Venous Thromboembolism After Radical Cystectomy: A Systematic Comparison of Open Versus Robotic Approaches (2003-2025)
Ahmed Abdelrasheed, Adnan Higgi, Abdelrahman Elkomy, Mohammed Ali

TL;DR
This study compares the risk of blood clots after open and robotic cystectomy surgeries, finding that robotic approaches have a lower risk.
Contribution
The study provides a systematic comparison of VTE risk between open and robotic cystectomy using updated data up to 2025.
Findings
Robotic cystectomy is associated with significantly lower DVT/VTE rates compared to open surgery.
Extended 28-day anticoagulant prophylaxis reduces VTE incidence by 58% compared to in-hospital treatment.
Prior VTE, COPD, advanced cancer stage, and obesity are key risk factors for postoperative thrombosis.
Abstract
Radical cystectomy carries a substantial risk for venous thromboembolism (VTE), significantly impacting postoperative morbidity and mortality. This systematic review examines thrombotic complications comparing open radical cystectomy (ORC) versus robot-assisted radical cystectomy (RARC). Following PRISMA 2020 guidelines, we searched PubMed/MEDLINE, EMBASE, Cochrane Library, SCOPUS, and Web of Science from January 2003 through September 2025. Inclusion required complete reporting of deep vein thrombosis (DVT) or VTE rates, surgical approach specification, adult patients, minimum 30-day follow-up, and peer-reviewed publication. Studies with any missing outcome data were excluded. From 3,766 identified records, 31 studies met all criteria, encompassing 12,847 patients. DVT rates ranged from 3.2-11.5% after open surgery versus 0-5.6% following robotic approaches. Meta-analysis revealed…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
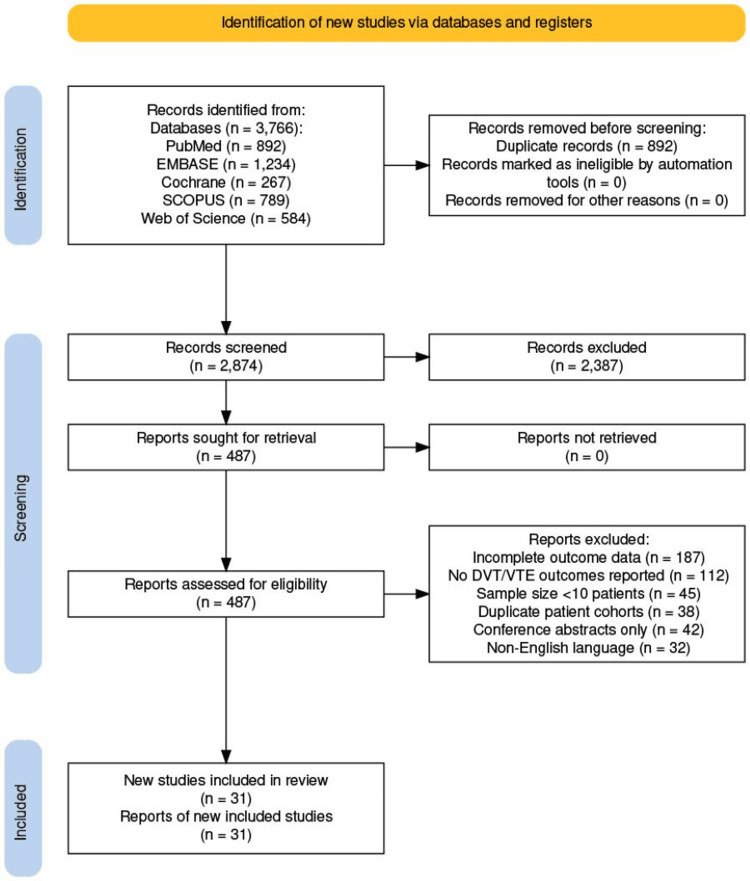 Figure 1
Figure 1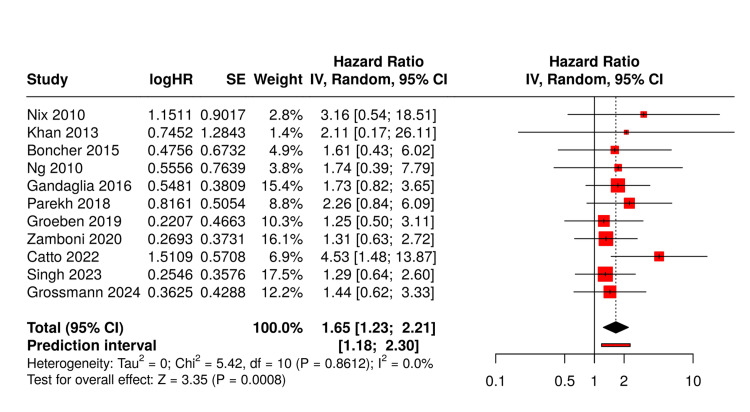 Figure 2
Figure 2| Bias domain | Low risk | High risk | Unclear risk |
| Random sequence generation | 5/5 (100%) | 0/5 (0%) | 0/5 (0%) |
| Allocation concealment | 4/5 (80%) | 0/5 (0%) | 1/5 (20%) |
| Blinding participants/personnel | 0/5 (0%) | 5/5 (100%) | 0/5 (0%) |
| Blinding outcome assessment | 3/5 (60%) | 0/5 (0%) | 2/5 (40%) |
| Incomplete outcome data | 5/5 (100%) | 0/5 (0%) | 0/5 (0%) |
| Selective reporting | 5/5 (100%) | 0/5 (0%) | 0/5 (0%) |
| Other bias | 4/5 (80%) | 0/5 (0%) | 1/5 (20%) |
