Highlighting the Importance of His Bundle Potential During Tachycardia and Ventricular Overdrive Pacing
Yasuharu Matsunaga‐Lee, Yasuyuki Egami, Koji Yasumoto, Masamichi Yano, Masami Nishino

TL;DR
This paper explains how His bundle potential helps distinguish between two types of heart rhythm disorders during specific pacing techniques.
Contribution
It identifies His–tachycardia dissociation as a key diagnostic marker for differentiating AVNRT from NF-ORT.
Findings
AVNRT and NF-ORT can both occur with HV block.
His–tachycardia dissociation during ventricular overdrive pacing is critical for diagnosis.
Abstract
Both AVNRT and NF‐ORT can be sustained with HV block. His–tachycardia dissociation during ventricular overdrive pacing is a key finding for differentiating AVNRT from NF‐ORT.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
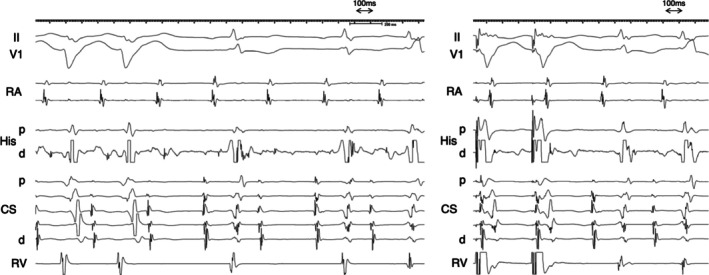 Figure 1
Figure 1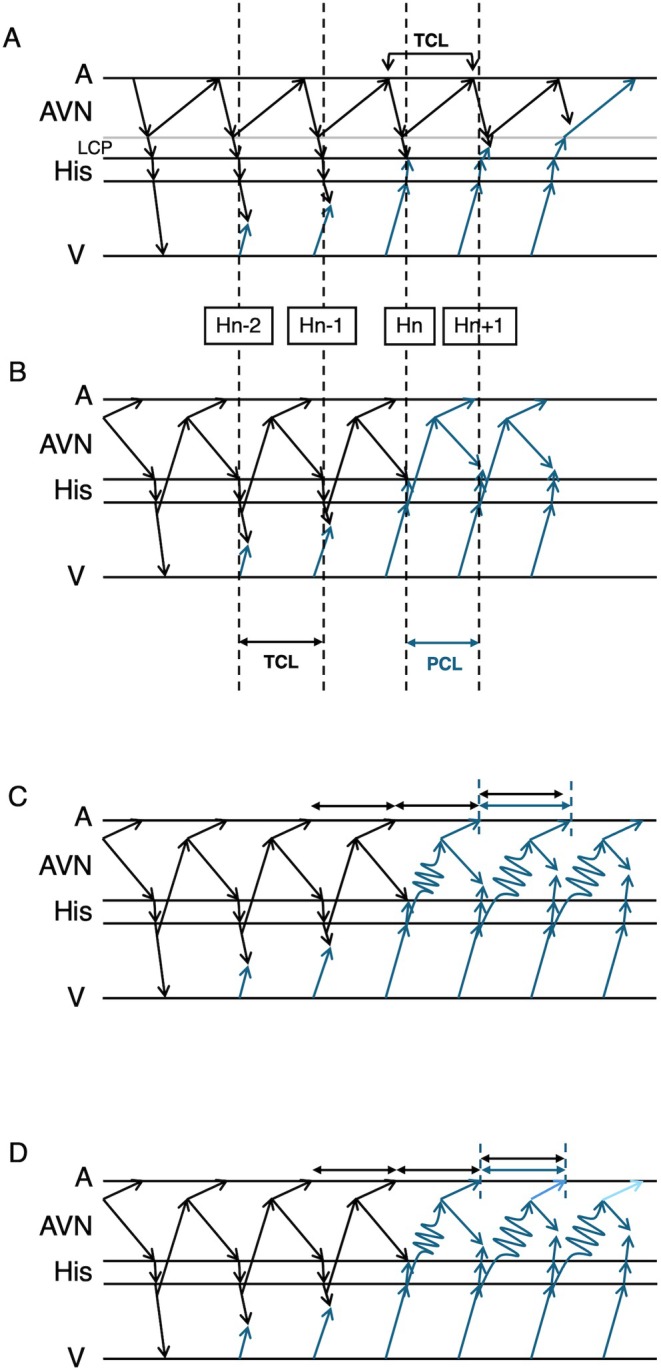 Figure 2
Figure 2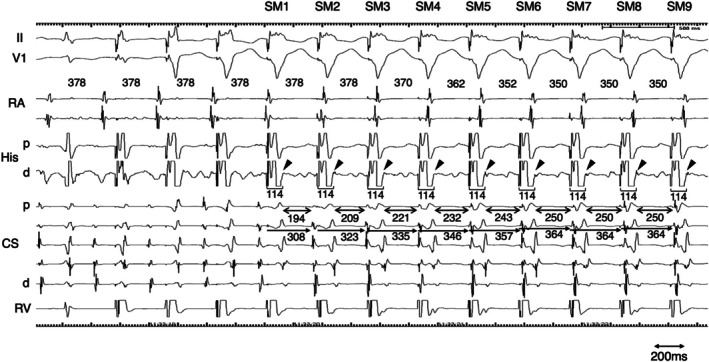 Figure 3
Figure 3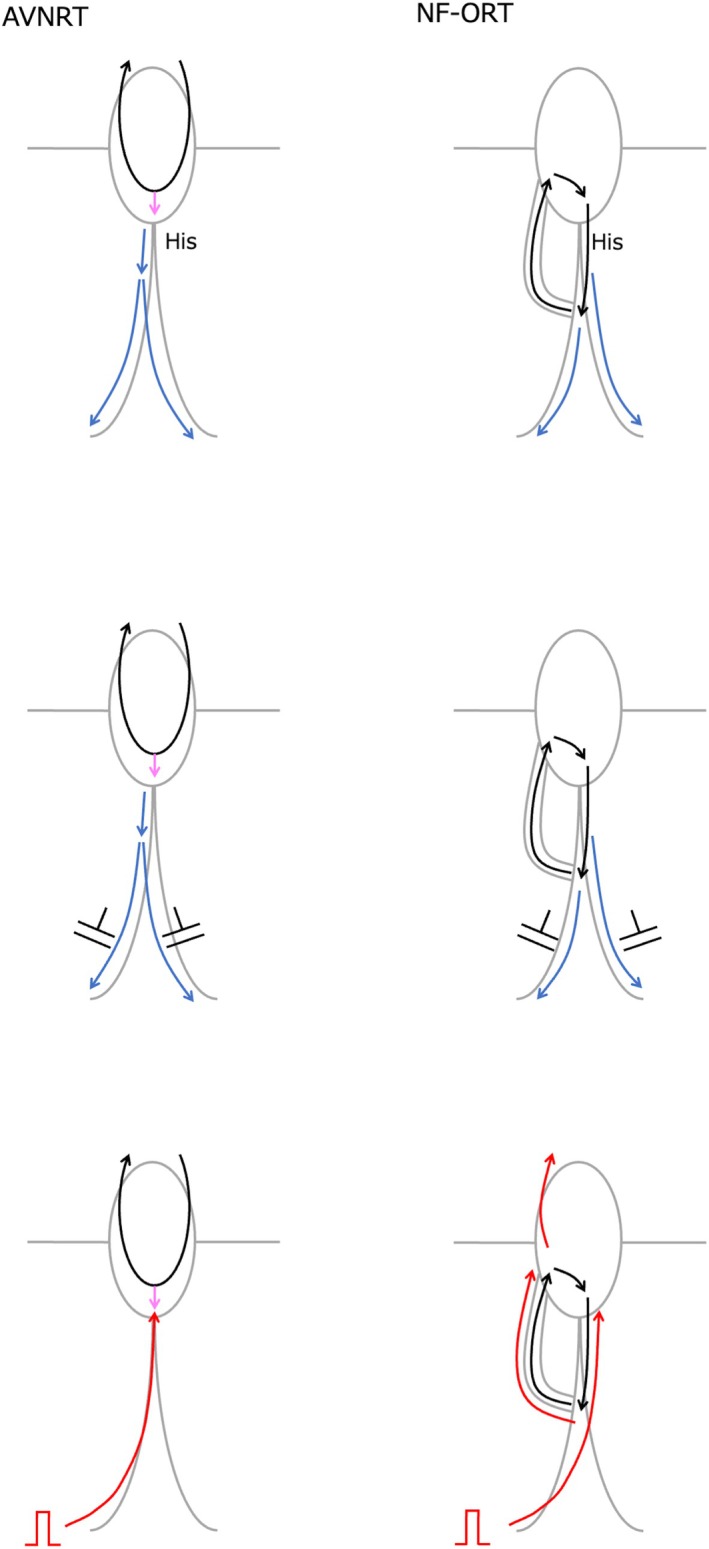 Figure 4
Figure 4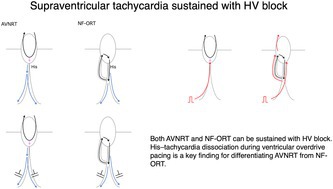 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac pacing and defibrillation studies · Cardiac Arrhythmias and Treatments · Cardiac electrophysiology and arrhythmias
A man in his 10s was referred to our hospital because of symptomatic palpitations. The surface 12‐lead electrocardiogram (ECG) exhibited a narrow QRS tachycardia with a long RP interval. At baseline, the atrio‐His (AH) and His‐ventricular (HV) intervals were 73 msec and 56 