Clarifying the Spectrum of Gallbladder Haemorrhage: A Systematic Review of Haemorrhagic Cholecystitis and Haemorrhagic Gallbladder
Evangelia Florou, Shirin Ubaid, Carol Balasingh, Parthi Srinivasan, Andreas Prachalias

TL;DR
This review clarifies the distinction between haemorrhagic cholecystitis and haemorrhagic gallbladder, highlighting their clinical differences and recommending a severity-based treatment approach.
Contribution
The paper introduces a stratified management framework for gallbladder haemorrhage based on clinical severity and treatment urgency.
Findings
Most cases (73.8%) were classified as haemorrhagic gallbladder due to haemodynamic instability.
Overall mortality was 10.8%, with anticoagulation reported in nearly half of the cases.
Multimodal treatment was most common, followed by urgent open and laparoscopic cholecystectomy.
Abstract
Haemorrhagic cholecystitis (HC) and haemorrhagic gallbladder (HGB) refer to rare clinical entities characterised by bleeding originating from the gallbladder. These terms are often used interchangeably in literature to describe a spectrum of presentations, ranging from incidental findings to life-threatening haemorrhage and shock. Reported cases are scarce and primarily limited to case reports and small series. Clinical presentation and management vary significantly, from conservative antibiotic therapy to urgent surgical intervention. This systematic review aims to summarise the published clinical experience, clarify terminology use, and propose a stratified management approach based on presentation severity. A systematic review of the literature was conducted in accordance with PRISMA guidelines, covering publications from January 2019 to May 2025. PubMed, Embase, Medline, and Google…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
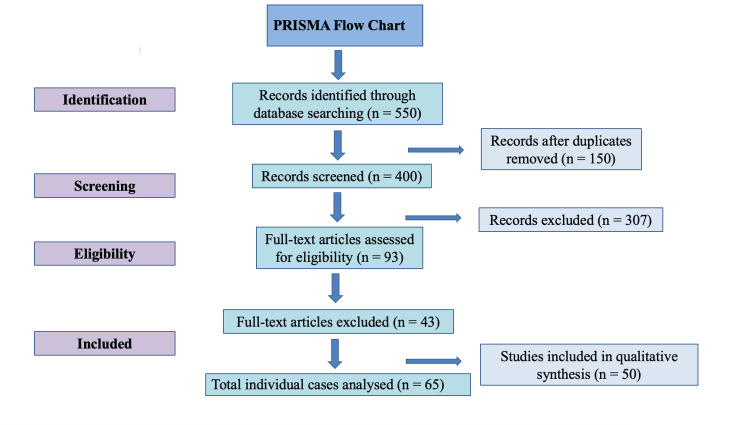 Figure 1
Figure 1| Treatment Type | Count | Percentage |
| Multimodal treatment* | 20 | 30.8 |
| Urgent open cholecystectomy | 17 | 26.2 |
| Urgent laparoscopic cholecystectomy | 12 | 18.5 |
| Cholecystostomy | 5 | 7.7 |
| Elective cholecystectomy | 4 | 6.2 |
| Embolization | 2 | 3.1 |
| Conservative, antibiotics | 3 | 4.6 |
| PTBD | 1 | 1.5 |
| ERCP | 1 | 1.5 |
| First author | Year of publication | Title | Number of cases | Gender | Age | Bgx liver disease | Typical symptoms | Jaundice | GI bleed | Haemorrhagic shock | Treatment | Transfusion | Death | HC or HGB |
| Louis M et al. [ | 2024 | Management of NSAID-Induced Penetrating Gastric Ulcer Complicated by Hemorrhagic Cholecystitis: The Role of Percutaneous Transhepatic Biliary Drainage | 1 | F | 68 | No | Yes | No | No | No | PTBD | NS | No | HC |
| AlMoshary M et al. [ | 2024 | Hemorrhagic cholecystitis afflicted with glanzmann thrombasthenia patient | 1 | M | 27 | No | Yes | Yes | No | No | urgent laparoscopic cholecystectomy | NS | No | HC |
| Diaz V et al. [ | 2024 | Hemorrhagic Cholecystitis Due to Rupture of Underlying Anomalous Duplicated Cystic Arteries | 1 | M | 33 | Yes | Yes | No | Yes | No | embolization | Yes | No | HGB |
| Harrison N et al. [ | 2023 | Haemorrhagic cholecystitis in a young patient, complicated by gallbladder perforation and choledocholithiasis | 1 | F | 43 | No | Yes | No | Yes | No | conservative, antibiotics | No | No | HC |
| Omura T et al. [ | 2023 | Acute hemorrhagic cholecystitis related to diffuse neurofibroma of gallbladder in a patient with neurofibromatosis type 1 | 1 | M | 46 | No | Yes | No | No | No | urgent open cholecystectomy | Yes | No | HGB |
| Morrow J et al. [ | 2023 | Haemorrhagic cholecystitis treated with endovascular embolization | 1 | F | 52 | No | Yes | No | No | Yes | embolization | Yes | No | HGB |
| Cochran R et al. [ | 2022 | COVID-19 associated spontaneous hemorrhagic cholecystitis | 1 | M | 67 | Yes | Yes | No | No | Yes | cholecystostomy | No | No | HGB |
| Karaisli S et al. [ | 2022 | Perforated hemorrhagic cholecystitis in a patient with Bernard–Soulier syndrome | 1 | M | 57 | No | Yes | No | No | No | urgent open cholecystectomy | Yes | Yes | HGB |