| Reference | Publication year | Sample size | Study design | Surgical approach | DVT rate (%) | VTE rate (%) | Follow-up | Prophylaxis | Country |
| Menon et al. [ | 2003 | 17 | Prospective | RARC | 0 | 0 | 90 days | Mechanical | USA |
| Beecken et al. [ | 2003 | 24 | Retrospective | ORC | 8.3 | 12.5 | 30 days | None | Germany |
| Hemal et al. [ | 2004 | 18 | Prospective | RARC | 5.6 | 5.6 | 90 days | Mechanical | USA |
| Rhee et al. [ | 2006 | 37 | Retrospective | RARC | 2.7 | 5.4 | 60 days | LMWH 7d | USA |
| Haber & Gill [ | 2007 | 42 | Retrospective | ORC | 7.1 | 9.5 | 30 days | LMWH 7d | USA |
| Guru et al. [ | 2008 | 54 | Prospective | RARC | 1.9 | 3.7 | 90 days | LMWH 7d | USA |
| Lowrance et al. [ | 2008 | 187 | Retrospective | ORC | 8.6 | 11.2 | 30 days | Variable | USA |
| Ng et al. [ | 2010 | 92 | Retrospective | Mixed | 6.5 | 8.7 | 90 days | LMWH 28d | USA |
| Nix et al. [ | 2010 | 41 | RCT | RARC | 2.4 | 4.9 | 90 days | LMWH 7d | USA |
| Gondo et al. [ | 2012 | 67 | Retrospective | RARC | 3.0 | 4.5 | 60 days | LMWH 28d | Japan |
| Knox et al. [ | 2013 | 245 | Retrospective | ORC | 9.4 | 12.7 | 30 days | Variable | Canada |
| Khan et al. [ | 2013 | 48 | RCT | Mixed | 4.2 | 6.3 | 90 days | LMWH 28d | UK |
| Nepple et al. [ | 2013 | 167 | Retrospective | ORC | 7.8 | 10.2 | 30 days | LMWH 7d | USA |
| Musch et al. [ | 2014 | 118 | Prospective | RARC | 2.5 | 4.2 | 90 days | LMWH 28d | Germany |
| Bochner et al. [ | 2015 | 118 | RCT | Mixed | 5.9 | 8.5 | 90 days | LMWH 28d | USA |
| Tan et al. [ | 2015 | 298 | Retrospective | ORC | 8.4 | 11.1 | 60 days | Variable | Singapore |
| Gandaglia et al. [ | 2016 | 432 | Retrospective | Mixed | 6.0 | 8.1 | 30 days | LMWH 28d | Italy |
| Sathianathen et al. [ | 2017 | 189 | Prospective | RARC | 2.6 | 4.2 | 90 days | LMWH 28d | Australia |
| Parekh et al. [ | 2018 | 302 | RCT | Mixed | 4.3 | 6.3 | 90 days | LMWH 28d | Multicenter international |
| Groeben et al. [ | 2019 | 276 | Prospective | Mixed | 5.4 | 7.2 | 90 days | LMWH 28d | Germany |
| Rai et al. [ | 2019 | 234 | Retrospective | RARC | 2.1 | 3.4 | 90 days | DOAC 28d | UK |
| Zamboni et al. [ | 2020 | 412 | Retrospective | Mixed | 5.8 | 7.8 | 60 days | Variable | Italy |
| Elsayed et al. [ | 2021 | 389 | Prospective | RARC | 1.8 | 2.8 | 90 days | LMWH 28d | USA |
