Accessory breast granulomatous mastitis: A case report and mini-review of the literature
Abdulwahid M. Salih, Ari M. Abdullah, Lana R.A. Pshtiwan, Sakar O. Arif, Zuhair D. Hammood, Shaban L. Tofiq, Hiwa O. Abdullah, Masty K. Ahmed, Harzal Hiwa Fatih, Meer M. Abdulkarim, Fahmi H. Kakamad

TL;DR
This paper reports a rare case of granulomatous mastitis in accessory breast tissue and reviews similar cases, highlighting the effectiveness of surgery over medication for long-term outcomes.
Contribution
The study presents a rare case of GM in accessory breast tissue and provides a mini-review of recent cases to guide treatment strategies.
Findings
GM in accessory breast tissue is rare and can recur despite corticosteroid treatment.
Surgical excision may offer more durable outcomes compared to conservative treatments.
Pregnancy and lactation history are common among GM patients.
Abstract
Granulomatous mastitis (GM) is a rare inflammatory condition that primarily affects the breasts, and its occurrence in accessory breast tissue is even rarer. The present report describes the case of a patient with GM in the accessory breast. A 43-year-old female patient presented with a 1-month history of pain in the left axilla and breast. An analysis of her medical and surgical history did not reveal any notable findings, but she had a history of four full-term pregnancies and a cumulative lactation period of 4 years. Upon a clinical examination, a palpable, ill-defined, tender mass was noted along with an accessory breast and nipple in the axilla. The diagnosis was chronic mastitis, and she was treated with oral corticosteroids, amoxicillin, cabergoline and analgesics. Her condition initially improved; however, the symptoms recurred 1 year later. A wide local excision of the left…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
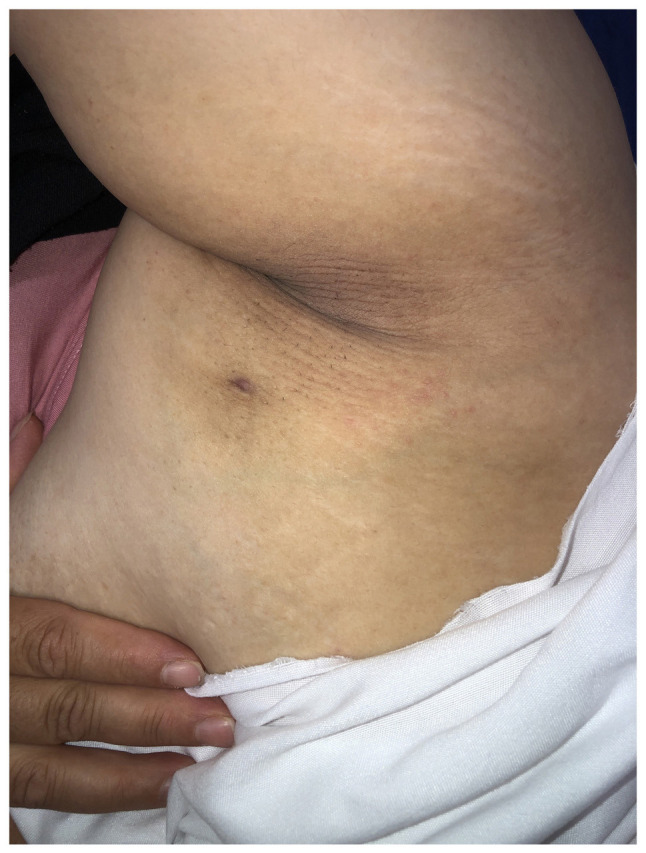 Figure 1
Figure 1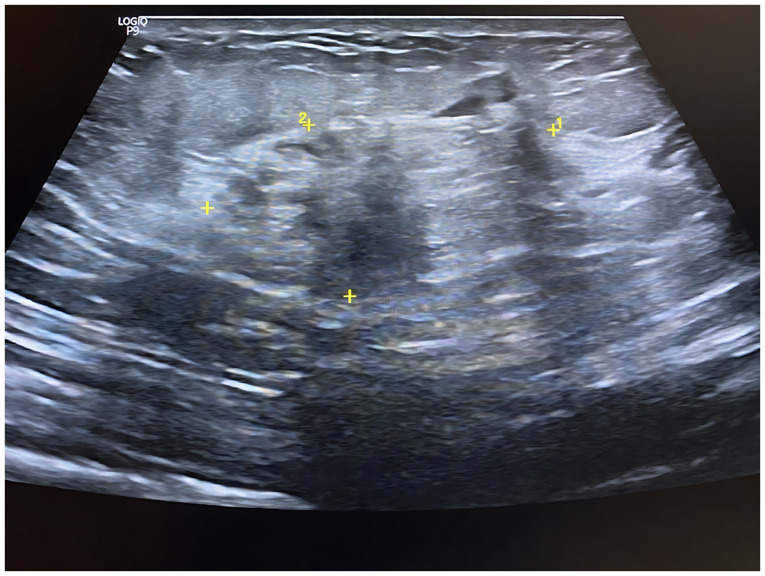 Figure 2
Figure 2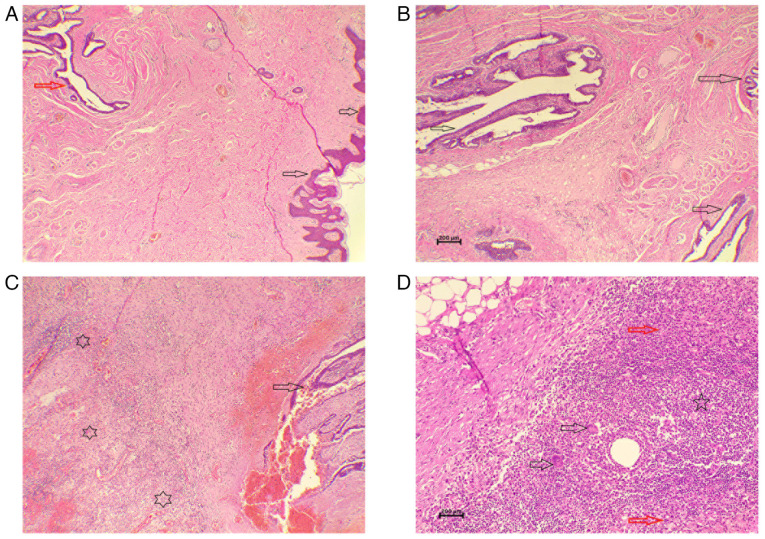 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBreast Lesions and Carcinomas · Cancer and Skin Lesions · Metastasis and carcinoma case studies