| Natcher P et al. [ | 2022 | Mirizzi Syndrome in the Setting of Hemorrhagic Cholecystitis | 1 | M | 75 | No | Yes | No | No | No | cholecystostomy | NS | No | HC |
| Aldohayan N et al. [ | 2021 | Hemorrhagic cholecystitis with auto-avulsion | 1 | F | 74 | No | Yes | No | No | No | urgent open cholecystectomy | NS | No | HGB |
| Hotak M et al. [ | 2021 | A case of haemorrhagic cholecystitis with no risk factors | 1 | F | 51 | No | Yes | No | No | No | urgent laparoscopic cholecystectomy | NS | No | HC |
| Liao TK et al. [ | 2020 | Idiopathic Intrahepatic Artery Aneurysm Presenting as Acute Hemorrhagic Cholecystitis | 1 | F | 20 | No | Yes | No | No | No | multimodal treatment | No | No | HGB |
| Long N et al. [ | 2021 | Point-of-care ultrasonography in the diagnosis of hemorrhagic cholecystitis | 1 | M | 81 | No | Yes | No | No | No | ERCP | NS | No | HC |
| Rahesh J et al. [ | 2021 | Atraumatic spontaneous hemorrhagic cholecystitis | 1 | F | 65 | No | Yes | No | No | No | urgent laparoscopic cholecystectomy | NS | No | HGB |
| Nitta T et al. [ | 2021 | Emergency laparoscopic cholecystectomy for hemorrhagic cholecystitis: A case report | 1 | M | 64 | No | Yes | No | No | No | urgent laparoscopic cholecystectomy | NS | No | HC |
| Leaning M et al. [ | 2021 | Acalculous hemorrhagic cholecystitis | 1 | M | 73 | No | Yes | No | No | No | urgent laparoscopic cholecystectomy | NS | No | HC |
| Sakharuk I et al. [ | 2021 | Anticoagulant-induced hemorrhagic cholecystitis with hemobilia after deceased donor kidney transplant and literature review | 1 | M | 55 | No | Yes | No | No | No | urgent open cholecystectomy | NS | No | HGB |
| Lan X et al. [ | 2019 | Massive hemoperitoneum and upper GI hemorrhage following liver rupture secondary to GB perforation | 1 | M | 53 | No | Yes | No | Yes | No | urgent open cholecystectomy | NS | No | HGB |
| Pickell Z et al. [ | 2021 | Acute hemorrhagic cholecystitis with gallbladder rupture and massive intra0abdominal hemorrhage | 1 | M | 67 | No | Yes | No | Yes | No | urgent open cholecystectomy | Yes | No | HGB |
| Staszak J et al. [ | 2019 | cholecystitis and hemobilia | 1 | M | 43 | No | Yes | No | Yes | No | multimodal treatment | NS | No | HGB |
| Ardu M et al. [ | 2020 | Hemoperitoneum from Hemorrhagic Perforated Cholecystitis in a Patient with Acquired Deficiency of Factor VIII | 1 | M | 79 | No | Yes | No | No | No | urgent open cholecystectomy | Yes | No | HGB |
| Zhang X et al. [ | 2020 | Hemorrhagic cholecystitis with rare imaging presentation: a case report and a lesson learned from neglected medication history of NSAIDs | 1 | F | 57 | No | Yes | No | No | No | elective cholecystectomy | NS | No | HGB |
| Yam M et al. [ | 2020 | A 51-year-old female presenting with shock due to hemorrhagic cholecystitis | 1 | F | 51 | No | Yes | No | No | Yes | multimodal treatment | NS | No | HGB |
| Chen X et al. [ | 2020 | A haemorrhagic cholecystitis presenting as obstructive jaundice | 1 | F | 63 | No | Yes | Yes | No | No | multimodal treatment | NS | No | HGB |
| Bergeron E et al. [ | 2019 | Massively distended, necrotic and hemorrhagic gallbladder in a long-term octreotide-treated patient with added everolimus | 1 | F | 63 | No | Yes | Yes | No | No | multimodal treatment | NS | No | HGB |
| Donn et al. [ | 2019 | Hemorrhagic Cholecystitis after Warfarin Use for Deep Vein Thrombosis | 1 | M | 63 | No | Yes | No | No | No | multimodal treatment | Yes | No | HGB |
| Ng Z et al. [ | 2019 | Haemorrhagic cholecystitis: a rare entity not to be forgotten | 1 | F | 68 | No | Yes | No | No | Yes | urgent open cholecystectomy | NS | No | HGB |
| Lauria A et al. [ | 2019 | Hemorrhagic Cholecystitis: An Uncommon Disease Resulting in Hemorrhagic Shock | 1 | M | 73 | Yes | Yes | No | Yes | No | urgent open cholecystectomy | Yes | Yes | HGB |
