Venoarterial Extracorporeal Membrane Oxygenation-Assisted Whole-Lung Lavage for Near Drowning With Massive Sand Aspiration: A Case Report
Tsuyoshi Suzuki, Chiaki Nemoto, Reiko Okubo, Makoto Onodera, Ken Iseki

TL;DR
A patient who nearly drowned and aspirated sand was successfully treated with whole-lung lavage supported by extracorporeal membrane oxygenation.
Contribution
Demonstrates the use of VA-ECMO-assisted whole-lung lavage for severe sand aspiration in a patient with impaired cardiac function.
Findings
VA-ECMO-assisted whole-lung lavage successfully cleared aspirated sand in a near-drowning case.
The patient's respiratory function improved and he regained communication ability after the procedure.
VA-ECMO support may be a safer approach for whole-lung lavage in patients with compromised cardiac function.
Abstract
Sand aspiration during drowning can cause tracheobronchial obstruction and severe respiratory failure. In life-threatening hypoxemia, there is currently no established method for the safe removal of aspirated sand. We report a case of a 50-year-old man with hypertension and angina pectoris who nearly drowned while surfing. Upon arrival at the hospital, he was unconscious, hypoxemic, and hypothermic. Chest computed tomography revealed extensive bilateral dorsal infiltrates and high-density material within the bronchi. Despite repeated suctioning of the foul-smelling sand, the partial pressure of arterial oxygen (PaO2)/fraction of inspired oxygen (FiO₂) (P/F) ratio remained less than 100 even with an FiO₂ of 1.0, necessitating whole-lung lavage (WLL). Transthoracic echocardiography (TTE) revealed severely impaired cardiac function. Because of the risk of cardiac arrest, WLL was initiated…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
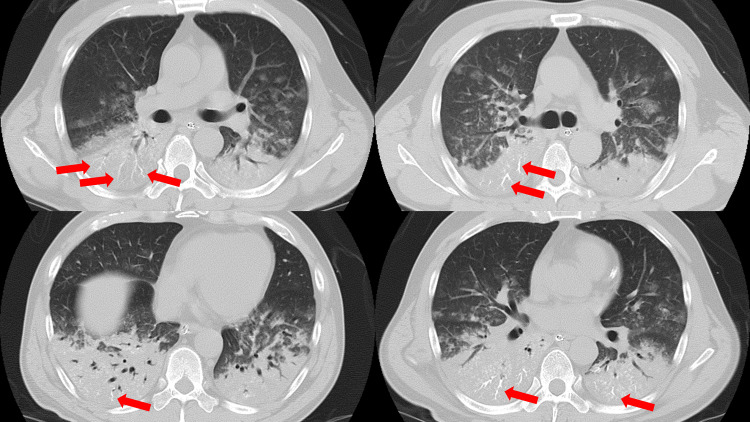 Figure 1
Figure 1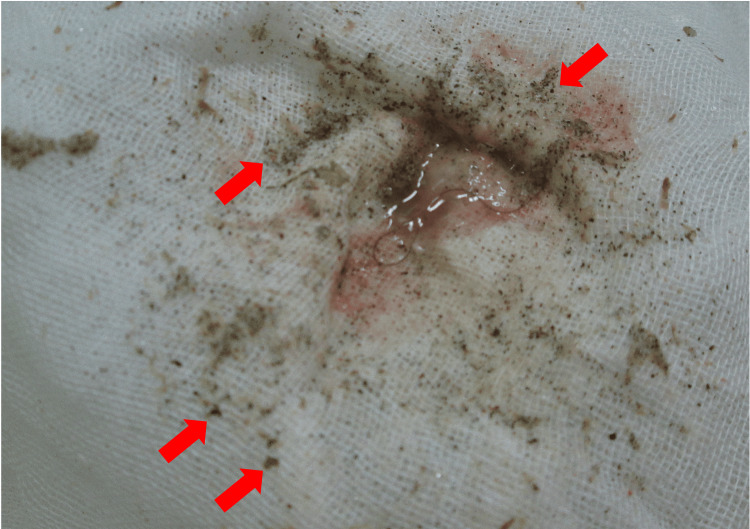 Figure 2
Figure 2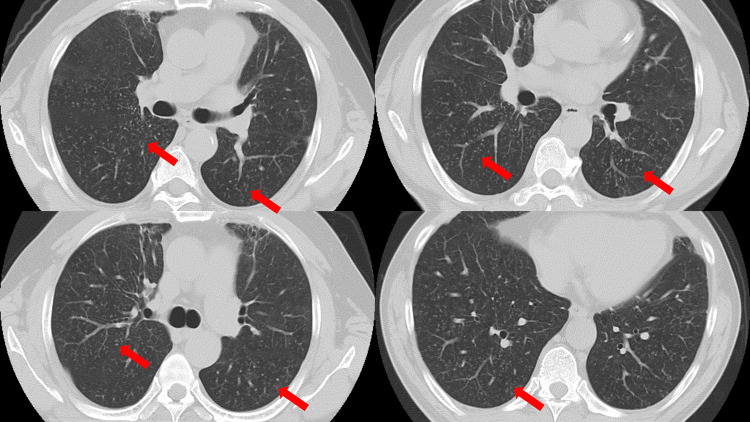 Figure 3
Figure 3| Laboratory parameters | Value | Reference range |
| WBC | 2.4 | 3.8-9.8(x103/μL) |
| Hemoglobin | 17.2 | 13.2-16.8(g/dL) |
| PLT | 33.6 | 14.7-34.1(x104/μL) |
| PT | 90.2 | 70-125(%) |
| APTT | 24.4 | 23-38(sec) |
| Total protein | 7.6 | 6.7-8.3(g/dL) |
| Serum albumin | 4.3 | 3.9-4.9(g/dL) |
| Creatinine | 1 | 0.6-1.1(mg/dL) |
| AST | 44 | 10-38(U/L) |
| ALT | 57 | 8-42(U/L) |