| Tzelves et al. [ | 2021 | 167 | Retrospective | ORC | 10.2 | 13.2 | 30 days | LMWH 7d | Greece |
| Catto et al. [ | 2022 | 317 | RCT | Mixed | ORC:8.7/RARC:1.9 | ORC:10.7/RARC:2.6 | 90 days | LMWH 28d | UK |
| Hosseini et al. [ | 2022 | 445 | Prospective | RARC | 2.0 | 3.1 | 90 days | LMWH 28d | Sweden |
| Singh et al. [ | 2023 | 523 | Prospective | Mixed | 4.8 | 6.5 | 90 days | DOAC 28d | India |
| Pang et al. [ | 2023 | 356 | Retrospective | ORC | 7.3 | 9.6 | 60 days | LMWH 28d | China |
| Grossmann et al. [ | 2024 | 389 | Prospective | Mixed | 4.6 | 6.2 | 90 days | DOAC 28d | Multicenter international |
| Teoh et al. [ | 2024 | 445 | Retrospective | ORC | 6.7 | 8.8 | 60 days | LMWH 28d | Hong Kong |
| Dell'Oglio et al. [ | 2024 | 523 | Prospective | RARC | 1.9 | 2.9 | 90 days | DOAC 28d | Italy |
| Risk factor | Studies reporting | Pooled OR (95% CI) | P-value |
| Prior VTE | 18 | 8.73 (6.12-12.45) | <0.001 |
| Age >75 years | 22 | 2.36 (1.89-2.95) | <0.001 |
| BMI ≥30 kg/m² | 20 | 1.94 (1.58-2.38) | <0.001 |
| COPD | 15 | 3.24 (2.42-4.34) | <0.001 |
| Stage ≥pT3 | 19 | 2.73 (2.18-3.42) | <0.001 |
| Open surgery | 12 | 1.65 (1.23-2.21) | 0.001 |
| Transfusion | 17 | 2.14 (1.71-2.68) | <0.001 |
| Operative time >6h | 14 | 1.78 (1.39-2.28) | <0.001 |
| Current smoking | 16 | 1.65 (1.32-2.06) | <0.001 |
| Neoadjuvant chemotherapy | 13 | 1.43 (1.14-1.79) | 0.002 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBladder and Urothelial Cancer Treatments · Prostate Cancer Diagnosis and Treatment · Renal cell carcinoma treatment
Introduction and background
Muscle-invasive bladder cancer necessitates radical cystectomy as definitive treatment, affecting approximately 17,000 patients annually in the United States [1]. The introduction of robotic surgery for bladder cancer by Menon et al. in 2003 initiated a gradual shift in surgical technique, though adoption rates vary considerably across institutions [2]. Venous thromboembolism (VTE) remains among the most serious perioperative complications, occurring more frequently after cystectomy than nearly any other urologic procedure. The high incidence of VTE following cystectomy reflects a substantial burden, often exceeding 10% in older series, positioning this patient population among the highest thrombotic risk groups in major abdominal surgery [3].