| Jiang et al. [ | 2020 | Hemorrhagic Cholecystitis | 1 | M | 68 | No | Yes | No | No | Yes | urgent open cholecystectomy | Yes | Yes | HGB |
| Cirillo B et al. [ | 2020 | Acalculous hemorrhagic cholecystitis and SARS - CoV-2 infection | 1 | M | 79 | No | Yes | No | No | No | urgent laparoscopic cholecystectomy | NS | No | HGB |
| Eduardo S et al. [ | 2024 | Hemorrhagic cholecystitis. A challenge for the general surgeon | 1 | M | 35 | No | Yes | No | No | No | urgent open cholecystectomy | NS | No | HGB |
| Gobishangar S et al. [ | 2021 | Hemorrhagic cholecystitis: A rare cause of melena | 1 | F | 75 | No | Yes | Yes | Yes | No | elective cholecystectomy | Yes | No | HC |
| Anouassi Z et al. [ | 2023 | A case of haemorrhagic cholecystitis in a patient on apixaban after covid 19 infection | 1 | M | 67 | No | Yes | Yes | No | No | conservative , abx | Yes | No | HGB |
| Arscott T et al. [ | 2024 | Hemorrhagic cholecystitis: A case report | 1 | M | 69 | No | Yes | No | No | No | urgent laparoscopic cholecystectomy | NS | No | HC |
| Khoury G et al. [ | 2019 | An intraoperatively diagnosed case of hemorrhagic cholecystitis in a 43 year old patient: case report | 1 | F | 43 | No | Yes | No | No | No | urgent laparoscopic cholecystectomy | NS | No | HC |
| Hasegawa T et al. [ | 2021 | A case of hemorrhagic cholecystitis and hemobilia under anticoagulation therapy | 1 | M | 70 | No | Yes | Yes | No | No | multimodal treatment | NS | No | HGB |
| Torrico CP et al. [ | 2024 | Severe hemorrhagic cholecystitis in the absence of common predisposing factors | 1 | M | 70 | No | Yes | No | No | No | urgent open cholecystectomy | NS | No | HGB |
| Espejo N et al. [ | 2024 | Hemorrhagic Cholecystitis: the forgotten differential diagnosis | 1 | M | 59 | No | Yes | No | Yes | No | multimodal treatment | Yes | No | HGB |
| Tarazi M et al. [ | 2019 | literature review and case series of haemorrhagic cholecystitis 1 | 1 | M | 87 | No | Yes | No | No | No | cholecystostomy | NS | No | HC |
| Tarazi M et al. [ | 2019 | literature review and case series of haemorrhagic cholecystitis 2 | 1 | F | 65 | No | Yes | No | No | No | conservative , abx | NS | No | HC |
| Tarazi M et al. [ | 2019 | literature review and case series of haemorrhagic cholecystitis 3 | 1 | F | 92 | No | Yes | No | No | No | cholecystostomy | NS | No | HC |
| Baier A et al.[ | 2022 | Emergent laparoscopic surgical intervention for perforated hemorrhagic cholecystitis with hemodynamic instability 1 | 1 | M | 74 | No | Yes | No | No | No | urgent laparoscopic cholecystectomy | Yes | No | HGB |
| Baier A et al. [ | 2022 | Emergent laparoscopic surgical intervention for perforated hemorrhagic cholecystitis with hemodynamic instability 2 | 1 | M | 69 | No | Yes | No | Yes | No | urgent laparoscopic cholecystectomy | Yes | No | HGB |
| Baier A et al. [ | 2022 | Emergent laparoscopic surgical intervention for perforated hemorrhagic cholecystitis with hemodynamic instability 3 | 1 | F | 23 | Yes | Yes | No | No | Yes | urgent laparoscopic cholecystectomy | Yes | No | HGB |
| Chernopolsky PM et al. [ | 2024 | Hemorrhagic cholecystitis - two cases and literature review 1 | 1 | F | 68 | No | Yes | Yes | No | No | urgent open cholecystectomy | NS | No | HGB |
| Chernopolsky PM et al. [ | 2024 | Hemorrhagic cholecystitis - two cases and literature review 2 | 1 | M | 76 | No | Yes | No | No | No | urgent open cholecystectomy | NS | No | HGB |
| Kim HC et al. [ | 2023 | patient 1 out of 10 Transcatheter arterial embolization of cystic artery bleeding | 1 | M | 43 | Yes | No | No | No | No | multimodal treatment | NS | No | HGB |
| Kim HC et al. [ | 2023 | patient 2 out of 10 Transcatheter arterial embolization of cystic artery bleeding | 1 | F | 49 | Yes | No | No | Yes | No | multimodal treatment | NS | Yes | HGB |
| Kim HC et al. [ | 2023 | patient 3 out of 10 Transcatheter arterial embolization of cystic artery bleeding | 1 | M | 75 | No | No | No | Yes | No | multimodal treatment | NS | No | HGB |
