Electrochemical nasal nitric oxide measurement during laryngeal mask ventilation as primary ciliary dyskinesia screening
Tobias Lipek, Maike vom Hove, Mandy Vogel, Konrad Platzer, Freerk Prenzel

TL;DR
A new electrochemical method for measuring nasal nitric oxide shows promise for diagnosing a rare genetic disorder in young children.
Contribution
A novel electrochemical technique for nasal nitric oxide measurement in children under 5 during laryngeal mask ventilation is introduced.
Findings
The technique showed high repeatability with an ICC of 0.974 in children under and over 5 years.
The coefficient of variation was 0.116, comparable to established chemiluminescence methods.
The method is feasible for young children and may simplify PCD diagnosis.
Abstract
Diagnosis of primary ciliary dyskinesia (PCD) can be challenging, especially in children of preschool age. Measurement of nasal nitric oxide (nNO) production helps in making the diagnosis. While chemiluminescence-based nNO measurement is sufficiently established, measuring nNO using electrochemical devices is common in older patients, although data on their repeatability and accuracy are scarce. This is a retrospective analysis of nNO measurements using an electrochemical technique (ECnNO) in 52 children undergoing bronchoscopy including 10 PCD cases. Using a novel approach to obtain electrochemical measurements in even very young children (n=31) (59.6%) were <5 years of age), ECnNO was measured while patients were in breath-hold during ventilation with laryngeal mask (ECnNO LAMA). For agreement, the intraclass correlation coefficient (ICC) was calculated. Precision is described by the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
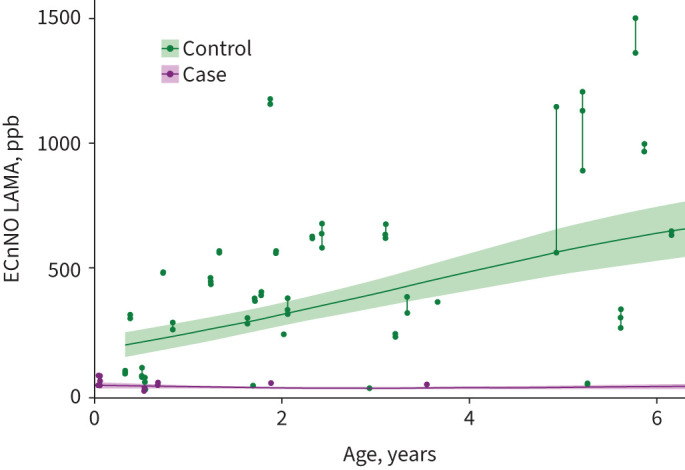 FIGURE 1
FIGURE 1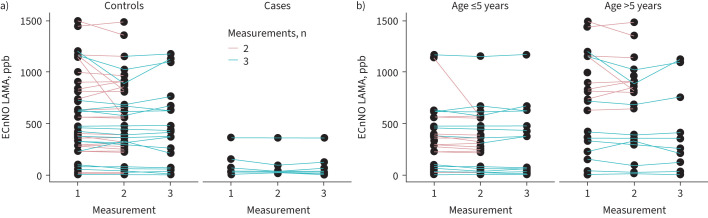 FIGURE 2
FIGURE 2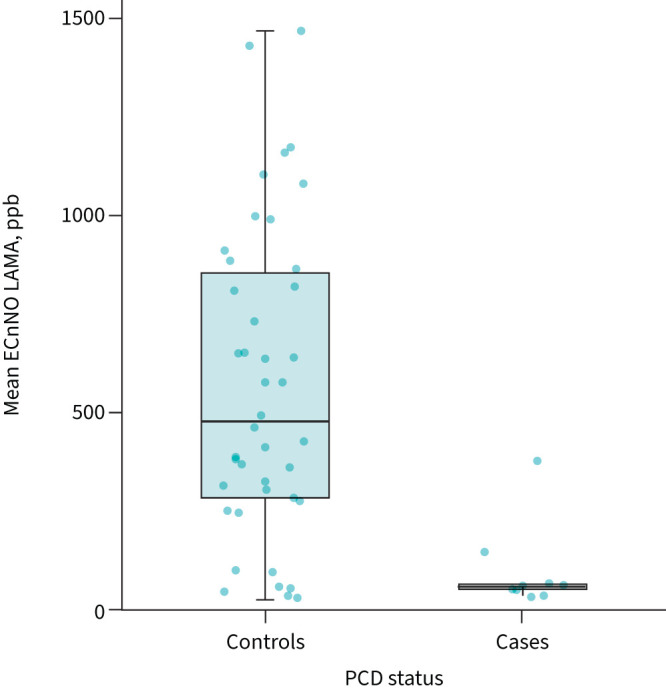 FIGURE 3
FIGURE 3| Patient number | Sex | Age at date of bronchoscopy (years) | Clinical features | TEM | IF | Genetic variants, protein effect, ACMG classification | Classification# | nNO measurements, ppb | ||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | ||||||||
|
| F | 0.1 | Perinatal persistent atelectasis of right UL; | Significant reduction of outer and inner dynein arms | Normal | Case | 68 | 28 | 29 | |
