Enucleation of a Large Pseudo-Mesenteric Cyst with Hemorrhage and Infection: A Case Report
Takeshi Utsunomiya, Jota Watanabe, Ryo Karasudani, Naho Ishimura, Atsushi Takada, Masayuki Kanzaki, Shigehiko Yagi, Hirotsugu Yoshiyama, Satoshi Sumida, Hiromi Ohtani

TL;DR
A rare case of a large infected pseudo-mesenteric cyst was successfully removed without cutting the intestine, showing a novel surgical approach.
Contribution
This case introduces enucleation as a novel surgical method for treating large infected pseudo-mesenteric cysts without intestinal resection.
Findings
A 17 cm pseudo-mesenteric cyst was successfully enucleated without intestinal resection.
The procedure was performed due to severe inflammation and vena cava compression.
Meticulous surgical planning enabled complete removal of the cyst.
Abstract
Pseudo-mesenteric cysts are exceptionally rare lesions, with limited reports of surgical management. This case highlights the novelty of enucleating a large infected pseudo-mesenteric cyst without intestinal resection, emphasizing its clinical significance. We report the case of a 64-year-old man who presented with acute abdomen. Computed tomography revealed a cystic lesion approximately 17 cm in size with an enhanced capsule in the sigmoid mesentery. Emergency surgery was warranted due to severe inflammation and inferior vena cava compression. Initial laparoscopy ruled out appendiceal abnormalities, and laparotomy was performed. Careful dissection along the thickened cyst wall, as seen on preoperative imaging, enabled complete enucleation without the need for intestinal resection. This case demonstrates successful enucleation of a giant pseudo-mesenteric cyst, a rare surgical…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
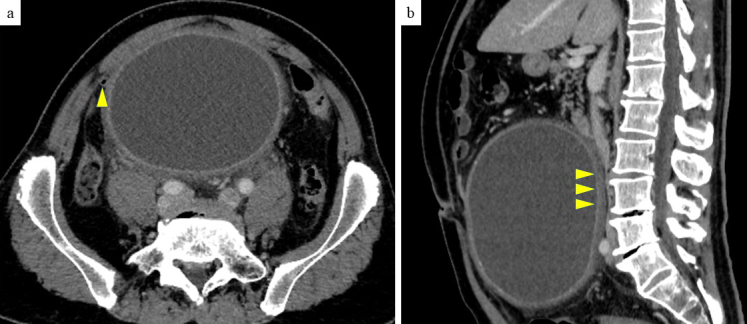 Figure 1
Figure 1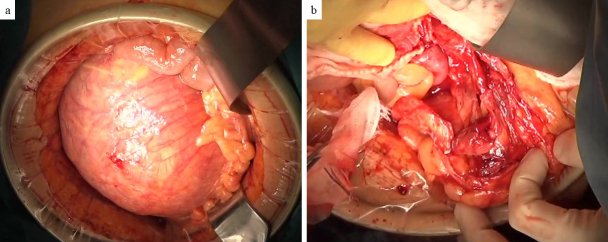 Figure 2
Figure 2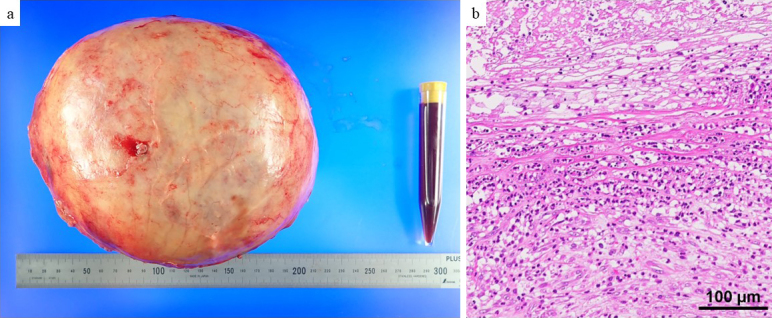 Figure 3
Figure 3| No | Reference | Reported year | Age | Gender | Location | Size (mm) | Trauma history | Laparoscopic operation | Enucleation | Bowel resection |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 |
| 2000 | 31 | Female | Mesojejunum | 40 | − | − | + | − |
| 2 |
| 2002 | 66 | Male | Mesojejunum | 55 | − | − | − | + |
| 3 |
| 2003 | 41 | Female | Mesojejunum | 40 | − | + | + | − |
| 4 | 2003 | 43 | Female | Mesotransverse | 150 | − | − | − | + | |
| 5 |
| 2003 | 38 | Female | Mesoileum | 110 | − | − | − | + |
| 6 |
| 2003 | 31 | Female | Mesosigmoid | 100 | − | − | − | + |
| 7 |
| 2004 | 16 | Male | Mesojejunum | 55 | − | − | + | − |
| 8 |
| 2004 | 74 | Male | Mesoileum | 60 | − | − | − | + |
| 9 |
| 2005 | 50 | Female | Mesoileocecum | 140 | − | − | − | + |
| 10 |
| 2007 | 63 | Male | Mesojejunum | 55 | − | + | + | - |
| 11 |
| 2007 | 84 | Female | Mesoileum | 65 | − | − | − | + |
| 12 |
| 2008 | 74 | Female | Mesojejunum | 80 | − | − | − | + |
| 13 |
| 2010 | 76 | Male | Ligamentum gastrocolicum | 210 | + | + | − | |
| 14 |
| 2014 | 65 | Male | Mesojejunum | 40 | − | + | + | − |
| 15 |
| 2014 | 83 | Female | Mesoileocecum | 110 | − | − | + | |
| 16 |
| 2017 | 64 | Male | Mesoaccending colon~mesotransverse colon | 120 | − | − | − | + |
| 17 |
| 2017 | 44 | Female | Mesojejunum | 42 | − | + | - | + |
| 18 |
| 2017 | 47 | Female | Meso small intestine | 140 | − | − | + | − |
| 19 |
| 2018 | 73 | Female | Mesosigmoid | 52 | − | + | + | − |
| 20 |
| 2018 | 32 | Male | Mesojejunum | 55 | − | + | + | − |
| 21 |
| 2018 | 22 | Male | Mesojejunum | 40 | − | + | + | − |
| 22 |
| 2018 | 60 | Male | Meso small intestine | 60 | − | − | + | − |
| 23 |
| 2019 | 16 | Male | Mesojejunum | 65 | − | − | + | − |
| 24 |
| 2021 | 40 | Female | Meso ascending colon | 142 | − | − | − | + |