| Kim HC et al. [ | 2023 | patient 4 out of 10 Transcatheter arterial embolization of cystic artery bleeding | 1 | M | 74 | No | Yes | No | Yes | No | multimodal treatment | NS | Yes | HGB |
| Kim HC et al. [ | 2023 | patient 5 out of 10 Transcatheter arterial embolization of cystic artery bleeding | 1 | M | 48 | No | Yes | No | Yes | No | multimodal treatment | NS | Yes | HGB |
| Kim HC et al. [ | 2023 | patient 6 out of 10 Transcatheter arterial embolization of cystic artery bleeding | 1 | F | 78 | No | Yes | No | Yes | No | multimodal treatment | NS | No | HGB |
| Kim HC et al. [ | 2023 | patient 7 out of 10 Transcatheter arterial embolization of cystic artery bleeding | 1 | M | 78 | No | Yes | No | No | No | multimodal treatment | NS | No | HGB |
| Kim HC et al. [ | 2023 | patient 8 out of 10 Transcatheter arterial embolization of cystic artery bleeding | 1 | M | 64 | No | Yes | No | Yes | No | multimodal treatment | NS | No | HGB |
| Kim HC et al. [ | 2023 | patient 9 out of 10 Transcatheter arterial embolization of cystic artery bleeding | 1 | M | 80 | Yes | No | No | Yes | No | multimodal treatment | NS | Yes | HGB |
| Kim HC et al. [ | 2023 | patient 10 out of 10 Transcatheter arterial embolization of cystic artery bleeding | 1 | M | 80 | No | No | No | Yes | No | multimodal treatment | NS | No | HGB |
| Florou E et al. [ | 2025 | hemorrhagic GB on BGx of PSC | 1 | F | 29 | Yes | Yes | Yes | No | Yes | urgent open cholecystectomy | Yes | No | HGB |
| Sweeney A et al. [ | 2019 | Hemorrhagic cholecystitis causing hemobilia and common bile duct obstruction | 1 | M | 78 | No | Yes | Yes | No | No | elective cholecystectomy | No | No | HC |
| Reens D et al. [ | 2019 | Hemorrhagic cholecystitis: A case of expecdited diagnosis by point -of -care ultrasound in the emergency department | 1 | M | 76 | No | Yes | No | No | No | cholecystostomy | NS | No | HC |
| Shah R et al. [ | 2020 | Hemorrhagic Cholecystitis in a Patient with Cirrhosis and Rectal Cancer | 1 | M | 66 | Yes | Yes | No | Yes | Yes | urgent laparoscopic cholecystectomy | Yes | No | HGB |
| Nguyen D et al. [ | 2021 | Acute Hemorrhagic Cholecystitis with Large Hemoperitoneum: Treatment with Microcoil Embolization and Subsequent Cholecystectomy 1 | 1 | M | 74 | No | No | Yes | No | Yes | multimodal treatment | NS | No | HGB |
| Nguyen D et al. [ | 2021 | Acute Hemorrhagic Cholecystitis with Large Hemoperitoneum: Treatment with Microcoil Embolization and Subsequent Cholecystectomy 2 | 1 | M | 74 | No | No | No | No | Yes | multimodal treatment | Yes | No | HGB |
| Ma Z et al. [ | 2019 | Anticoagulants is a risk factor for spontaneous rupture and hemorrhage of gallbladder: a case report and literature review | 1 | F | 51 | No | Yes | No | No | Yes | urgent open cholecystectomy | NS | No | HGB |
| Itagaki H et al. [ | 2019 | Gallbladder hemorrhage during orally administered edoxaban therapy: a case report | 1 | F | 86 | No | No | No | Yes | No | elective cholecystectomy | NS | No | HC |
| Azam M et al. [ | 2021 | It's the Bloody Gallbladder! Spontaneous Gallbladder Hemorrhage Following Factor Xa Inhibition | 1 | M | 55 | No | Yes | No | No | No | urgent open cholecystectomy | NS | No | HGB |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Gastrointestinal Bleeding Diagnosis and Treatment · Pancreatitis Pathology and Treatment
Introduction and background
Haemorrhagic cholecystitis (HC) and haemorrhagic gallbladder (HGB) are rare but potentially life-threatening conditions involving bleeding within or from the gallbladder. Although often used interchangeably, these terms likely describe different stages of a clinical spectrum, from intraluminal bleeding secondary to haemorrhagic inflammation to more advanced presentations such as gallbladder rupture and hemoperitoneum. Due to their low incidence, most available evidence consists of isolated case reports and small series, limiting the ability to define standardised diagnostic or management pathways [1-3].