|
| M | 7.5 | Situs inversus totalis, chronic pansinusitis, chronic otitis media, | Not done | Not done | Case | 9 | 17 | 7 | |
|
| F | 0.1 | Term newborn with respiratory distress syndrome, congenital pneumonia | Normal | DNAH5 within cilia absent | Case | 28 | 45 | 66 | |
|
| F | 17.2 | Chronic rhinosinusitis with nasal polyposis, bronchiectasis in both LL, chronic otitis media with eardrum perforation; | Normal | Normal | Probable case | 42 | 35 | 38 | |
|
| M | 0.7 | Situs inversus totalis | Combined dynein arm defect | Sample quality insufficient | Case | 38 | 29 | 32 | |
|
| M | 3.6 | Chronic bronchitis, CDH, chronic otitis media | Not done | DNAH5, defect of outer dynein arm | Case | 33 | 32 | 30 | |
|
| F | 17.1 | Chronic otitis media, chronic mastoiditis, bronchiectasis in right ML and LL, infection by | Normal | Sample quality insufficient | Probable case | 363 | 360 | 361 | |
|
| M | 10.5 | Chronic bronchitis, bronchiectasis in ML, LL bilaterally, chronic rhinosinusitis, CDH | Not done | Sample quality insufficient | Case | 156 | 98 | 127 | |
|
| F | 1.9 | Full-term neonate with neonatal respiratory distress, recurrent pulmonary infections | Not done | DNAH5 mislocalisation compatible with defect of ODA | Case | 37 | 37 | 39 | |
|
| M | 0.5 | Full-term neonate with neonatal respiratory distress, situs inversus totalis, CCTGA | Not done | Normal | Two variants in | Probable case | 5 | 21 | 19 |
|
| |
| Overall | 4.85±4.68 (range 0.05–17.6) |
| <5 years | 31 (59.6%) |
| ≥5 years | 21 (40.4%) |
| Age in PCD group, years | 5.91±6.86 |
| Age in control group, years | 4.60±4.07 |
|
| |
| Female | 23 (44.2%) |
| Male | 29 (55.8%) |
|
| |
| Yes | 10 (19.2%) |
| No | 42 (80.8%) |
| ICC (95% CI) | CV (95% CI) | |
|---|---|---|
|
| 0.974 (0.972–0.990) | 0.116 (0.061–0.167) |
|
| 0.954 (0.943–0.984) | 0.127 (0.051–0.203) |
|
| 0.977 (0.966–0.993) | 0.100 (0.042–0.157) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAdvanced Chemical Sensor Technologies
Introduction
Primary ciliary dyskinesia (PCD) is an important differential diagnosis when reviewing young patients with chronic cough, hearing loss, chronic nasal congestion, unexplained neonatal respiratory distress, organ laterality defect, cardiac defects or bronchiectasis [1].
