically identify and synthesize the risk factors contributing to pressure injury in elderly inpatients. Methods: PubMed, Embase, Web of Science, Cochrane Library, and CINAHL were systematically searched from database inception to March 1, 2025. Two researchers independently screened the retrieved studies and extracted the data. The risk of bias was assessed using the AHRQ criteria or the Newcastle–Ottawa Scale (NOS). Meta-analysis was performed using R version 4.5.0. Results: A total of 3,629 studies were retrieved, and 23 studies met the inclusion criteria. Altogether, 70,340 participants were included in the analysis, of whom 5,792 developed PI during hospitalization, corresponding to an overall prevalence of 8.2%. Meta-analysis showed that age (OR = 1.06, 95%CI: 1.03 to 1.09), immobility (OR = 4.54, 95%CI: 3.09 to 6.67), incontinence (OR…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
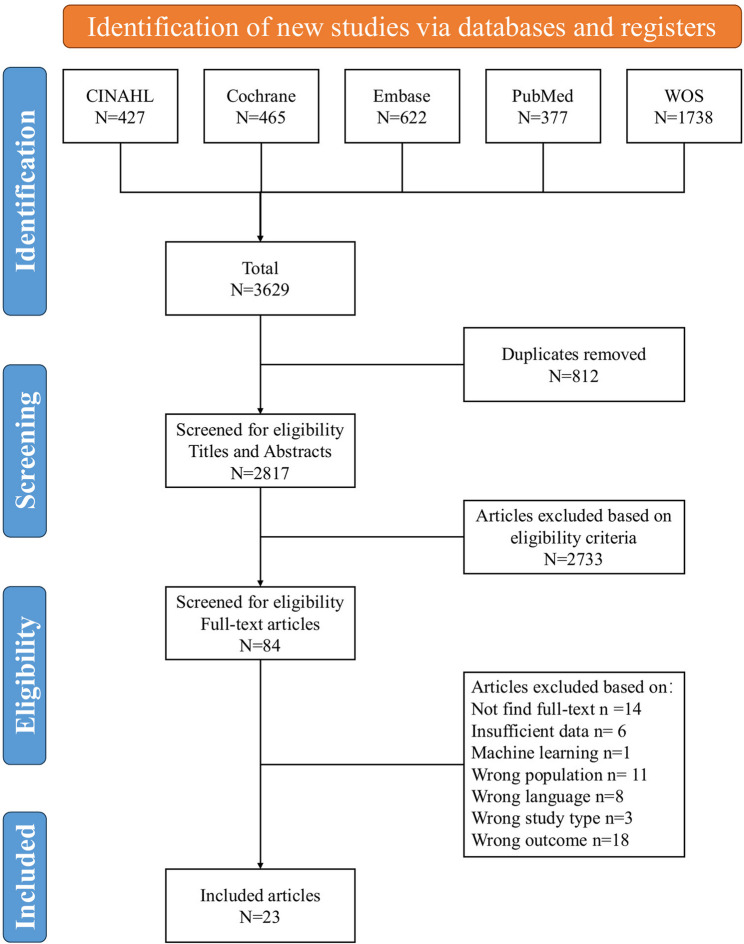 Figure 1
Figure 1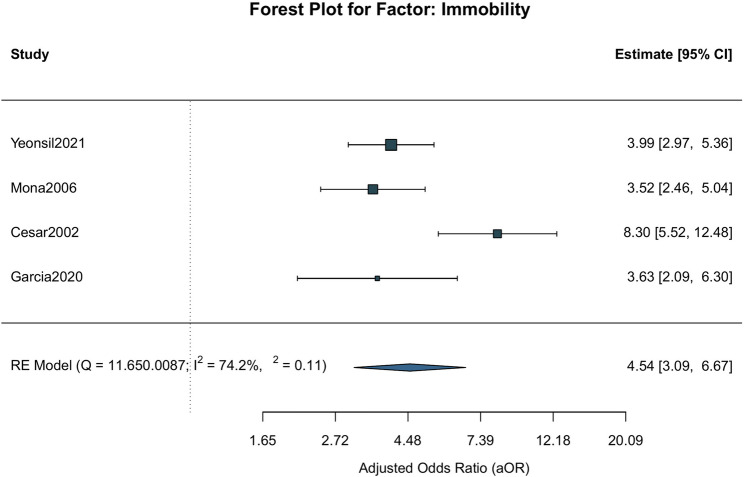 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPressure Ulcer Prevention and Management · Stoma care and complications · Pelvic floor disorders treatments
Introduction
Pressure injury (PI) is defined as localized damage to the skin and/or underlying tissue, usually over a bony prominence or associated with medical or other devices, resulting from prolonged pressure or pressure in combination with shear [1]. PI is a significant clinical problem that requires urgent attention, especially among older adults. On the one hand, epidemiological evidence shows that the prevalence of PI remains high in hospital settings worldwide, with older adults being disproportionately affected. A global systematic review and meta-analysis [2] involving including more than 2.5 million hospitalized adult patients reported a pooled PI prevalence of 12.8%, with hospital-acquired pressure injury rates accounting for nearly two-thirds of all cases; another global burden of disease study [3] revealed that the age-standardized prevalence rates of PI were notably higher in individuals aged 60 and older compared to younger age groups. On the other hand, PI has sever negative impacts on patients’ physical functioning, mental health, and social participation [4], even leading to death/medical malpractice [5]. Furthermore, PI also imposes a substantial burden on society, leading to considerable healthcare and treatment costs. In Australia, the total cost of PI in public hospitals was estimated at 3.60 billion attributable to the opportunity cost of excess length of stay and $3.59 billion to treatment expenses [6]. Therefore, the high prevalence, severe consequences, and heavy economic burden make PI a major health challenge for elderly patients, healthcare systems, and society.