Presentations range from non-specific symptoms such as abdominal pain or anaemia to more severe findings, including jaundice, gastrointestinal bleeding, and haemorrhagic shock. Reported management strategies vary accordingly, from conservative therapy to embolisation or urgent surgical intervention [4-6]. In a recent systematic review, Tarazi et al. examined the published literature and emphasised the inconsistent use of terminology and treatment indications. They proposed that classification based on haemodynamic stability and imaging features may help guide appropriate intervention [7].
Building on that concept, this review systematically evaluates the literature from 2019 to 2024 and retrospectively stratifies reported cases into HC or HGB based on clinical parameters such as haemodynamic status, transfusion requirement, haemoglobin drop, and timing of intervention. The objective is to clarify terminology use, assess consistency in reporting, and propose a severity-based management framework for this rare condition.
Review
Materials and methods
A systematic literature review was conducted in accordance with PRISMA 2020 guidelines. A comprehensive search of PubMed, Embase, Medline, and Google Scholar was performed to identify relevant studies published between January 2019 and May 2025. The search terms included “haemorrhagic cholecystitis”, “haemorrhagic gallbladder”, “gallbladder rupture”, and “haemorrhagic shock and gallbladder rupture”. Only English-language publications reporting clinical cases of gallbladder-origin haemorrhage were included. Eligible studies comprised case reports, case series, and retrospective reviews with extractable patient-level data. Articles were excluded if they lacked clinical detail, described purely histological findings without clinical correlation, or presented aggregated data that could not be stratified. This systematic review was not prospectively registered in a publicly accessible database.
To avoid duplication and maintain relevance to current practice, studies summarised in the pre-2019 systematic review by Tarazi et al. were not re-analysed [7]. Extracted variables included patient demographics, background use of anticoagulants and non-steroidal anti-inflammatory drugs (NSAIDs), presence of gallstones, presenting symptoms, haemoglobin drop, transfusion requirement, treatment modality, and reported mortality.
Treatment strategies were categorised using a 12-point classification system (e.g., conservative management, elective or emergency surgery, interventional radiology, or multimodal approaches). Cases were stratified as haemorrhagic cholecystitis (HC) if patients were haemodynamically stable and managed conservatively, semi-electively, or electively, and as haemorrhagic gallbladder (HGB) if patients were unstable or required urgent or multimodal intervention. Descriptive statistics were used to summarise the findings. Cases with incomplete stratification data were reviewed by two authors and categorised by consensus.
Results
Fifty publications were included in this review, reporting a total of 65 individual cases. Two case series that were excluded need to be mentioned: one due to reliance solely on imaging findings with key clinical variables (e.g., symptoms, haemodynamic status, treatment, and outcomes) inconsistently reported or missing; and the second because cases were identified from histological diagnoses without clinical correlation or documentation of treatment urgency.
Of the 65 patients analysed, 23 were females and 42 males, yielding a female-to-male ratio of approximately 1:1.8. The median age was 67 years, ranging from 20 to 92 years.
Anticoagulation therapy was identified as a potential risk factor in 31 cases (47.7%), while non-steroidal anti-inflammatory drug (NSAID) use was noted in three patients (4.6%). Comorbidities were frequent and often multisystemic. From a cardiovascular perspective, 22 patients (33.8%) had coronary artery disease, atrial fibrillation, or heart failure; cerebrovascular disease, including prior strokes or transient ischaemic attacks, was present in seven cases (10.8%). Renal dysfunction was documented in 13 patients (20.0%), including those with chronic kidney disease and end-stage renal disease. Malignancies were reported in four patients (6.2%), while three patients (4.6%) had a history of solid organ transplantation. Background liver disease, including cirrhosis and portal hypertension, was identified in eight patients (12.3%), and systemic or metabolic conditions such as diabetes, autoimmune disease, or sarcoidosis were seen in 26 cases (40.0%).
Clinical presentation was dominated by typical symptoms such as right upper quadrant pain, vomiting, fever, or a combination of them, reported in 57 cases (87.7%). Jaundice was present in 10 patients (15.4%), while gastrointestinal bleeding occurred in 19 cases (29.2%). Haemorrhagic shock, reflecting the most severe end of the clinical spectrum, developed in 11 patients (16.9%). Notably, many of these patients initially presented with typical or atypical symptoms but progressed to haemodynamic instability during hospitalisation and early treatment. A drop in haemoglobin and/or transfusion requirement was documented in 24 patients (36.9%) and 18 patients (27.7%), respectively, although this information was not consistently reported in all cases.
A wide range of treatments was applied and are summarised in Table 1. Conservative management with antibiotics alone was used in three patients (4.6%), elective cholecystectomy in four cases (6.2%), cystic artery embolisation alone in two (3.1%), and percutaneous cholecystostomy in five cases (7.7%). Percutaneous transhepatic biliary drainage (PTBD) and endoscopic retrograde cholangiopancreatography (ERCP) were used as sole interventions in one case each (1.5%), though they were more often part of a broader multimodal plan. Urgent laparoscopic and urgent open cholecystectomies were performed in 12 (18.5%) and 17 (26.2%) patients, respectively. The most common approach was a multimodal strategy combining interventional radiology or endoscopy with surgery for gallbladder resection, applied in 20 patients (30.8%). Overall, seven patients (10.8%) died, while 58 (89.2%) survived. Gallstones were documented in 25 patients (38.5%), absent in 30 (46.2%), and not reported in 10 cases (15.4%).