msec, respectively. The effective refractory period of atrioventricular conduction during baseline pacing was 380 msec, determined by the occurrence of an AH block. A narrow QRS tachycardia was induced with ventricular burst pacing. During tachycardia, tachycardia sustained with atrioventricular block (AVB) (Figure 1 Left). The earliest atrial activation was at the proximal coronary sinus (CS). A V‐A‐V response was observed following ventricular overdrive pacing (VOP) from the apex of the right ventricle. The corrected post pacing interval minus tachycardia cycle length (cPPI–TCL) was 144 msec, as calculated 525–375–(97–91) (Figure 1 Right). The His‐atrial (HA) intervals during VOP and tachycardia were 258 msec and 249 msec, respectively. The difference between the stimulus‐atrial interval during VOP and the ventriculoatrial interval was 156 msec, calculated as 358–202. During VOP, the retrograde His potential was recoded just after the ventricular potential recoded at the His catheter (Figure 2). The stim‐His interval was stable after the first stable morphology of the QRS complex (SM), whereas the atrial‐atrial interval was reset after the third SM.
Narrow QRS tachycardia persisting during AVB ruled out orthodromic reciprocating tachycardia (ORT) involving an atrioventricular or nodo‐ventricular (NV) bypass tract. A V‐A‐V pattern after ventricular overdrive pacing excluded atrial tachycardia. When AVB occurs at the atrio‐His conduction level, ORT using a nodo‐fascicular bypass tract (NF‐ORT) is also excluded (Figure 3). An atypical atrioventricular nodal