The aging population bringing numerous health challenges, particularly regarding PI. According to the World Health Organization, the global population aged 60 years and older is projected to reach 2.1 billion by 2050, nearly doubling from 1 billion in 2020 [7]. This demographic shift suggests that the number of elderly patients at risk of PI will increase significantly. Therefore, it is essential to identify risk factors for PI in elderly inpatients and implement targeted preventive measures. However, most existing studies have focused on individual factors, and a critical gap remains: no comprehensive systematic evaluation has synthesized all known risk factors to clearly delineate their relationships with PI development in elderly inpatients. This study systematically reviewed the literature on the risk factors of PI in elderly hospitalized patients and conducted a Meta-analysis on the risk factors. Addressing the gap may enable clinicians to better stratify risk, prioritize interventions, and develop evidence-based prevention protocols tailored to elderly inpatients.
Method
The study was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines[8], and the protocol has been registered on PROSPERO (CRD420251010457).
Search strategy
The studies search was performed in PubMed, Embase, Web of Science, Cochrane Library, and CINAHL from inception to March 1, 2025. Search terms were “Older Adults”, “Inpatients”, “Pressure Ulcer” and “Risk Factors”. We used a combination of subject terms and free words, Boolean logical operators, and truncation to search in the target database. The full search strategy can be found in Appendix 1.
Eligibility criteria
Inclusion Criteria: We included cohort, case-control and cross-sectional studies that investigated elderly inpatients, defined as individuals aged 60 years or older who are admitted to a hospital for any forms of inpatient care; Eligible studies examined risk factors associated with PI, such as nutritional status[9], level of physical activity[10], chronic disease[11], urinary incontinence [12] or length of hospitalization[13], and reported outcomes of PI during hospitalization [14]. Only articles published in English were considered.
Exclusion Criteria: We excluded studies that were not original research (e.g., reviews, editorials, conference abstracts), those involving residents of nursing homes or long-term care facilities, and studies in which PI had already occurred at the time of hospital admission.
Screening and data extraction
Two researchers independently screened the retrieved studies and extracted data using EndNote21, following Eligibility Criteria. The results were cross-checked for accuracy. Any disagreements were resolved through discussion, and when consensus could not be reached, the second author served as the third researcher for adjudication. Extracts include: first author, year of publication, country, sample size, age (mean ± standard deviation or range), risk factors with P < 0.05 and their effect values and 95% confidence intervals (CI).
Quality assessment
Cross-sectional studies were assessed using the Agency for Healthcare Research and Quality (AHRQ) [15] criteria, which includes 11 items. Studies scoring 8 to 11 were considered high quality, 4 to 7 were considered medium quality, and 0 to 3 were considered low quality. Case-control and cohort studies were evaluated using the Newcastle-Ottawa Scale (NOS) [16]. The evaluation consisted of 3 columns with 8 entries, which were scored according to the criteria of the entries. 5 to 9 were categorized as high quality, and 0 to 4 were categorized as low quality.