Introduction
Granulomatous mastitis (GM) is a rare inflammatory condition of the breast that primarily affects women of childbearing age, often with a history of breastfeeding. GM is categorized into idiopathic or primary GM and secondary GM (1,2). It primarily involves the mammary gland, although in rare cases, it can develop in accessory breast tissue (2). While the exact cause of GM remains unclear, the leading hypothesis suggests an autoimmune origin. Various factors, including medications, diabetes, trauma and smoking, may trigger the inflammatory response. However, the strongest associations with GM are pregnancy, lactation and hyperprolactinemia. The disease accounts for <1% of breast biopsies (3). Despite being a benign disease, GM is frequently difficult to detect, as it often masquerades as breast carcinoma, which is the primary concern at the clinical stage (4). Its locally aggressive character causes long-term discomfort and distress for affected patients. Its non-specific imaging findings can lead to delayed diagnosis, misinterpretation and potentially unnecessary invasive procedures. Only a limited number of cases of GM in axillary breast tissue have been documented (1,2). The present report describes the case of a 43-year-old female patient with GM in the accessory breast. The report has been organized following the CaReL guidelines, and only reliable, peer-reviewed sources were included, while excluding any untrustworthy references or data (5,6).
Case report
Patient information
A 43-year-old lactating woman presented to the Breast Clinic at Smart Health Tower (Sulaymaniyah, Iraq) with a 1-month history of pain in the left axilla and breast. An analysis of her past medical and surgical history did not reveal any notable findings. She had a history of four full-term pregnancies and a cumulative lactation period of 4 years.
Clinical examination
The clinical examination revealed a palpable, ill-defined area of hardness with a firm consistency and tenderness upon palpation. Additionally, an axillary breast with a nipple was noted (Fig. 1).