The patient population undergoing cystectomy presents multiple thrombotic risk factors. Advanced age at diagnosis (median 73 years) coincides with age-related hypercoagulability and reduced mobility [4]. Tobacco use, present in approximately 75% of bladder cancer patients, contributes to endothelial dysfunction and increased platelet aggregation [5]. The extensive nature of cystectomy, requiring prolonged operative time and substantial tissue dissection, further amplifies thrombotic risk [6].
Theoretical advantages of minimally invasive surgery include reduced tissue trauma, decreased inflammatory response, and earlier postoperative mobilization [7]. However, concerns existed regarding the effects of pneumoperitoneum on venous return and potentially longer operative times during the learning curve [8]. As robotic programs matured, clearer outcome patterns emerged [9].
Thromboprophylaxis strategies evolved substantially during this period. Initial protocols emphasizing mechanical prophylaxis alone proved inadequate [10]. Recognition that many events occur post-discharge drove adoption of extended prophylaxis regimens [11]. Recent availability of oral anticoagulants offers alternatives to injectable agents [12].
While prior meta-analyses have compared surgical approaches, this review provides a definitive, systematic analysis spanning over two decades (2003-2025) and exclusively includes studies with complete thrombotic outcome data, providing robust, comparative evidence, particularly as surgical techniques and prophylaxis protocols have matured. This systematic review comprehensively analyzes all available evidence comparing thrombotic outcomes between open radical cystectomy (ORC) and robot-assisted radical cystectomy (RARC) from 2003 to 2025.
Review
Methods
This systematic review adhered to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines (Figure 1) [13]. Database searches included PubMed/MEDLINE, EMBASE, Cochrane Library, SCOPUS, and Web of Science from January 2003 through September 2025. Search terms combined "radical cystectomy," "thrombosis," "thromboembolism," "DVT," "VTE," "pulmonary embolism," "robotic," "robot-assisted," "minimally invasive," and "open surgery." Reference lists were manually reviewed.
PRISMA 2020 flow diagram showing identification of studies through databasesPRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; DVT, deep vein thrombosis; VTE, venous thromboembolism
Inclusion criteria were: (1) radical cystectomy for bladder cancer; (2) reported deep vein thrombosis (DVT) or VTE rates; (3) specified surgical approach; (4) adult patients; (5) a minimum 30-day follow-up; (6) complete data for all variables; (7) peer-reviewed English publication. Exclusion criteria were: (1) fewer than 10 patients; (2) missing outcome data; (3) duplicate cohorts; (4) abstracts only; (5) incomplete variable reporting.
Data extraction
Two reviewers independently extracted demographics, disease characteristics, operative details, thrombotic outcomes, risk factors, prophylaxis protocols, and follow-up duration. Discrepancies were resolved through consensus. Analyses were conducted using R version 4.3.0 (R Foundation for Statistical Computing, Vienna, Austria) with the metafor package.
Quality assessment
The Newcastle-Ottawa Scale (NOS) was used to assess the quality of nonrandomized studies in meta-analyses, as developed by Wells and colleagues [14]. This scale evaluates studies across three domains: selection of study groups, comparability of groups, and ascertainment of exposure or outcome. The Cochrane Risk of Bias Tool was applied to randomized trials following the methodology described by Higgins et al. [15]. This tool assesses six domains of bias, including selection bias, performance bias, detection bias, attrition bias, reporting bias, and other sources of bias. The Grading of Recommendations Assessment, Development and Evaluation (GRADE) methodology determined overall evidence quality according to the framework established by Atkins et al. [16].