Data analysis
All statistical analyses were conducted using the R software (version 4.5.0), specifically employing the “metafor”[17] package. The natural logarithms of the adjusted odds ratios (aOR) and 95%CI were used to calculate effect estimates and corresponding standard errors (SEs). Within-study variances were computed as the squared SEs. One study reported the association as a regression coefficient (β) from a logistic regression model. This value was transformed into an aOR using exponentiation (aOR = exp[β]) to enable its inclusion in the meta-analysis. Additionally, effect estimates such as risk ratio (RR), adjusted risk ratio (aRR), and adjusted hazard ratio (aHR) reported by only one study, respectively, were excluded from meta-analysis. They were instead presented narratively to complement the quantitative findings.
A random-effects model was primarily used to account for potential heterogeneity among studies. Heterogeneity among studies was assessed using the I², τ², and Cochran’s Q test. I² value between 0% and 40% might not be important, 30% to 60% may indicate moderate heterogeneity, 50% to 90% may represent substantial heterogeneity, and 75% to 100% suggests considerable heterogeneity [18]. If heterogeneity is low, the results of the fixed effects model are reported.
Sensitivity analyses were conducted by comparing results from fixed-effects and random-effects models. Forest plots were used to visually present individual and pooled effect estimates. A significance level of P < 0.05 was considered statistically significant.
Results
Characteristics of included studies
A total of 3629 studies were retrieved 2817 remaining after eliminating duplicates, and finally 23 studies[9–13, 19–36] met eligibility criteria, including 1 case-control study, 4 cross-sectional studies, and 18 retrospective cohort studies. The process of studies screening is shown in Fig. 1. Detailed information on the literature characteristics for each included study can be found in Table 1.Fig. 1. Flowchart of section studies
Table 1. Basic characteristics of included studiesAuthorYearCountryDesignCase/TotalAgeRisk FactorsEffect valuesScoresAnthony2000EnglandCohort113/773≥ 65Waterlow score, albumin aOR 8Baumgarten2003USACohort824/9400≥ 60time to surgery, surgical anesthesia, durations of prior ICU stay, age, ADL, nutritional risk, health status bad, Charlson Comorbidity Index aOR 9Baumgarten2006USACohort266/3233≥ 65age, male, dry skin, incontinence, immobility, nursing home, hospitalized history, nutritional risk aOR 7Baumgarten2008USACase-control195/792≥ 65durations of prior ICU stay, medication aOR 8Baumgarten2012USACohort96/65883.2 ± 6.6length of stay in emergency department, time from inpatient admission to surgery, general anesthesia aRR 8Casimiro2002SpainCross-sectional295/82782.4 ± 8.0age, BMI, history of ulcer, immobility, poor circulation, diabetes, sensory changes, erythema aOR 8Cataneo-Piña2023MexicoCohort37/11882.1 ± 5.6length of stay aOR 8Chiari2017ItalyCohort246/108384.1 ± 7.6age, railings on the bed, positioning, catheter, caregiver, foam valve, pain aOR 8Compher2007USACohort608/321477.3 ± 7.9BMI aOR 9Garcia2021SpainCohort90/29982.3 ± 8.0age, origin home, outdoor life, walking, immobility, nutritional risk aOR 9Gazineo2019ItalyCohort91/76183.68 ± 7.9Braden score, diaper, catheter, foam valve, surgical procedure aHR 7Han2018KoreaCohort1368/34,287≥ 65female, age, admission via wheelchair, drowsy, Braden score aOR 7Jaul2019IsraelCross-sectional23/40median 73.5dementia, spasticity aOR 9Kartal2023TurkeyCross-sectional117/38276.20 + 8.36age, BMI, clinical diagnosis, length of stay, admission via stretcher-wheelchair, tube feeding, insulin and steroids RR 8Man2013ChinaCohort17/22983.35 ± 7.69hypotension, use of restraint, length of stay aOR 8Mecocci2005ItalyCohort412/137978.38 ± 7.2cognitive impairment aOR 9Mohammed2024EgyptCohort31/33472.35 ± 8.1nutritional risk aOR 8Moon2021KoreaCohort328/826373.84 ± 6.33age, admission via emergency department, low income, incontinence, immobility aOR 9Ottaviani2024ItalyCohort152/31685 ± 7age, mobility, friction/shear, albumin, hemoglobin, Barthel, Mini Nutritional Assessment aOR 8Papanikolaou2002EnglandCohort47/213≥ 65poor appetite, broken skin, incontinence, age, cancer, Parkinson β 8Papier2022IsraelCohort80/89577.6 ± 9.1Norton score, albumin, low intake aOR 7Rademakers2007NetherlandsCohort214/72276.9 to 87.5diabetes, urinary tract infection, hip dislocation, American Society of Anesthesiologists Classification, time to surgery aOR 8Stephenson2023PolandCross-sectional143/212282.18 ± 7.90nutritional risk aOR 10“USA” United States of America. “Scores” represents the scores of studies quality evaluation
Quality assessment
The quality of the studies was assessed using the AHRQ checklist or the NOS, with scores ranging from 7 to 10, indicating generally moderate to high methodological quality (Table 1). This evaluation supports the reliability of the findings presented in our meta-analysis.