Diagnostic approach
A breast ultrasonography demonstrated bilateral axillary breast tissue, more prominent on the left side, containing two distinct heterogeneous collections, the largest measuring 36x9 mm. Mild edema, skin sinuses and non-specific axillary nodes were also observed. These findings are consistent with chronic mastitis involving axillary breast tissue (Fig. 2) (1).
Therapeutic intervention
The patient was initially diagnosed with periductal mastitis and managed medically with a tapering course of oral corticosteroids (prednisolone 10 mg once daily for 20 days, followed by 5 mg once daily for an additional 20 days; this was used to suppress the immune-mediated inflammatory process underlying GM and to reduce swelling, pain and disease activity), in combination with amoxicillin (1 g three times daily for 7 days, to cover potential secondary bacterial infection, which may complicate the course of GM, particularly when abscesses, fistulae, or skin involvement are present), cabergoline (0.5 mg once daily for 2 days, to suppress prolactin secretion) and analgesics (co-codamol 500 mg, two tablets as needed for pain control). She demonstrated a good clinical response to this regimen; however, the condition recurred 1 year later. Following multidisciplinary team discussion, a wide local excision of the left axillary tail was performed. A histopathological analysis of the excised specimen was performed on 5-µm-thick sections fixed in 10% neutral-buffered formalin for 24 h, embedded in paraffin, and stained with hematoxylin and eosin (Bio Optica Co.) for 1-2 min at room temperature. Examination under a light microscope (Leica Microsystems GmbH) revealed xanthogranulomatous inflammation involving the axillary accessory breast tissue, along with benign lymph nodes showing acute lymphadenitis (Fig. 3).
Follow-up and outcome
At the 2-month follow-up time point, the symptoms of the patient had markedly improved, with no signs of recurrence. At the most recent annual follow-up following surgical excision, she remained in good health and recurrence-free.
Discussion
Accessory breast tissue arises along the embryonic mammary ridge, extending from the axilla to the pubic region, and is susceptible to the same pathological conditions as normally located breast tissue (1). The frequently reported conditions in accessory breast tissue include cancer, mastitis, fibroadenomas, phyllodes tumors and fibrocystic changes (7). The leading hypothesis regarding the pathogenesis of GM suggests that an autoimmune response is initiated within the lobules of the breast parenchyma following ductal injury. This triggers a localized inflammatory reaction in the connective tissue, promoting the recruitment of macrophages and lymphocytes, ultimately resulting in a noncaseating granulomatous response (3).
The influence of ethnicity on GM remains a subject of debate. Vall et al (3) reported no specific ethnic predisposition. By contrast, the studies by Yuan et al (8) and Deng et al (9) indicated a higher prevalence of GM in Middle Eastern populations compared to Western countries. Consistent with the present case, GM predominantly affects women of reproductive age, particularly those with a history of breastfeeding. Among the 7 cases reviewed herein, 4 patients had a prior history of breastfeeding, with an average duration of 22.7 months (Table I) (1-4,7,10,11). However, Nakamura et al (7) and Rajendran et al (10) documented cases of GM in women without a history of breastfeeding.
Bilateral involvement in GM is rare, as the condition typically presents unilaterally (1). In the patient in the present study, a breast ultrasonography identified two distinct heterogeneous collections within the left axillary breast, accompanied by mild edema and skin sinuses. These imaging findings were consistent with the characteristic manifestations of GM, which commonly include mass formation, skin changes and the development of a sinus tract. Systemic symptoms, such as fever, remain uncommon in GM cases (1). Among the cases reviewed herein, all were unilateral, with fever reported in only 1 patient. Pain was the reported symptom in 6 cases, whereas erythema was observed in only 2 cases.
The diagnosis of GM requires a well-coordinated multidisciplinary approach involving clinicians, radiologists and pathologists, as demonstrated in the present case report. This is particularly critical given that cases with clinical deviance or coexistence with breast cancer have been reported, increasing the risk of misdiagnosis. Multidisciplinary collaboration not only helps to avoid such errors, but also facilitates earlier preoperative diagnosis and ensures the appropriate use of corticosteroid therapy in selected patients (8,12). Due to the absence of specific clinical or radiological characteristics, imaging findings may be non-specific. Mammography often reveals asymmetric density, while an ultrasound may detect irregular, heterogeneous masses suggestive of abscesses. However, these features are not unique to GM and can mimic other breast pathologies (1).