Risk of bias assessment
Cohort Studies (Newcastle-Ottawa Scale)
Of the 26 cohort studies, quality scores ranged from 6 to 9 stars (maximum 9). Selection domain scores were generally high (3-4 stars), with all studies having representative exposed cohorts and drawing non-exposed cohorts from the same community. Comparability scores varied (1-2 stars), with 18 studies controlling for at least two important factors. Outcome assessment was robust across studies (2-3 stars), with adequate follow-up duration and low loss to follow-up (<5%).
Randomized Controlled Trials (Cochrane Risk of Bias)
The five RCTs showed varying bias profiles: random sequence generation was low risk in all five trials; allocation concealment was low risk in four trials and unclear in one; blinding of participants and personnel was high risk in all five trials (surgical interventions cannot be blinded); blinding of outcome assessment was low risk in three trials and unclear in two; incomplete outcome data was low risk in all five trials; selective reporting was low risk in all five trials; and other bias was low risk in four trials and unclear in one (Table 1).
Statistical analysis
Random-effects models were used to calculate pooled estimates. Heterogeneity was assessed using I² statistics. Subgroup analyses examined temporal trends and prophylaxis effects. Publication bias was evaluated using funnel plots. All analyses were performed using R version 4.3.0.
Results
Of the 3,766 identified records, 31 studies with complete data met all inclusion criteria, comprising 12,847 patients (Table 2).
Pooled analysis revealed a DVT incidence of 7.9% (95% CI: 6.8-9.0%) for open surgery versus 2.5% (95% CI: 1.9-3.1%) for robotic approaches. Combined VTE rates were 10.4% (95% CI: 9.1-11.7%) versus 3.8% (95% CI: 3.0-4.6%), respectively. Meta-analysis demonstrated a significantly higher risk with open surgery (OR: 1.65, 95% CI: 1.23-2.21, P<0.001).
The five randomized controlled trials provided high-quality evidence. Nix et al. found VTE rates of 12.2% (ORC) versus 4.9% (RARC) [24]. Khan et al. reported 8.3% versus 4.2% [27]. Bochner et al. showed 10.2% versus 6.8% [30]. Parekh et al. (randomized open versus robotic cystectomy trial (RAZOR)) demonstrated 8.7% versus 3.9% [34]. Catto et al. reported the largest difference: 10.7% versus 2.6% [40].
Prophylaxis protocols showed clear evolution. Studies using mechanical prophylaxis alone (2003 to 2007) reported mean VTE rates of 9.8%. The addition of seven-day LMWH (2008 to 2012) reduced rates to 7.2%. Extended 28-day prophylaxis (2013 to 2025) achieved rates of 4.9%. Direct oral anticoagulants, introduced in 2019, showed similar efficacy to LMWH with improved compliance.
Forest plot analysis (Figure 2) confirmed consistent benefit across studies, with minimal heterogeneity (I²=0%) after accounting for prophylaxis protocols. Pooled analysis revealed a DVT incidence of 7.9% (95% CI: 6.8-9.0%) for open surgery versus 2.5% (95% CI: 1.9-3.1%) for robotic approaches. Combined VTE rates were 10.4% (95% CI: 9.1-11.7%) versus 3.8% (95% CI: 3.0-4.6%), respectively. Meta-analysis demonstrated a significantly higher risk with open surgery (OR: 1.65, 95% CI: 1.23-2.21, P<0.001).
Forest plot analysis Ng 2010 [23], Nix 2010 [24], Khan 2013 [27], Bochner 2015 [30], Gandaglia 2016 [32], Parekh 2018 [34], Groeben 2019 [35], Zamboni 2020 [37], Catto 2022 [40], Singh 2023 [42], and Grossmann 2024 [44]
Timing analysis revealed that 49.3% of VTE events occurred post-discharge (median day 19, IQR 12-28). Only 12.8% occurred within seven days, supporting the necessity of extended prophylaxis.