Prevalence of pressure injuries
A total of 70,340 participants were included in the analysis. Among them, 5792 participants developed PI during hospitalization, corresponding to an overall prevalence of approximately 8.2%.
Results of Meta-analysis
We performed risk factors that were reported in two or more studies. A total of 10 risk factors were included. For each factor, both fixed-effect and random-effects models were applied. Specifically, factors with high heterogeneity were analyzed using random-effects models, while those with low heterogeneity were analyzed using fixed-effect models. Table 2 summarizes the meta-analysis results of two models. Finally, a total of 8 risk factors were found to be statistically significant. For interpretability, the identified risk factors were further classified into two categories: non-modifiable patient characteristics and modifiable care-related factors.Table 2. Meta-analysis results of risk factors of PI in elderly inpatientsRisk FactorsNRandom Effect ModelFixed Effect ModelORCIP-valI^2^ORCIP-valage91.06(1.03, 1.09)0.000183.701.04(1.03, 1.05)< 0.0001immobility44.54(3.09, 6.67)0.000074.204.45(3.69, 5.37)< 0.0001albumin31.12(0.72, 1.74)0.625085.701.17(1.12, 1.22)< 0.0001incontinence39.97(2.33, 42.75)0.002087.204.00(2.75, 5.82)< 0.0001nutritional risk33.00(1.78, 5.05)0.000080.202.41(1.99, 2.92)< 0.0001BMI20.39(0.05, 3.34)0.391078.300.94(0.92, 0.96)< 0.0001diabetes21.60(1.21, 2.11)0.00100.001.60(1.21, 2.11)< 0.0001ICU stay21.93(1.46, 2.55)0.00000.001.93(1.46, 2.55)< 0.0001time to surgery22.06(1.58, 2.69)0.00004.202.07(1.60, 2.67)< 0.0001length of stay21.05(1.01, 1.09)0.014665.001.05(1.02, 1.07)< 0.0001Notes: “N” means the number of studies
The results of the meta-analysis showed that risk factors of non-modifiable patient characteristics: age (OR = 1.06, 95%CI: 1.03 to 1.09, P = 0.0001), immobility (OR = 4.54, 95%CI: 3.09 to 6.67, P < 0.0001), diabetes (OR = 1.60, 95%CI: 1.21 to 2.11, P = 0.0010) and durations of prior ICU stay (OR = 1.93, 95%CI: 1.46 to 2.55, P < 0.0001); risk factors of modifiable care-related factors: incontinence (OR = 4.54, 95%CI: 2.33 to 42.75, P = 0.0020), nutritional risk (OR = 3.00, 95%CI: 1.78 to 5.05, P = 0.0020), time from admission to surgery (OR = 2.07, 95%CI: 1.60 to 2.67, P < 0.0001) and length of stay (OR = 1.05, 95%CI: 1.01 to 1.01, P = 0.0146). Those are statistically significant associated with the occurrence of PI in elderly inpatients. In contrast, albumin (OR = 1.12, 95%CI: 0.72 to 1.74, P = 0.6250) and BMI (OR = 0.39, 95%CI: 0.05 to 3.34, P = 0.3910) were not significantly associated. The forest plot as an example of the relationship between comorbid immobility and the occurrence of PI in elderly inpatients (Fig. 2).Fig. 2. Forest plot of immobility
Sensitivity analyses
To assess the stability of the meta-analysis results, sensitivity analyses were performed comparing the random-effects model and the fixed-effects model (Table 2). Excepting incontinence, the magnitude of the effect estimates differed slightly, the direction and statistical significance remained consistent across models, indicating the findings are stable. Factor BMI and albumin yielded a statistically significant association in the fixed-effects model, while not in the random-effects model.