HC/HGB stratification
Cases were stratified as haemorrhagic cholecystitis (HC) or haemorrhagic gallbladder (HGB) based on clinical severity, haemodynamic status, and treatment approach. HC was defined by haemodynamic stability and non-urgent treatment, including conservative management, semi-elective or elective cholecystectomy, cholecystostomy, PTBD, or ERCP. These patients typically did not exhibit a haemoglobin drop or require transfusion. In contrast, HGB was characterised by haemodynamic compromise, the presence of shock or gastrointestinal bleeding, a documented drop in haemoglobin or transfusion requirement, and the need for urgent intervention such as embolisation, laparotomy, or a multimodal approach combining surgical and radiological management. Among the 65 analysed cases, 48 (73.8%) were classified as HGB and 17 (26.2%) as HC.
In accordance with PRISMA guidelines, a flowchart (Figure 1) and summarised table of all included studies with key clinical and methodological parameters are provided (Table 2).
PRISMA flowchartThe initial 550 records were retrieved from PubMed, Embase, Medline, and Google Scholar using the terms “haemorrhagic cholecystitis”, “haemorrhagic gallbladder”, “gallbladder rupture”, and “haemorrhagic shock and gallbladder rupture”. After deduplication, 400 records were screened. Forty-three full-text articles were excluded due to lack of extractable clinical data (n = 21), histological-only reports without clinical correlation (n = 14), or duplicate/overlapping cases (n = 8).
Discussion
HC and HGB are terms often used interchangeably to describe the rare clinical scenario of bleeding originating from the gallbladder. The condition is known to represent a rare complication in the context of cholecystitis; however, it has been primarily documented through isolated case reports and small series, contributing to the lack of standardised diagnostic and management protocols [1,2,49].
In their literature review, Tarazi et al. analysed 31 cases reported between 1985 and 2018, identifying anticoagulation therapy as the most common risk factor, present in 45% of patients. Interestingly, an equal proportion (45%) were not receiving anticoagulation, and in 10% of cases, anticoagulation status was not reported [7]. These findings partially align with those of the present review, in which anticoagulation was identified in 47.7% of cases. This substantial proportion highlights a strong association, though not necessarily causation [7,33]. A retrospective study further demonstrated that although anticoagulated patients undergoing cholecystectomy experienced increased intraoperative blood loss and transfusion requirements, their postoperative outcomes were not significantly worse compared to non-anticoagulated counterparts [57]. These findings collectively support the interpretation that anticoagulation likely functions as a risk-enhancing cofactor in haemorrhagic gallbladder pathology, particularly when mucosal integrity is compromised, a fact that can be encountered in both acute and chronic cholecystitis settings.
Other potential contributors identified included chronic renal failure, haemophilia, vasculitic disorders, steroid use, and advanced age. While Tarazi et al. highlighted the potential contribution of systemic illness, the broader dataset in this review reinforces the multifactorial nature of haemorrhagic gallbladder pathology and its strong association with comorbidities [7]. Notably, 47.7% of patients who developed HGB had more than one underlying systemic illness. These findings underscore the need for risk-based stratification and heightened clinical vigilance, particularly in vulnerable patient populations.
While classic symptoms such as right upper quadrant pain, vomiting, and fever were observed in 89.2% of cases, less typical features like jaundice (15.4%) and gastrointestinal bleeding (29.2%) were also reported. These atypical signs may appear concurrently or sequentially, potentially delaying diagnosis.
Jaundice is likely a result of haemobilia obstructing the biliary tract, and if unrecognised, gastrointestinal bleeding may become the next evident clinical manifestation. On the contrary, diagnosis is more challenging when patients present with GI bleeding and, in the absence of common symptoms, work-ups fail to direct clinicians to identify that the cause of bleeding is haemobilia [58].
Haemobilia refers to bleeding into the biliary tree, typically resulting from vascular erosion, trauma, inflammation, or tumour invasion. When blood enters the common bile duct, it can obstruct biliary flow, resulting in biochemical evidence of cholestasis. This manifests as an obstructive pattern on liver function tests, including elevated bilirubin, alkaline phosphatase, and gamma-glutamyl transferase levels. Clinically, this may present as jaundice, often in the absence of gallstones or malignancy [59,60].