| Total bilirubin | 0.5 | 0.2-1.2mg/dL) |
| Sodium | 155 | 138-146(mEq/L) |
| Potassium | 4.2 | 3.6-4.9(mEq/L) |
| Chloride | 125 | 99-106(mEq/L) |
| Troponin I | <0.017 | 0.00-0.056(ng/mL) |
| BNP | 14.3 | 0.0-18.4(pg/mL) |
| CRP | 7.04 | <0.03(mg/dL) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInjury Epidemiology and Prevention · Cardiovascular and Diving-Related Complications · Neonatal Respiratory Health Research
Introduction
In outdoor drowning, not only microorganisms but also particulate matter, such as sand and mud, enter the alveoli, leading to airway obstruction. Drowning is a known risk factor for drowning-associated pneumonia (DAP) and acute respiratory distress syndrome. Removing particulate matter from the alveoli and airways is essential to achieve resolution of respiratory failure. Whole-lung lavage (WLL) has been established as an effective method for washing the trachea during pulmonary alveolar proteinosis [1,2]. However, previously, there have been reports of WLL in adults due to aspiration of lubricants [3]; no report has described the use of WLL for near drowning with sand aspiration. Moreover, the indications for WLL in drowning-related, life-threatening respiratory failure due to sand aspiration remain unclear. Here, we describe the successful use of venoarterial extracorporeal membrane oxygenation (VA-ECMO)-assisted WLL in a patient with severe hypoxemia following drowning and massive sand aspiration.
Case presentation
A 50-year-old man with a history of hypertension, angina pectoris, and smoking (20 cigarettes/day) disappeared while surfing. Approximately one hour later, the patient was found unconscious and transferred to a hospital. On arrival, his Glasgow Coma Scale (GCS) score was three, respiratory rate 30 breaths/min, oxygen saturation (SpO_2_) 75% (room air), blood pressure 213/146 mmHg, heart rate 94 beats per minute (bpm), and body temperature 33°C. He had impaired consciousness and hypoxemia and was intubated. During intubation, large amounts of sand and mud were aspirated from the trachea, which were thought to be due to drowning (Figure 1).
Axial chest computed tomography image on admissionExtensive infiltrative shadows were observed in the bilateral dorsal lungs. In addition, there was a high-density finding of gravel and mud in the bronchi of the same area (red arrow).