Publication bias assessment
Due to the limited number of included studies, we did not perform publication bias assessments such as funnel plots or Egger’s test.
Narrative synthesis
In addition, several studies reported effect estimates such as aRR, aHR and RR. They were not included in the meta-analysis but are summarized in Table 3.Table 3. Studies with effect estimates not pooled in the meta-analysisStudyFactorsEffect estimatesValues95%CIBaumgarten2012 [20]length of stay in emergency departmentaRR0.680(0.48, 0.96)time from admission to surgery1.620(1.24, 2.11)general anesthesia0.660(0.49, 0.88)Gazineo2019 [29]Braden scoreaHR0.884(0.806, 0.969)diaper1.007(1.001, 1.013)catheter1.013(1.006,1.019)foam valve1.017(1.01, 1.023)osteosynthesis1.876(1.183, 2.975)Kartal2023 [35]ageRR2.551(1.616, 4.026)BMI0.842(0.786, 0.942)clinical diagnosis1.647(1.055, 2.569)length of stay10.681(6.444, 17.704)non-ambulatory admission3.947(2.009, 7.753)tube feeding1.380(1.212, 1.572)antibiotics and insulins6.986(2.730, 17.875)
Baumgarten et al. (2012), [20] a cohort study of 658 elderly patients, found that time from admission to surgery > 24 h (aRR = 1.62, 95%CI: 1.24 to 2.11) was associated with increased hospital-acquired PI risk, while length of stay in emergency department > 6 h (aRR = 0.68, 95%CI: 0.48 to 0.96) and general anesthesia (aRR = 0.66, 95%CI: 0.49 to 0.88) were associated with reduced risk.
Gazine et al. (2019) [29] identified risk factors associated with hospital-acquired PI using multivariate Cox regression analysis. Several factors were found to be significant. Specifically, a higher Braden score was associated with a lower risk (aHR: 0.884, 95% CI: 0.806 to 0.969). Conversely, factors such as diapers postoperatively (aHR: 1.007, 95% CI: 1.001 to 1.013), urinary catheters (aHR: 1.013, 95% CI: 1.006 to 1.019), increased percentage of days using foam valves preoperatively (aHR: 1.017, 95% CI: 1.010 to 1.023), and undergoing osteosynthesis (aHR: 1.876, 95% CI: 1.183 to 2.975) were positive and significant.
Kartal et al. (2023),[35] a cross-sectional analysis of 382 patients, showed that age ≥ 75 years (RR = 2.551, 95% CI: 1.616 to 4.026), BMI (RR = 0.842, 95% CI: 0.786 to 0.942), clinical diagnoses related to cardiovascular, respiratory, and COVID-19 systems (RR = 1.647, 95% CI: 1.055 to 2.569), length of stay ≥ 15 days (RR = 10.681, 95% CI: 6.444 to 17.704), non-ambulatory admission (RR = 3.947, 95% CI: 2.009 to 7.753), tube feeding (RR = 1.380, 95% CI: 1.212 to 1.572), and treatment with antibiotics and insulins (RR = 6.986, 95% CI: 2.730 to 17.875) were all significantly associated with increased PI risk.
Discussion
Age, diabetes, and duration of prior ICU stay represent intrinsic patient vulnerabilities that are not amenable to modification. These factors reflect a higher degree of physiological frailty, impaired tissue perfusion, and chronic metabolic compromise, all of which predispose elderly individuals to PI development. For example, age-related skin changes include loss of dermal vessels, thinning of the epidermis, flattening of the dermal-epidermal junction, loss of elastic fibers, loss of subcutaneous fat, decreased rate of epithelialization, and decreased cell viability [37]. Persistent elevation of blood glucose induces metabolic dysregulations that result in peripheral neuropathy and vasculopathy. The ensuing loss of protective sensation, combined with compromised microcirculation (due to endothelial damage and capillary basement membrane thickening) and impaired immunity, significantly elevates susceptibility to PI[38]. It is also one of the main reasons why wounds are difficult to heal [39]. Longer durations of prior ICU stay may be associated with sustained immobility, hypo-perfusion, and exposure to risk-enhancing interventions (e.g., mechanical ventilation[40], vasopressors [41]), all of which may exacerbate risk of PI.