reentrant tachycardia (AVNRT) could be sustained with AH block if a lower common pathway (LCP) is blocked. In this case, a His bundle potential was recorded during AVB, indicating that the block occurred at the HV level. Therefore, remaining possible diagnoses were atypical AVNRT or NF‐ORT (Figure 3). In this case, left and right bundle branch block morphology were observed during AVB (Figure 1). Although long PPI‐TCL supported atypical AVNRT [1, 2], the decremental property of the concealed NF bypass tract [3] could also result in a long PPI after VOP. In this case, a retrograde His potential was observed on the His catheter following the ventricular potential during ventricular extra‐stimulation at baseline. The conversion of the potential sequence from His‐ventricular to ventricular‐His was presumed to result from retrograde conduction block within the conduction system [4]. During VOP, a retrograde His potential was recorded on the distal His catheter following the ventricular potential after the first stable morphology of the QRS complex, and a stable stim‐His interval was subsequently observed during pacing. At the time when a His bundle potential was captured by VOP, the TCL, assessed by the atrial electrogram interval, was not affected by VOP. This observation was interpreted as His‐tachycardia dissociation, which is theoretically never observed in NF‐ORT. The tachycardia was diagnosed as an atypical AVNRT. Radiofrequency ablation at the earliest atrial activation site rendered the tachycardia noninducible, following a junctional response.
