Paraneoplastic Cerebellar Degeneration from Subclinical Breast Cancer on Mammography
Shinsuke Sasada, Ayumi Kawamata

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
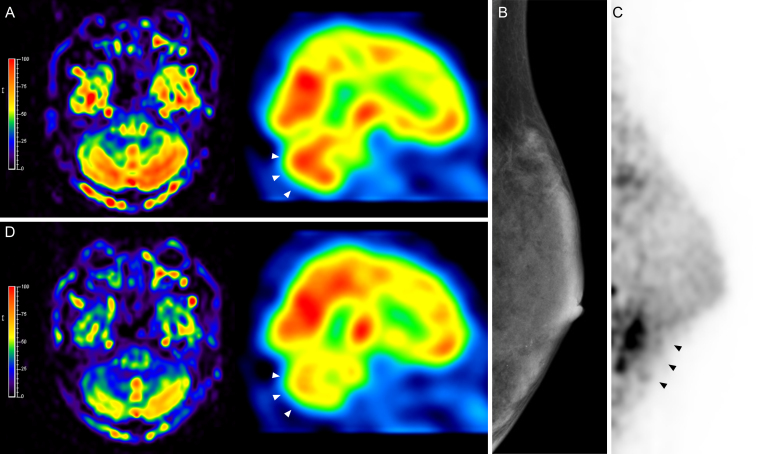 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAutoimmune Neurological Disorders and Treatments · Neuroscience and Neuropharmacology Research · Neurological Complications and Syndromes
Paraneoplastic cerebellar degeneration (PCD) is a rare presentation of tumor immune-mediated cerebellar ataxias ^(1), (2), (3)^. PCD often occurs with breast and gynecologic cancer (anti-Yo and anti-Ri antibodies), small cell lung cancer (anti-Hu and anti-CV2/ collapsin response-mediator protein 5 [CRMP5]), and Hodgkin’s lymphoma (anti-Tr antibodies) ^(4)^. A 45-year-old female with PCD developed worsening gait impairment and increased cerebellar perfusion on brain single photon emission computed tomography (SPECT) (Figure 1A). The anti-Yo antibody was present in the cerebrospinal fluid. Left breast cancer was subclinical on mammography (Figure 1B); however, it was detected via dedicated breast positron emission tomography (dbPET) (Figure 1C). She underwent a mastectomy and was diagnosed with invasive ductal carcinoma with an invasive diameter of 3 mm. The intensity of cerebellar hypermetabolism decreased on brain SPECT a week post-surgery (Figure 1D). She remained symptomatic without further progression. Patients with PCD symptoms and specific antibodies require appropriate diagnostic evaluation to identify the underlying cause.
Article Information
Author Contributions
All the authors cared for the patient. Shinsuke Sasada drafted the manuscript, and Ayumi Kawamata approved the final version of the manuscript.
Conflicts of Interest
None
Approval by Institutional Review Board (IRB)
IRB approval was not required for this study.
Informed Consent
Informed consent was obtained from the patient.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mitoma H, Manto M, Hadjivassiliou M. Immune-mediated cerebellar ataxias: clinical diagnosis and treatment based on immunological and physiological mechanisms. J Mov Disord. 2021;14(1):10-28.33423437 10.14802/jmd.20040 PMC 7840241 · doi ↗ · pubmed ↗
- 2Vogrig A, Gigli GL, Segatti S, et al. Epidemiology of paraneoplastic neurological syndromes: a population-based study. J Neurol. 2020;267(1):26-35.31552550 10.1007/s 00415-019-09544-1 · doi ↗ · pubmed ↗
- 3Hadjivassiliou M, Martindale J, Shanmugarajah P, et al. Causes of progressive cerebellar ataxia: prospective evaluation of 1500 patients. J Neurol Neurosurg Psychiatry. 2017;88(4):301-9.27965395 10.1136/jnnp-2016-314863 · doi ↗ · pubmed ↗
- 4Loehrer PA, Zieger L, Simon OJ. Update on paraneoplastic cerebellar degeneration. Brain Sci. 2021;11(11):1414.34827413 10.3390/brainsci 11111414 PMC 8615604 · doi ↗ · pubmed ↗