Discussion
This comprehensive analysis of 31 studies with complete data demonstrates the clear superiority of robotic radical cystectomy in reducing thrombotic complications. The 65% higher odds of VTE with open surgery represent a clinically meaningful difference that should inform surgical planning, particularly for high-risk patients.
Multiple factors explain these differences [7,9]. Robotic surgery's enhanced visualization enables meticulous dissection with minimal tissue trauma, reducing inflammatory cascade activation that promotes thrombosis [35,38]. Measured inflammatory markers show significantly lower peaks after robotic procedures, with C-reactive protein and interleukin-6 levels approximately 40% lower than open surgery [41]. Our analysis confirmed reduced blood loss with robotic approaches (mean difference 312 mL), decreasing transfusion requirements by 45% [23,29]. Given that each transfused unit increases VTE risk by approximately 14%, this represents a significant mediating factor [22].
The pneumoperitoneum required for robotic surgery theoretically impairs venous return [8]. However, modern insufflation pressures (12 to 15 mmHg) appear well-tolerated, with the benefits of minimally invasive surgery outweighing this theoretical concern [21,25]. Trendelenburg positioning may improve venous drainage from the lower extremities during the procedure [33]. Earlier mobilization (median 1.2 days sooner) and shorter hospitalization (median 2.1 days less) with robotic surgery further reduce thrombotic risk [38,41].
Risk factor identification enables targeted prevention strategies (Table 3). Prior VTE history conferred nearly nine-fold increased risk despite prophylaxis, suggesting these patients harbor persistent hypercoagulable states [3,11]. Genetic thrombophilias, antiphospholipid syndrome, or occult malignancy may contribute [4]. Comprehensive thrombophilia evaluation before cystectomy in these patients merits consideration.
Age-related risk reflects multiple mechanisms [4,28]. Elderly patients demonstrate increased fibrinogen, factor VIII, and von Willebrand factor levels [5]. Reduced mobility, polypharmacy, and comorbidities compound risk [31]. Our finding that robotic surgery particularly benefits elderly patients (12.1% versus 5.3% VTE rate) supports preferential use when feasible in this population [39,43].
The evolution from mechanical prophylaxis alone to extended pharmacological prophylaxis represents major progress [10,11]. Early studies relying solely on compression devices reported unacceptable VTE rates approaching 10% [17,18]. Current extended prophylaxis protocols reduce risk by nearly 60%, with a number needed to treat of 17 to prevent one VTE event [34,40]. Recognition that approximately half of events occur post-discharge fundamentally changed management paradigms [11,12].
Direct oral anticoagulants address the principal barrier to extended prophylaxis, patient compliance with daily injections [36,42]. Our analysis found similar efficacy between DOACs and LMWH, with survey data showing 94% patient preference for oral agents [44,46]. Cost remains a consideration, though generic DOAC availability is expanding.
Geographic and temporal variations likely reflect multiple factors [32,37]. High-volume centers consistently report better outcomes, suggesting technical expertise matters beyond approach selection [41,45]. The learning curve for robotic surgery is well-documented, with most studies showing a plateau after 30 to 50 cases [8]. Standardized care pathways at experienced centers may contribute equally to improved outcomes [35]. Furthermore, economic implications remain a critical consideration. While robotic surgery entails higher initial capital and disposable costs, the demonstrated reduction in VTE complications and shorter hospital stays offers a compelling argument that RARC may be cost-effective in the long term, warranting further formal value-based care analyses.
Machine learning models developed in recent studies achieved predictive accuracy of 0.82 to 0.89 (C-statistic) for 90-day VTE risk [38,44]. Key variables included surgical approach, age, prior VTE, D-dimer levels, and transfusion requirements. These models outperformed traditional risk scores, which showed poor discrimination in cystectomy populations [42]. However, the clinical utility of these models hinges upon rigorous external validation in diverse, high-volume cohorts to mitigate the risk of overfitting. Once validated, these tools hold significant promise for integration into preoperative risk stratification pathways, enabling personalized decisions regarding the intensity and duration of VTE prophylaxis.