Narrow QRS tachycardia in the presence of AVB is often considered to represent either atrial tachycardia with AVB or AVNRT with LCP block. AVNRT with LCP block is associated with AH block. The presence of AVB at the AH level effectively excludes the possibility of NV/NF‐ORT. In the present case, however, AVB occurred at the HV level, necessitating further diagnostic evaluation to distinguish between AVNRT and NF‐ORT. Although NF‐ORT could theoretically be sustained despite an HV block if both left and right bundle branch blocks occur distal to the bifurcation of the NF accessory pathway, to the best of our knowledge, there have been no documented clinical observations of this in the literature. One possible reason is the diagnostic challenge in differentiating NF‐ORT from AVNRT. In a previous study that proposed diagnostic criteria for distinguishing NV/NF‐ORT from AVNRT, the cPPI–TCL was reported to be useful for NV‐ORT, but not for NF‐ORT [2]. This case underscores the clinical value of careful His bundle potential analysis in differentiating the underlying mechanism of sustained narrow QRS tachycardia in the presence of AVB. The theoretical concepts and limitations underlying the differential diagnosis during VOP are illustrated in Figure 4. The timing of the first reset His potential was defined as Hn. The preceding and following His potentials are defined as Hn‐2, Hn‐1, and Hn + 1. The interval between Hn‐2 and Hn‐1 corresponds to TCL, and the interval between Hn and Hn + 1 corresponds to the pacing cycle length (PCL). The interval between Hn‐1 and Hn is between TCL and PCL. In the case of NRT, since the His bundle is not included in the circuit, the timing of atrial reset can be delayed to the timing of His reset. The decremental property of retrograde nodal conduction, can prolong the HA interval. In this case, this decremental property accounted for the discrepancy of the atrial interval after His reset. In the case of NF‐ORT, since the His bundle is included in the circuit, at the timing of His reset, the tachycardia is reset by pacing, and the atrial interval should also be reset. However, because the interval between Hn‐1 and Hn is shorter than the TCL, the decremental property of retrograde conduction can mask the atrial reset. In this situation, the following His interval between Hn and Hn + 1 is even shorter than that between Hn‐1 and Hn, and the degree of atrial delay is expected to be even longer than the previous prolongation. Thus, the next atrial interval is speculated to be longer than the TCL. In this case, the atrial intervals were always ≤ TCL, which excluded the possibility of NF‐ORT. The limitation of this diagnostic interpretation arises when both the NF and slow pathways exhibit decremental properties. If these decremental properties act independently, a short interval input to the NF‐ACP can result in a longer input to the slow pathway, which in turn produces either a shorter or longer atrial interval or no net change at all. Taking these limitations into account, from the current electrophysiological standpoint [5], the most reasonable diagnosis in this case is AVNRT rather than NF‐ORT.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1G. F. Michaud , H. Tada , S. Chough , et al., “Differentiation of Atypical Atrioventricular Node Re‐Entrant Tachycardia From Orthodromic Reciprocating Tachycardia Using a Septal Accessory Pathway by the Response to Ventricular Pacing,” Journal of the American College of Cardiology 38, no. 4 (2001): 1163–1167.11583898 10.1016/s 0735-1097(01)01480-2 · doi ↗ · pubmed ↗
- 2K. Nagashima , Y. Kaneko , M. Maruyama , et al., “Novel Diagnostic Observations of Nodoventricular/Nodofascicular Pathway‐Related Orthodromic Reciprocating Tachycardia Differentiating From Atrioventricular Nodal Re‐Entrant Tachycardia,” JACC Clinical Electrophysiology 6, no. 14 (2020): 1797–1807.33357576 10.1016/j.jacep.2020.07.007 · doi ↗ · pubmed ↗
- 3K. Onuki , K. Nagashima , Y. Matsunaga‐Lee , et al., “Decremental Properties of a Concealed Nodoventricular Pathway,” Journal of Cardiovascular Electrophysiology 35, no. 11 (2024): 2254–2257.39256920 10.1111/jce.16430 · doi ↗ · pubmed ↗
- 4K. Ukita , Y. Egami , Y. Matsunaga‐Lee , et al., “A Case of a ‘Pseudo Jump‐Up Phenomenon’ Caused by Retrograde Ventricular‐His Prolongation,” Journal of Electrocardiology 58 (2020): 43–45.31710874 10.1016/j.jelectrocard.2019.11.003 · doi ↗ · pubmed ↗
- 5A. Doi , N. Miyazaki , T. Goda , et al., “Irregular Narrow QRS Complex Tachycardia With Intermittent Atrioventricular Dissociation: What Is the Mechanism?,” Journal of Cardiovascular Electrophysiology 31 (2020): 2234–2237.32529764 10.1111/jce.14610 · doi ↗ · pubmed ↗