In contrast, immobility, incontinence, nutritional risk, time from admission to surgery and length of stay are dynamic, extrinsic factors that are closely tied to the quality and continuity of nursing delivered during hospitalization.
Prolonged immobility prevents natural pressure relief. Unrelieved pressure between bony prominences (like sacrum, hip, heel) and support surfaces compresses small blood vessels [42]. Inadequate blood flow deprives tissue of oxygen and nutrients, causing a buildup of metabolic waste, leading to local cell death and tissue necrosis [42]. Similarly, the Clinical Practice Guideline 2025 states that repositioning should be performed every two to three hours for at-risk individuals, particularly those with limited mobility [1].
Poor nutrition impairs skin integrity and wound healing. Protein deficiency impairs fibroblast proliferation, collagen synthesis, angiogenesis, and immune function, weakening wound structure [43]. Inadequate calories force the body to break down protein for energy, leading to further muscle and structural protein loss [44]. Lack of micronutrients impaired enzymatic reactions essential for tissue regeneration and immunity [45]. The clinical practice also showed that malnourished patients receiving intensive nutrition had better PI healing outcomes than standard care [46]. We recommend nutritional screening to enhance individualized nutritional care for patients to decrease PI.
Incontinence (urinary and fecal) showed the largest cumulative effect size in our analyses, but the confidence interval was extremely wide (OR = 9.97, 95% CI: 2.33–42.75). This was mainly driven by the study [25] that reported an unusually high OR, which substantially influenced the pooled estimate. Overall, Patients with incontinence are 4.5 times more likely to develop PI than those without incontinence. Incontinence exposes the skin to prolonged moisture and chemical irritants. Urine, often alkaline due to ammonia, raises skin pH, compromising the acid mantle that protects against pathogens; Feces contain digestive enzymes (e.g. proteases, lipases) that degrade lipids and proteins in the stratum corneum, further weakening the skin [47]. Moreover, other studies confirmed that dual incontinence was more damaging to skin integrity than urinary incontinence alone [48, 49]. This is consistent with the results of our meta-analysis. we recommend that clinicians strengthen the assessment of patients’ excretory function as part of routine PI risk screening. For patients with incontinence, particular attention should be paid to the condition of the perianal skin.
Prolonged time from admission to surgery is associated with a higher risk of PI, possibly due to extended periods of immobility and inadequate preventive care during the preoperative phase. Patients awaiting surgery may remain in a catabolic state, and delays in surgical intervention are often accompanied by increased exposure to risk factors such as malnutrition, hemodynamic instability, and limited mobility, which collectively increase susceptibility to tissue breakdown. Clinically, patients experiencing prolonged delays exhibited significantly higher odds of PI across various surgical cohorts [50, 51]. These findings suggest a dose–response relationship where longer delays incrementally increase ischemic exposure and pressure injury risk. So, reducing the time from admission to surgery is important, which calls for improved coordination among inpatient ward, surgical, and geriatric teams to streamline preoperative assessments and avoid unnecessary delays.
The length of stay is a common factor. It creates cumulative and synergistic effects — cumulative exposure to multiple risk factors, which we refer — significantly heightening the risk of PI.
BMI and albumin are not statistically associated with the occurrence of PI in elderly inpatients. It is an interesting finding because low BMI and hypoalbuminemia have traditionally been considered indicators of malnutrition. But their role as independent predictors remains controversial. Several recent studies [52, 53] have questioned the predictive value of albumin alone due to its sensitivity to acute illness and inflammation, rather than true nutritional status. Similarly, evidence [54] indicated a non-linear (J‑shaped/U‑shaped) association between BMI and PI: both underweight and obesity significantly increase risk compared to normal BMI. It is making pooled results inconsistent across studies.