Gallstones were documented in 38.5% of cases, while 46.2% had no evidence of cholelithiasis, and 15.4% lacked documentation. Notably, gallstones were present across both HC and HGB categories, without a clear trend correlating their presence to severity. This suggests that gallstones, while common, are not essential for the development of haemorrhagic manifestations. When stratified by clinical severity, gallstones were found in 10 out of 15 HC cases (66.7%), but in only 15 of 50 HGB cases (30%). This suggests that gallstones may be more commonly associated with stable, less severe presentations of gallbladder haemorrhage, whereas HGB is more often observed in the absence of gallstones. These findings imply that gallstone-related inflammation might trigger haemorrhage in HC, while HGB likely reflects alternative mechanisms such as chronic cholecystitis, mucosal ischaemia, vascular compromise, or anticoagulation-related bleeding.
The above findings reflect the pathophysiological mechanisms of acute cholecystitis known so far. Acute cholecystitis begins with cystic duct obstruction, most commonly due to gallstones, which leads to bile stasis and elevated intraluminal pressure in the gallbladder [61]. This increased pressure causes venous congestion and mucosal oedema, reducing blood flow and precipitating mucosal ischaemia and necrosis [61,62]. Histologically, the gallbladder wall shows inflammation, oedema, vascular congestion, haemorrhage, neutrophilic infiltration, and focal mucosal necrosis [62]. Continued ischaemia may progress to gangrene and perforation, sometimes accompanied by bacterial invasion from organisms, which exacerbates transmural inflammation [63]. In acalculous cholecystitis, particularly in critically ill patients, hypoperfusion rather than stone obstruction is the primary driver of ischaemic injury, leading to similar histopathological findings [62,63]. Overall, acute cholecystitis can occur in both settings, with or without gallstones.
In the context of haemorrhagic cholecystitis, transmural inflammation with or without vascular compromise of the gallbladder wall can lead to intraluminal bleeding that extends into the cystic duct and biliary tree, manifesting as obstructive jaundice [61,65-66]. The pathophysiological mechanisms underlying this process, particularly in the setting of recent or ongoing anticoagulation or in the presence of systemic disease, remain poorly understood. However, literature suggests that intracystic bleeding may be triggered by ischaemia due to increased intraluminal pressure and compromised perfusion, possibly exacerbated by anticoagulants, trauma, or systemic illness [31,36,52]. Histopathologically, the gallbladder wall demonstrates oedema, vascular congestion, subserosal haemorrhage, neutrophilic infiltration, mucosal necrosis, and full-thickness necrosis or infarction have also been documented [17,67]. A small subset of patients presenting with such atypical features rapidly progressed to haemorrhagic shock, representing the most severe end of the clinical spectrum [52]. These findings, along with the occurrence of haemodynamic compromise, haemoglobin drop, or transfusion requirement in a substantial proportion of cases, support once again the rationale for stratifying presentations into haemorrhagic cholecystitis (HC) and HGB.
In our review, treatment approaches were notably heterogeneous, reflecting both the clinical severity of presentation and the anatomical complexity encountered. Tarazi et al. reported cholecystectomy as the predominant treatment modality, performed in 71% of the 31 cases reviewed, with only a small proportion managed conservatively or by cholecystostomy [7]. In contrast, our review identified a broader therapeutic landscape. While urgent cholecystectomy (laparoscopic or open) was undertaken in 44% of cases, the most frequently reported intervention was a multimodal approach, combining interventional radiology, endoscopy, and/or surgery, used in 30.5% of patients. Additionally, less common but significant interventions such as cystic artery embolisation (3.4%), elective cholecystectomy (3.4%), and percutaneous techniques like PTC (1.7%) or ERCP (1.7%) highlight the nuanced, case-specific nature of treatment. Conservative management with antibiotics alone was rare (5.1%) and limited to haemodynamically stable individuals.
These findings show the variability in management approaches, which were primarily guided by the patient’s clinical status.
The differences in treatment trends between studies likely reflect the absence of a symptom-based stratification model to guide management and show inconsistencies in the reporting and documentation of haemorrhagic cholecystitis across the literature, potentially contributing to an underestimation of its true severity.
Stratification may enhance diagnostic suspicion when common symptoms suggestive of gallbladder pathology are accompanied by more serious or unusual clinical features. It can also help guide the urgency and nature of clinical interventions, accounting for patient-specific factors such as age, baseline functional status, and comorbidities.
Supportive of our suggestion of the need for a stratified approach to haemorrhagic gallbladder pathology is the large retrospective study by Hotak et al., which reviewed 35 cases of histologically confirmed haemorrhagic cholecystitis identified from over 6400 cholecystectomy specimens [68]. Notably, only 5.7% of patients were on anticoagulation therapy, and nearly 89% underwent laparoscopic cholecystectomy, indicating a stable preoperative clinical status in the majority. While their cohort adds epidemiological weight to the incidence of HC (0.55%), it provides limited insight into clinical urgency, haemodynamic compromise, or symptom severity, as the diagnosis was made histologically post-resection. Furthermore, the inclusion of predominantly elective or emergency cholecystectomy specimens, with all patients surviving without complication, reinforces the view that not all haemorrhagic findings carry acute clinical significance. This highlights the value of a clinical classification into HC and HGB, particularly in guiding decision-making when haemorrhage is suspected preoperatively, based on atypical presentations or physiological instability. This study was excluded from the final cohort of studies analysed in our review due to its reliance on histopathological diagnosis alone, with a lack of detailed clinical presentation, haemodynamic status, treatment urgency, or outcome data, thus the essential parameters required for stratification and meaningful clinical comparison.