When suspecting PCD, clinicians face diagnostic challenges. Often, a variety of diagnostic procedures are needed to confirm or exclude PCD, including measurement of nasal nitric oxide (nNO), high-speed video microscopy analysis (HSVA), transmission electron microscopy (TEM), cell culture and genetic testing. Given its overall good negative predictive value, the European Respiratory Society (ERS) and the American Thoracic Society (ATS) both recommend nNO measurement as the first step in PCD diagnosis [2, 3]. As a screening tool, this measurement may reduce the burden of further invasive and costly investigations. Nonetheless, attention must be paid to technical detail; two different methods for nNO measurement are available.
Although the chemiluminescence technique has been extensively studied and used at larger tertiary centres, electrochemical nNO (ECnNO) testing is more widely used [4]. This is most likely the case because nNO measurements using chemiluminescence are many times more expensive than electrochemical measurements [5, 6], approximately EUR 50 000 versus EUR 3000 per device (values from own market research, for orientation only).
The main technical disadvantage of electrochemical measurement is the duration of constant airflow needed for valid measurements, making it practically impossible to use for children <5 years of age. Measurement of ECnNO requires ≥15 s, preferably 30 s, of sampling time [7, 8]. Using chemiluminescence techniques, it is possible to obtain valid measurements from an online display of nNO flow in only 3 s [5, 9], and the measurement may be completed even faster [10]. Furthermore, chemiluminescence measurements are possible during normal tidal breathing, during plateaus in breath-hold and during expiration against resistance. Measurements using electrochemical devices are more difficult to perform [11, 12]. Therefore, centres without access to chemiluminescence-based nNO (CInNO) devices face technical challenges in obtaining valid measurements, especially in young children.
In the device manual (NIOX VERO; Circassia AB, Uppsala, Sweden), only data from a company-funded study are available, and these were only published as a poster presentation [8, 13], while the registered study did not publish any results [14]. To our knowledge, no complete datasets on the accuracy, repeatability and precision of ECnNO measurements in children <5 years of age have been published. It is therefore not surprising that electrochemical measurement is not approved in the USA and clinicians question this method. This knowledge gap is addressed in the ERS’ recent technical standard on nNO measurement, in which the authors call for quality evidence regarding electrochemical analysers and sampling methods used in young children [4].
In this setting, we have introduced a new technique for measuring nNO with our electrochemical device, which is performed during ventilation with a laryngeal mask. The first test results were promising and could provide a practicable way to measure nNO. Hence, this retrospective pilot study aims to evaluate the repeatability of ECnNO measurement during laryngeal mask ventilation (ECnNO LAMA) in children.
Material and methods
Study subjects and setting
This monocentric retrospective comparative study was approved by the Research Ethics Committee of the Medical Faculty of the University of Leipzig (registration number 318/22 ek). The inclusion criteria were: scheduled bronchoscopy at our centre between February 2018 and January 2023; PCD as a potential differential diagnosis and therefore the clinical need to obtain nNO measurements; and written informed consent from the children's legal guardians for bronchoscopy and measurement of nNO, at least two measurements of the nNO value and general anaesthesia in accordance with local clinical standards. The only exclusion criterion was the presence of clear signs of a respiratory infection.
Diagnostic criteria of PCD cases and controls
The final PCD diagnosis was made based on the criteria from the international PCD registry (www.pcdregistry.eu/) [15] and the ERS/ATS guidelines [2, 3], with special emphasis on genetic diagnostics. HSVA was not available at our centre during the study, but it was performed on two patients at a national reference centre. Patients were regarded as PCD cases and probable cases, respectively, if 1) the clinical findings were consistent with PCD, and 2) at least one of the following four examination procedures revealed findings indicating pathogenicity: TEM, immunofluorescence microscopy, detection of biallelic mutation by genotyping or HSVA (table 1 and supplementary material). Patients with other respiratory diseases who did not meet the above diagnostic criteria for PCD were controls. Immunofluorescence microscopy, genetic testing and TEM were performed at external reference centres. For analyses requiring a dichotomous classification of diagnostic certainty (descriptive statistics and receiver operating characteristic (ROC) analysis), cases and probable cases were treated as one group versus controls. See figure S4 for a flow chart of the study population.
nNO measurements
The examinations were performed in one of four similar operating theatres with automatic air supply and air conditioning. nNO was measured via an electrochemical device (NIOX VERO; Circassia AB, Uppsala, Sweden) with a flow rate of 0.3 L·min^−1^. The ambient NO concentration was checked during all measurements and was always <5 ppb (below the detection limit of the device), which is well below the suggested threshold for absence [5]. With a controlled fresh air supply of 1600 m^3^·h^−1^ in the operating room, stable conditions for ambient air were assumed.