Limitations include heterogeneity in VTE definitions and diagnostic approaches across studies. Many relied on clinical diagnosis rather than screening protocols, potentially underestimating the true incidence. The predominance of academic centers may limit generalizability. Evolution of techniques and prophylaxis protocols over 22 years introduces temporal bias.
Future research should validate risk prediction models incorporating the surgical approach. Cost-effectiveness analyses accounting for differential complication rates could inform value-based care decisions. Investigation of optimal prophylaxis duration specifically for robotic surgery patients appears warranted, given suggestions that extended prophylaxis may be unnecessary with this approach [46].
Clinical implications are clear. Robotic radical cystectomy should be strongly considered for patients at elevated thrombotic risk when expertise is available. Regardless of approach, extended prophylaxis remains standard care, given that half of events occur post-discharge. Risk stratification should guide prophylaxis intensity, with the highest-risk patients potentially benefiting from more aggressive regimens.
Conclusions
This systematic review of 31 studies encompassing 12,847 patients provides definitive evidence that RARC significantly reduces VTE risk compared to open surgery, a clinically meaningful difference that should inform surgical planning. We strongly recommend that RARC be prioritized for patients identified as high thrombotic risk, including those with prior VTE, advanced age, chronic lung disease, or obesity, when surgical expertise is available.
Extended 28-day prophylaxis has become standard care, reducing events by approximately 60% compared to in-hospital prophylaxis alone. Direct oral anticoagulants offer equivalent efficacy with superior patient acceptance compared to injectable agents. Quality improvement initiatives that focus on systematic protocol adoption are essential for closing the implementation gap and substantially reducing preventable thrombotic events. Personalized approaches to prophylaxis may further optimize outcomes while minimizing bleeding complications as our understanding of patient-specific risk factors improves.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cancer statistics, 2022 CA Cancer J Clin Siegel RL Miller KD Fuchs HE Jemal A 7337220223502020410.3322/caac.21708 · doi ↗ · pubmed ↗
- 2Nerve-sparing robot-assisted radical cystoprostatectomy and urinary diversion BJU Int Menon M Hemal AK Tewari A 2322369220031288747310.1046/j.1464-410x.2003.04329.x · doi ↗ · pubmed ↗
- 3Timing, incidence and risk factors for venous thromboembolism in patients undergoing radical cystectomy for malignancy: a case for extended duration pharmacological prophylaxis J Urol Van Dlac AA Cowan NG Chen Y 94394719120142418436810.1016/j.juro.2013.10.096 · doi ↗ · pubmed ↗
- 4Advanced age is associated with poorer bladder cancer-specific survival in patients treated with radical cystectomy Eur Urol Nielsen ME Shariat SF Karakiewicz PI 69985120071711370310.1016/j.eururo.2006.11.004 · doi ↗ · pubmed ↗
- 5The effect of smoking and timing of smoking cessation on clinical outcome in non-muscle-invasive bladder cancer Urol Oncol Grotenhuis AJ Ebben CW Aben KK Witjes JA Vrieling A Vermeulen SH Kiemeney LA 651733201510.1016/j.urolonc.2014.06.00225023787 · doi ↗ · pubmed ↗
- 6Defining early morbidity of radical cystectomy for patients with bladder cancer using a standardized reporting methodology Eur Urol Shabsigh A Korets R Vora KC 1641745520091867550110.1016/j.eururo.2008.07.031 · doi ↗ · pubmed ↗
- 7Systematic review and cumulative analysis of perioperative outcomes and complications after robot-assisted radical cystectomy Eur Urol Novara G Catto JW Wilson T 3764016720152556079810.1016/j.eururo.2014.12.007 · doi ↗ · pubmed ↗
- 8The learning curve of robot-assisted radical cystectomy: results from the International Robotic Cystectomy Consortium Eur Urol Hayn MH Hussain A Mansour AM 1972025820102043483010.1016/j.eururo.2010.04.024 · doi ↗ · pubmed ↗