Similarly, the retrospective case series by Calderón et al. reported 11 patients with radiologically confirmed haemorrhagic cholecystitis based on ultrasound and computed tomography (CT) imaging [69]. While this study offers valuable insight into imaging characteristics, such as haemobilia (91%), hemoperitoneum (55%), and ductal bleeding manifestations, it was excluded from our analysis. Crucially, it lacked comprehensive clinical data on patient presentation, comorbidities, haemodynamic status, timing or urgency of intervention, treatment modalities, and patient outcomes. These omissions precluded meaningful comparison and stratification in our analysis.
In conclusion, both the Hotak and Calderón series offer contrasting perspectives on the clinical significance, severity, treatment application, and reported incidence of bleeding from the gallbladder, thus collectively highlighting the urgent need for standardised case documentation. Their divergence reinforces the importance of adopting a structured stratification framework based on clinical presentation, haemodynamic stability, and treatment urgency to enable more accurate reporting and a deeper, more consistent understanding of HC and HGB [68,69].
This review proposes a pragmatic stratification model based on clinical severity, with HC referring to haemodynamically stable patients managed conservatively or with elective intervention, and HGB representing unstable cases requiring urgent and/or multimodal treatment. Applying this model retrospectively, 48 of 65 cases (73.8%) met criteria for HGB, characterised by urgent intervention and haemorrhagic shock or a documented haemoglobin drop and blood transfusion. This underscores the life-threatening nature of HGB in the majority of patients. Although the overall mortality rate was 10.8%, stratification likely provides a more meaningful reflection of disease burden, with deaths predominating in the HGB subgroup. These findings reinforce the importance of standardised terminology, documentation, and a severity-based management approach tailored to patient physiology and clinical context.
Conclusions
HC and HGB represent a rare but clinically significant spectrum of gallbladder pathology, often presenting with overlapping symptoms and variable haemodynamic consequences. This systematic review highlights the heterogeneity in clinical presentation, risk factors, and treatment approaches, and reveals critical gaps in standardised terminology and reporting.
By introducing a stratification model based on clinical severity, distinguishing stable HC from unstable HGB, we propose a practical framework to enhance diagnostic suspicion, guide the urgency of intervention, and support consistent documentation. Wider adoption of this classification may improve recognition, allow for more accurate incidence reporting, and ultimately optimise patient outcomes through tailored management strategies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Dual paraneoplastic syndromes in a patient with small cell lung cancer: a case report J Med Case Rep Coners K Woods SE Webb M 318520112177130110.1186/1752-1947-5-318PMC 3158120 · doi ↗ · pubmed ↗
- 2Hemorrhagic cholecystitis Arch Surg Parekh J Corvera CU 2022041452010 http://Parekh J, Corvera CU. Hemorrhagic cholecystitis. Arch Surg. 2010 Feb;145(2):202-4. doi: PMID: 20157090.2015709010.1001/archsurg.2009.265 · doi ↗ · pubmed ↗
- 3Trends in vascular surgery since the introduction of percutaneous transluminal angioplasty Br J Surg Pell JP Whyman MR Fowkes FG 832835811994 https://doi.org/10.1002/bjs.1800810613804459410.1002/bjs.1800810613 · doi ↗ · pubmed ↗
- 4Hemorrhagic cholecystitis: report of a case Korean J Hepatobiliary Pancreat Surg Lee JW Park CY Park JH 5356162012 https://pmc.ncbi.nlm.nih.gov/articles/PMC 4575003/10.14701/kjhbps.2012.16.3.120PMC 457500326388920 · doi ↗ · pubmed ↗
- 5Acute cholecystitis in end-stage renal disease patients: a nation-wide longitudinal study Dig Liver Dis Chen YT Ou SM Chao PW 1421464520132302149310.1016/j.dld.2012.08.022 · doi ↗ · pubmed ↗
- 6Longitudinal follow-up of pulmonary function after lobectomy in childhood - factors affecting lung growth Pediatr Surg Int Nakajima C Kijimoto C Yokoyama Y 341345131998963961210.1007/s 003830050334 · doi ↗ · pubmed ↗
- 7Literature review and case series of haemorrhagic cholecystitis J Surg Case Rep Tarazi M Tomalieh FT Sweeney A 02019201910.1093/jscr/rjy 360PMC 632610330647900 · doi ↗ · pubmed ↗
- 8Management of NSAID-induced penetrating gastric ulcer complicated by hemorrhagic cholecystitis: the role of percutaneous transhepatic biliary drainage Radiol Case Rep Louis M Cawthon M Gibson B Kuhn B 405940651920243907688510.1016/j.radcr.2024.06.032PMC 11284942 · doi ↗ · pubmed ↗