With adequate sedation, a laryngeal mask was inserted to exclude nasal exhalation during the nNO measurement. Standardised preparation for bronchoscopy was initiated, including continuous measurement of oxygen saturation and monitoring of exhaled carbon dioxide_._ The duration of each measurement was 30 s with breath-hold and paused ventilation (figure S1). Between measurements, patients were ventilated to ensure an oxygen saturation of >97% and normal expiratory carbon dioxide. Three measurements were attempted, but in the event of technical problems (e.g. sampling too short, blocked nose or internal device error), a third measurement was not repeated to avoid prolonged sedation.
Data analysis
Descriptive statistics are given as mean±sd for continuous variables and counts (percentages) for categorical variables.
To assess within-patient variability, i.e. agreement of the repeated nNO measurements per patient, we determined the intraclass correlation coefficient (ICC), also known as the reliability index. The ICC is estimated by applying variance components [16]. The categories chosen for the ICC for the strength of agreement are based on the categorisation by McBride [17] of Lin's concordance correlation coefficient for continuous variables: >0.99 (almost perfect), 0.95–0.99 (substantial), 0.90–0.95 (moderate) and <0.90 (poor).
We calculated the precision of the measurement per subject using the coefficient of variation (CV). Group comparison of the CVs was carried out using an unpaired t-test. The nNO thresholds were determined using ROC analysis based on the mean value of the nNO measurements obtained per person.
The significance level was set to α=0.05. Statistical analyses were performed using R (www.R-project.org) for ROC, CV and ICC; jamovi (www.jamovi.org) was used for descriptive statistics. In R, the package pROC [18] was used for ROC analysis, the package cccrm [19] was used for calculation of the ICC and ggplot2 [20] was used for visualisation.
Results
A total of 70 patients were examined, with 52 patients meeting the inclusion criteria. For 18 patients, the clinical records showed signs of upper respiratory infection (URI), leading to their exclusion. Of the children examined, 10 were diagnosed with confirmed or probable PCD and 42 were classified as a control group with other respiratory diseases. The characteristics of the study population are shown in table 2, and the details of the patients with PCD are listed in table 1. Age distribution versus PCD status is also shown in figure 1. Three nNO measurements were obtained in a total of 29 (55.8%) patients, and two measurements were recorded in 23 patients.
Electrochemical nasal nitric oxide measurement during laryngeal mask ventilation (ECnNO LAMA) versus age in cases and controls. Shaded areas represent confidence intervals. The x-axis is clipped at approximately 6 years of age. See figure S2 for the whole cohort.
Repeatability of ECnNO LAMA measurements
Figure 2 presents the measurements stratified by age (≤5 versus >5 years) and PCD status, showing the overall good consistency of repeated measurements.
Plots showing all measurements in all subjects studied: a) controls versus cases, and b) patients ≤5 years versus those >5 years of age. ECnNO LAMA: electrochemical nasal nitric oxide measurement during laryngeal mask ventilation.
The ICCs and CVs are shown in table 3. The ICCs were >0.95 in the total cohort and in both age groups. As the two confidence intervals substantially overlapped, we were unable to determine a statistically significant difference in the ICC between the two age groups. Likewise, we found no significant difference in CVs between these groups (both p>0.5).
Diagnostic performance of ECnNO LAMA measurements
The nNO measurements in our cohort differed significantly between patients with PCD and controls (74.3±38 versus 555±396 ppb, p<0.001) (figure 3). The ROC analysis resulted in an area under the curve of 0.89. The optimal cut-off of 178 ppb (flow rate 53.4 nL·min^−1^) yielded a specificity of 0.833 and a sensitivity of 0.900 (figure S3).