Although no standardized treatment exists for GM to date, at least to the best of our knowledge, steroids are frequently used to reduce lesion size. However, their use is associated with adverse effects, such as weight gain, hyperglycemia, Cushing syndrome and opportunistic infections (7). Additionally, patient non-adherence can compromise treatment efficacy. Vall et al (3) reported a case in which poor adherence led to multiple recurrences, ultimately necessitating rescue therapy. While the studies by Alvand et al (2) Rajendran et al (10) and Oze et al (4) reported favorable outcomes with conservative management, the lack of long-term follow-up in these cases raises concerns about the sustained efficacy and reliability of conservative treatment strategies.
A previous meta-analysis of 138 cases undergoing surgery and 358 cases with steroid therapy revealed improved outcomes with surgery (complete response: 90.6 vs. 71.8%; recurrence: 6.8% vs. 20.9%) (13). Combining surgery with steroids further improved results, with a 94.5% complete response rate and a 4.0% recurrence rate (13). A conservative approach was initially employed for the patient in the present study; however, recurrence occurred after 1 year. By contrast, wide local excision of the axillary tail achieved a favorable outcome, with no recurrence observed at the one-year follow-up.
The case described herein enriches the existing body of knowledge by elucidating the presentation, complex diagnosis, treatment options and favorable outcomes of GM in accessory breast tissue, guiding clinicians in recognizing and managing this rare condition effectively. However, it is worth mentioning that a longer period of monitoring would strengthen this report and the conclusions drawn significantly.
In conclusion, GM can occur in accessory breast tissue. While corticosteroids may provide favorable short-term results, they do not necessarily prevent recurrence, whereas surgical management may offer more durable long-term outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Salih AM Pshtiwan LR Latif S Ali HO Abdullah AM Baba HO Hama JI Hassan SH Hassan MN Mohammed SH Granulomatous mastitis in accessory breast tissue: A rare presentation and surgical management Biomed Rep 2062202410.3892/br.2024.175038476604 PMC 10928478 · doi ↗ · pubmed ↗
- 2Alvand S Hessami A Kiani L Makhmalbaf AO Elahi A Uncommon location of idiopathic granulomatous mastitis: A case report: Uncommon Location of IGM Arch Breast Cancer 93203242022
- 3Vall E Araya V Tortajada L Escobedo V Nogueiras R Del Riego J Idiopathic granulomatous mastitis after m RNA vaccination against COVID-19: A possible association?BJR Case Rep 11uaae 048202510.1093/bjrcr/uaae 04839995498 PMC 11849954 · doi ↗ · pubmed ↗
- 4Oze KR Yehouenou Tessi RT Mendes P Allali N Chat L El Haddad S Granulomatous mastitis: A case report SAGE Open Med Case Rep 102050313 X 221146671202210.1177/2050313 X 22114667136582424 PMC 9793057 · doi ↗ · pubmed ↗
- 5Abdullah HO Abdalla BA Kakamad FH Ahmed JO Baba HO Hassan MN Bapir R Rahim HM Omar DA Kakamad SH Predatory publishing lists: A review on the ongoing battle against fraudulent actions Barw Med J 226302024
- 6Prasad S Nassar M Azzam AY García-Muro-San JoséF Jamee M Sliman RKA Evola G Mustafa AM Abdullah HO Abdalla BA Ca Re L Guidelines: A consensus-based guideline on case reports and literature review (Ca Re L)Barw Med J 213192024
- 7Nakamura J Tanaka F Ohtaka K Sato K Iyama AA rare case of granulomatous mastitis in the accessory axillary breast of a pregnant woman successfully treated by surgery Eur J Breast Health 18195202210.4274/ejbh.galenos.2021.2021-10-535445183 PMC 8987857 · doi ↗ · pubmed ↗
- 8Yuan QQ Xiao SY Farouk O Du YT Sheybani F Tan QT Akbulut S Cetin K Alikhassi A Yaghan RJ Management of granulomatous lobular mastitis: An international multidisciplinary consensus (2021 edition)Mil Med Res 920202210.1186/s 40779-022-00380-535473758 PMC 9040252 · doi ↗ · pubmed ↗