| 25 |
| 2021 | 55 | Female | Mesojejunum | 35 | − | + | + | − |
| 26 |
| 2022 | 33 | Female | Mesojejunum | 55 | − | + | + | − |
| 27 | Our case | 2024 | 64 | Male | Mesosigmoid | 210 | − | − | + | − |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVascular Malformations and Hemangiomas · Genetic and Kidney Cyst Diseases
Introduction
Mesenteric cysts are uncommon benign masses, with an incidence of approximately 1 in 20,000 in the pediatric population ^(1)^. Pseudo-mesenteric cysts represent an extremely rare subtype. In terms of location, 60% of cases are reported in the small bowel mesentery, while 24% occur in the large bowel mesentery ^(2)^. We present a case of a large pseudo-mesenteric cyst treated by open enucleation.
Case Report
The patient was a 64-year-old man. Four days before referral to our hospital, he developed right lower abdominal pain, followed by progressive abdominal distention over the next 3 days. He also noticed an increase in his belt hole size during this period. He had no history of abdominal trauma. The patient’s blood biochemical data were as follows: white blood cell count, 9530/μL (3,300-8,600/μL); hemoglobin, 13.2 g/dL (13.7-16.8 g/dL); C-reactive protein, 22.34 mg/dL (0.00-0.14 mg/dL); carcinoembryonic antigen, 2.2 ng/mL (0.0-5.0 ng/mL); carbohydrate antigen 19-9, 8.2 U/mL (0.0-37.0 U/mL); and no hepatic enzymes or renal function abnormalities were noted. Contrast-enhanced computed tomography revealed a cystic lesion approximately 17 cm in length with an enhanced capsule in the sigmoid mesentery. No internal contrast-enhanced nodules were observed, but elevated peri-cystic lipid density suggested inflammation. An infected mesenteric cyst was the most likely diagnosis. The cyst was in contact with the appendix (Figure 1a), raising the possibility of abscess formation due to perforated appendicitis. However, these distinctions were difficult to make with preoperative imaging. The cyst was large, with the superior mesenteric artery and vein draining ventrally, the inferior mesenteric artery draining leftward, and evidence of compression of the inferior vena cava (Figure 1b). Emergency surgery was performed. First, diagnostic laparoscopy was performed to rule out perforated appendicitis. Laparoscopy revealed no evident inflammatory changes in the appendix. Laparotomy was performed. The cyst was located within the mesentery of the sigmoid colon (Figure 2a), but there was no continuity with the intestinal tract. The cyst capsule was relatively thick, allowing for enucleation via sharp dissection along the capsule (Figure 2b). The operation lasted 147 min, with a blood loss of 425 mL. The enucleated mesenteric cyst had a maximum diameter of 21 cm (Figure 3a). The cystic fluid was a light, pleomorphic solution (Figure 3a), with no malignant findings on cytology. The cystic fluid culture tests identified Clostridium ramosum, Eubacterium callanderi, and Parabacteroides distasonis, while no bacteria were detected in the ascitic fluid cultures. Postoperatively, the patient showed overall good progress and was discharged on the 18th postoperative day. Histological examination revealed a monocystic structure with a fibrous connective tissue cyst wall, lacking epithelial or endothelial cells on the luminal surface (Figure 3b). The pathological diagnosis was a pseudo-mesenteric cyst. Eight months post-surgery, no recurrence has been observed.
a) Contrast-enhanced horizontal CT image: The appendix is in contact with a large cyst (arrowhead). The continuity between the appendix and cyst is unclear on CT.b) Contrast-enhanced sagittal CT image: The IVC is significantly compressed by the large cyst (arrowhead).CT: computed tomography; IVC: inferior vena cava.