Electrochemical nasal nitric oxide measurement during laryngeal mask ventilation (ECnNO LAMA) in primary ciliary dyskinesia (PCD) versus controls. Horizonal bars represent medians, boxes represent interquartile ranges and whiskers represent ranges.
Discussion
To our knowledge, the results of this pilot study represent the first complete dataset on the reproducibility of ECnNO measurement for PCD screening in a paediatric cohort, which includes a substantial proportion of children under the age of 5 years. ECnNO measurements during general anaesthesia with ventilation via a laryngeal mask were possible in children of all age groups without complications. Repeated measurements showed considerable agreement and the diagnostic performance indicated the usefulness of the method in screening for PCD.
The repeatability (agreement and precision) of nNO measurements were determined using ICCs and CVs. ICCs were >0.95 in the overall cohort, with no statistical difference between age groups (>5 and ≤5 years), indicating a high level of agreement [17]. Compared with previously reported ICCs for chemiluminescence-based nNO measurements in children aged 5–18 years, the agreement of nNO measurements in our study was higher and, most importantly, independent of the breathing technique used [21].
In terms of precision, the CV in our overall cohort was 11.6% with no significant difference for ages ≥5 or <5 years. Comparison with existing data is challenging, as data on the repeatability of ECnNO measurements are not available for currently available devices. However, there are studies on an ECnNO analyser (NIOX MINO) that is no longer on the market. Using this device, a CV of 15% was documented in a cohort of children and adults (age distribution not specified) using the tidal breathing technique (5 mL·s^−1^, 45 s sampling time with mouth open), with valid measurements in 48 out of 50 subjects [22]. In another cohort of 57 subjects, including two subjects who were <5 years old, the CV for ECnNO was 10% for the same recording technique (tidal breathing, 5 mL·s^−1^; data extracted from results tables) [23]. Thus, our method shows comparable or better precision in a much younger cohort. It is not possible to differentiate whether this is due to a different analysis technique (less flow and less acquisition time required) or to a smaller variation in breath-holding time due to laryngeal breathing versus tidal breathing with an open mouth.
Numerous precision data have been published for nNO measured by chemiluminescence, which allow a comparison with our results. As ECnNO LAMA is most comparable to the breath-holding technique, we have focused on this method for comparisons. The reported CV varied from 16.6% in a small cohort of 20 children [24] to 6.7% in a cohort of 282 individuals, 58.5% of whom were <16 years old [25].
In the latter study, outliers (i.e. deviating values that were not further defined) “were discarded at the technician's discretion”. The stated CV could therefore underestimate the actual variance that would have resulted if all measurements had been included. We consider it a strength of our study that we have included all measurements without neglecting outliers.
Determining nNO values using breath-holding manoeuvres is extremely challenging in younger children. In a study by Beydon et al. [9], technically reliable chemiluminescence measurements during breath-hold, slow expiration against resistance and tidal breathing were possible in as few as 5.6%, 21% and 77% of 105 children under the age of 5 years. CVs in tidal breathing measurements tend to be higher than in velum closure manoeuvres [26, 27].
In summary, the ECnNO LAMA method has a CV comparable to the chemiluminescence technique using velum closure manoeuvres (expiration against resistance and breath-holding) in children aged <5 years. We are unable to determine whether this is due to the electrochemical device itself or due to the measurement setting.
Although this aspect was not the primary focus of the study, ECnNO values were lower in younger children, and there was a large overlap in ECnNO results, especially in the younger patients (figures 1, 2b and S2). This is not surprising because it is well known that nNO values are physiologically lower in the first year of life and during URIs [23]. For this reason, nNO screening values should be confirmed by repeated measurements at this age, especially if pathologically low values are detected.
As with all nNO measurement techniques, the ECnNO technique must be postponed or reassessed if there is evidence of a URI, as was the case in a substantial proportion of all records available in our study (18 out of 70). When describing the characteristics of the measurement, it is important to note that low absolute values in children may be due to young age or clinically silent URI and do not necessarily reflect pathology. Still, repeatability within a series of measurements is not affected.