Unlike the commonly recognized risk factors for PI — such as pressure, friction, shear forces, and moisture — the study identified several patient- and treatment-related factors, which may be particularly relevant in the elderly population. For instance, incontinence is a significant and modifiable risk factor in our analysis. Compared to younger individuals, older adults are more prone to fractures [55] and cardiovascular diseases [56]. These conditions are often accompanied by varying degrees of urinary or fecal incontinence, which can prolong tissue exposure to pressure and compromise the protective mechanisms of skin, increasing the risk of PI. Therefore, we recommend that clinicians perform comprehensive and individualized risk assessments for hospitalized elderly patients, focusing on physical function, excretion, comorbidities, and nutritional support. Such targeted assessments enable the early identification of high-risk individuals. Timely evidence-based prevention strategies and continuously precise nursing aimed at reducing PI.
The study has several limitations: (1) The risk factors analyzed varied widely among studies, and some cases could not be synthesized, thereby limiting the comprehensiveness of this meta-analysis. (2) Some risk factors were explored in only a few studies, reducing the statistical power and generalizability of the findings. (3) There was considerable variability in sample sizes across studies, which could contribute to heterogeneity and affect the stability of the pooled results.
Conclusion
This meta-analysis identified the age, immobility, incontinence, nutritional risk and length of stay, time of prior ICU stay, time from admission to surgery, and diabetes as significant risk factors for PI in elderly inpatients. These findings provide more scientific, stable, and reliable evidence than individual studies, and may help clinical personnel recognize the high-risk patients and implement preventive strategies. However, because most included studies were retrospective, the findings may reflect associations influenced by confounding rather than definitive causal relationships. Future multicenter, large-sample, high-quality randomized controlled trials are needed to further validate these findings and strengthen causal inferences.
Supplementary Information
Supplementary Material 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1National Pressure Injury Advisory Panel, European Pressure Ulcer Advisory Panel and Pan Pacific Pressure Injury Alliance. Pressure Ulcers/Injuries: Definition ad Etiology. In: Prevention and Treatment of Pressure Ulcers/Injuries: Clinical Practice Guideline. The International Guideline: Fourth Edition. Emily Haesler (Ed.). 2025. https://internationalguideline.com.
- 2Li Z, Lin F, Thalib L, Chaboyer W. Global prevalence and incidence of pressure injuries in hospitalised adult patients: Asystematic review and meta-analysis. Int I Nurs Stud. 2020;105:103546. 10.1016/.inurstu.2020.103546.10.1016/j.ijnurstu.2020.10354632113142 · doi ↗ · pubmed ↗
- 3Zhang S, Wei G, Han L, Zhong W, Lu Z, Niu Z. Global, regional and National burden of decubihus ulcers in 204 countries andterritories from 1990 to 2021: a systematic analysis based on the global burden of disease study 2021. Front Public Health 2025:13:1494229. 10.3389/fpubh.2025.1494229.10.3389/fpubh.2025.1494229 PMC 1189756140078762 · doi ↗ · pubmed ↗
- 4Liu S, Rawson H, Islam RM, Team V. Impact of pressure injuries on health-related quality of life: A systematic review. Wound Repair Regen Jan-Feb. 2025;33(1):e 13236. 10.1111/wrr.1323610.1111/wrr.1323639578671 · doi ↗ · pubmed ↗
- 5Labeau SO, Afonso E, Benbenishty J, et al. Prevalence, associated factors and outcomes of presure injuries in adult intensivecare unit patients: the decubicus study. Intensive Care Med. 2021:47(2):160-9. 10.3389/fpubh.2025.149422910.1007/s 00134-020-06234-9PMC 788091333034686 · doi ↗ · pubmed ↗
- 6Organization WH. Ageing and health. World Health Organization. Updated October 1, 2024. Accessed June 16, 2025. https://www.who.int/news-room/fact-sheets/detail/ageing-and-health
- 7Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA (editors). Cochrane Handbook for Systematic Reviews of Interventions version 6.5 (updated August 2024). Cochrane, 2024. www.cochrane.org/handbook.10.1002/14651858.ED 000142 PMC 1028425131643080 · doi ↗ · pubmed ↗
- 8Moon Y, Han S, Kim Y, et al. Hospital adverse outcomes of the elderly in a tertiary referral hospital: A prospective cohort study of 9,586 admissions. Archives Of Gerontology And Geriatrics. 2021-1-1 2021;92. 10.1016/j.archger.2020.104253.10.1016/j.archger.2020.10425333032184 · doi ↗ · pubmed ↗