Intraoperative findings.a) The large cyst originated from the sigmoid mesentery.b) Post-enucleation image of the abdominal cavity showing that only the cyst was removed without damage to the ureter or other parts of the colon.
Resected specimen.a) The cyst measured 210 160 mm and was covered by a relatively thick fibrous capsule. The cystic fluid was old bloody.b) Histological image of the cyst wall showing the cystic lumen covered with fibrin, blood, and degenerative material. No epithelial or endothelial cells were present. The cyst wall was composed of fibrous connective tissue with numerous neutrophilic infiltrates.
Discussion
Infectious pseudo-mesenteric cysts have been reported infrequently, and the mechanism of infection has not been clarified ^(3)^. Some reports cite bacterial translocation as the most likely route of infection ^(3), (4)^. In the present case, there was no obvious connection between the cyst and the intestinal tract, and the bacterial culture of the cystic fluid detected intestinal bacteria, suggesting that intestinal bacteria had invaded the cyst for some reason. The most recent report on pseudo-mesenteric cysts in Japan summarizes cases from 1988 to 2021 ^(5)^. Including other reports and self-experimental cases, a total of 27 cases from 2000 to 2024 are listed in Table 1 ^(6), (7), (8)^. Regarding surgery, laparoscopic surgery was performed in 10 cases. The cyst diameters ranged from 40 mm to 210 mm (median, 100 mm) in laparotomy cases and from 35 mm to 210 mm (median, 47 mm) in laparoscopic cases. Case 13 involved a large cyst with a diameter of 210 mm, but laparoscopic cyst enucleation was performed. Initially, puncture drainage of the cyst was carried out, followed by laparoscopic enucleation ^(9)^. In our case, the cyst was severely inflamed. Severe inflammation makes dissection difficult. There is a risk of massive hemorrhage, so laparotomy was performed. The cyst diameters ranged from 42 mm to 150 mm (median, 105 mm) in patients who underwent complicated bowel resections, while they ranged from 35 mm to 210 mm (median, 55 mm) in patients without complicated bowel resections.
In our case, the cyst was large enough to consider bowel resection. However, preoperative imaging showed no significant features within the cyst to suggest malignancy, and the cyst wall appeared relatively thick. A decision was made to perform cyst enucleation, which was successfully completed through careful dissection along the cyst wall, without major vascular injury or the need for bowel resection.
Article Information
Author Contributions
Takeshi Utsunomiya, Atsushi Takada, and Hirotsugu Yoshiyama performed the surgical procedures. Takeshi Utsunomiya, Ryo Karasudani, Naho Ishimura, Shigehiko Yagi, and Masayuki Kanzaki joined the data interpretation. Takeshi Utsunomiya drafted the manuscript. Jota Watanabe, Hiromi Ohtani, and Satoshi Sumida were involved in key revisions of the manuscript. Hiromi Ohtani joined the final approval of the manuscript. All authors are in agreement regarding the consent of the manuscript. All authors read and approved the final manuscript.
Conflicts of Interest
None
Approval by Institutional Review Board (IRB)
Not applicable.
Informed Consent
The patient authorized the publication of the case while requesting the confidentiality of his identity.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kurtz RJ, Heimann TM, Holt J, et al. Mesenteric and retroperitoneal cysts. Ann Surg. 1986;203(1):109-12.3942415 10.1097/00000658-198601000-00017 PMC 1251046 · doi ↗ · pubmed ↗
- 2Hirajima S, Kobayashi H, Yanagisawa A, et al. Case of mesenteric cyst in which resection was performed under suspicion of an infection. J Abdom Emerg Med. 2021;41(1):103-5. Japanese.
- 3Tomioku M, Saito G, Okada K, et al. A mesenteric pseudocyst of the mesocolon. Nihon Rinsho Geka Gakkai Zasshi (J Jpn Surg Assoc). 2017;78(2):340-6. Japanese.
- 4Nishiyama M, Sunami T, Yoshida M, et al. A case of laparoscopic resection of mesenteric pseudocyst of the small intestine. Nihon Rinsho Geka Gakkai Zasshi (J Jpn Surg Assoc). 2022;83(6):1067-72. Japanese.
- 5Ooiwa T, Ooiwa H, Yamashita Y, et al. A case of pseudomesenteric cyst arising in the mesentery of the small intestine. Jpn J Exp Med. 2017;94:1148-50. Japanese.
- 6Kotani H, Matsubara K, Kaneko H, et al. Two cases of rare pelvic cyst diagnosed after laparoscopic cystectomy. Jpn J Gynecol Obstet Endosc. 2018;34(1):159-63. Japanese.
- 7Komada S, Kondo S, Iwadare T, et al. A case of mesenteric pseudocyst with acute abdomen. Med J Nagano Mun Hp. 2020;5:69-73. Japanese.
- 8Suzuki K, Chiba S, Nakajima K, et al. Laparoscopic resection of a mesenteric pseudocyst. Jpn J Gastroenterol Surg. 2010;43(6):685-90. Japanese.