It has already been noted that nNO screening is limited and that the currently used cut-off values may need to be revised [28]. In our pilot study with multiple measurements in a mixed cohort comprising 10 PCD cases, ECnNO LAMA screening showed a decent ability to find cases, with a specificity of 0.833 and a sensitivity of 0.90. The optimal cut-off value of 178 ppb was found in an ROC analysis. These results should be considered as a proof of concept in our data. Undoubtedly, this needs to be verified by larger studies with complete diagnostics including functional analysis (HSVA) in all patients. We do not recommend using these rather preliminary cut-offs in clinical practice until further validated data are available.
At our regional centre, bronchoscopies are performed as part of our diagnostic workup in selected children with chronic wet cough to rule out anatomical variations and collect lower airway samples, especially in young children who cannot produce sputum. It must be acknowledged, however, that this approach may be unsuitable for other centres and their patient populations. Of course, bronchoscopy is not a mandatory procedure for diagnosing PCD. Nasal brush biopsy can be performed without general anaesthesia even in very young children.
Limitations of our study include its retrospective nature, the relatively small number of cases including three patients with only probable PCD and the lack of HSVA performed at our site. As functional evaluation of ciliary function was only performed externally in a few patients with very high clinical suspicion, other PCD cases could have been missed. This may influence the results of the sensitivity/specificity analysis.
Moreover, although our results show a wide range for possible ECnNO LAMA data, this does not technically exclude effects of the anaesthetics used on the whole cohort, as it is possible that systemic administration of such drugs could affect nitric oxide production in humans in general. However, this should not affect the ECnNO LAMA technique or its characteristics per se.
It is essential that the ECnNO LAMA measurements are verified in future studies with larger cohorts and that age-specific cut-off values are determined. A comparison with chemiluminescence-based nNO measurements as the gold standard is required in such studies to determine diagnostic accuracy.
In conclusion, our novel ECnNO LAMA technique is feasible and showed promising repeatability and precision in screening for PCD in children <5 years of age. While further studies are needed, the method may help in the diagnosis of PCD in young patients and simplify a challenging differential diagnostic process.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Leigh MW, Ferkol TW, Davis SD, et al. Clinical features and associated likelihood of primary ciliary dyskinesia in children and adolescents. Ann Am Thorac Soc 2016; 13: 1305–1313. doi:10.1513/Annals ATS.201511-748OC 27070726 PMC 5021075 · doi ↗ · pubmed ↗
- 2Shapiro AJ, Davis SD, Polineni D, et al. Diagnosis of primary ciliary dyskinesia. An official American Thoracic Society clinical practice guideline. Am J Respir Crit Care Med 2018; 197: e 24–e 39. doi:10.1164/rccm.201805-0819 ST 29905515 PMC 6006411 · doi ↗ · pubmed ↗
- 3Lucas JS, Barbato A, Collins SA, et al. European Respiratory Society guidelines for the diagnosis of primary ciliary dyskinesia. Eur Respir J 2017; 49: 1601090. doi:10.1183/13993003.01090-201627836958 PMC 6054534 · doi ↗ · pubmed ↗
- 4Beydon N, Kouis P, Marthin JK, et al. Nasal nitric oxide measurement in children for the diagnosis of primary ciliary dyskinesia: European Respiratory Society technical standard. Eur Respir J 2023; 61: 2202031. doi:10.1183/13993003.02031-202236822632 · doi ↗ · pubmed ↗
- 5Shapiro AJ, Dell SD, Gaston B, et al. Nasal nitric oxide measurement in primary ciliary dyskinesia. A technical paper on standardized testing protocols. Ann Am Thorac Soc 2020; 17: e 1–e 12. doi:10.1513/Annals ATS.201904-347OT 31770003 PMC 6993796 · doi ↗ · pubmed ↗
- 6Manna A, Montella S, Maniscalco M, et al. Clinical application of nasal nitric oxide measurement in pediatric airway diseases. Pediatr Pulmonol 2015; 50: 85–99. doi:10.1002/ppul.2309425156952 · doi ↗ · pubmed ↗
- 7Circassia. 2023. NIOX VERO Nasal user manual German. Date last accessed: 22 August 2025.
- 8Circassia. 2023. Product labeling summary/package insert NIOX VERO. Date last accessed: 22 August 2025.