After intubation, his SpO_2_ remained low at 80% despite a fraction of inspired oxygen (FiO_2_) of 1.0. The patient was transferred to our hospital for intensive care. He remained unconscious and hypoxemic. Blood tests (Table 1) showed a white blood cell count of 2400/µL, hemoglobin 17.2 g/dL, platelet count 33.4×104/µL/µL, prothrombin time/international normalized ratio 1.0, activated partial thromboplastin time 24.4 sec, glutamic oxaloacetic transaminase 44 U/L, glutamic pyruvic transaminase 57 U/L, lactate dehydrogenase 238 U/L, creatinine 1.0 mg/dL, Na^+^ 155 mEq/L, K^+^ 4.2 mEq/L, and Cl 125 mEq/L. Blood gas analysis (FiO_2_ 1.0) showed pH 7.144, partial pressure of arterial oxygen (PaO_2_) 54.2 mmHg, partial pressure of arterial carbon dioxide (PaCO_2_) 56.7 mmHg, and bicarbonate (HCO3) 18.7 mmol/L.
Transthoracic echocardiography (TTE) revealed a left ventricular ejection fraction of 25%-30%; diffuse left ventricular hypokinesis was shown. After admission to the intensive care unit, a large amount of sand was aspirated from the trachea. Therefore, the patient was diagnosed with near drowning with aspirated sand and mud. The presence of hypernatremia also suggested drowning in seawater. Meropenem (1 g every 12 hours) was administered as antibiotic therapy. Invasive positive-pressure ventilation was then initiated (assist-control mode; FiO_2_, 1.0; respiratory rate, 12/min; positive end-expiratory pressure (PEEP), 10 cmH_2_O); however, to achieve a tidal volume of 6 mL・kg⁻¹ of predicted body weight, the peak airway pressure (PAP) reached 40 cmH_2_O, and the PaO_2_/FiO_2_ ratio was <100. Despite several attempts at endotracheal suction over one to two hours, the patient showed no change in PAP and hypoxemia. Thus, endotracheal suctioning was insufficient for sand removal, and WLL was planned. To prepare for WLL, the tracheal tube was changed to a double-lumen tube. Isolated lung ventilation and WLL were planned for the non-ventilated side. However, severe hypoxemia reduced cardiac function on TTE, and worsening hypoxemia during WLL raised concerns about cardiac arrest. Therefore, we decided to initiate VA-ECMO and then perform WLL to remove the aspirated particles. On day 1 of admission, VA-ECMO (MERA centrifugal blood pump system HCS-CFP; Senko Medical Instruments, Tokyo, Japan) was initiated. We inserted a 20 Fr cannula (PCKC-A; MERA Development Corp., Tokyo, Japan) into the right femoral artery and a 24 Fr cannula (PCKC-V; MERA Development Corp) into the right femoral vein and established VA-ECMO (3000 rpm; pump flow 3.0 L/min; O₂ flow 2.0 L/min). WLL was initiated with warm normal saline, and the patient soon experienced cardiac arrest following severe bradycardia. The ECMO flow was increased to 5.1 L/min, followed by resuscitation for a few minutes until return of spontaneous circulation was achieved. We continued the WLL and obtained alveolar lavage fluid that appeared muddy. It smelled foul, and when we filtered it through gauze, we observed numerous small, sand-like particles (Figure 2).
Small particles obtained via the whole lung lavage (WLL)The washing solution obtained during the first WLL cycle, filtered through gauze. Countless small dots, likely sand particles (red arrows), are observed.
The treatment was stopped when the wash solution became clear (5 liters × 5 cycles, total 25 L). Following WLL, PAP decreased to 30 cmH₂O. On day three, cardiac function improved, but severe respiratory failure persisted; therefore, a 24 Fr blood cannula (PCKC-A; MERA Development Corp) was inserted into the right internal jugular vein, and the circuit was converted from VA-ECMO to venovenous (VV) ECMO. On day seven, the patient was weaned off VV-ECMO; however, on day nine, VV-ECMO was reintroduced because of hypercapnia with decreased pulmonary compliance. On day 18, a tracheostomy was performed. On day 30, the patient was weaned off the ventilator. On day 49, he was transferred to the rehabilitation department because of muscle weakness. He fully recovered after hospitalization one year later. Respiratory function tests showed that his vital capacity recovered to 81%, and his forced expiratory volume in one second was three liters. Computed tomography revealed the disappearance of diffuse infiltrative shadows in the lungs, with only a few miliary shadows remaining along the bronchioles (Figure 3).
Axial chest computed tomography image one year laterThe diffuse infiltrative shadow had disappeared, leaving only a slight miliary shadow along the microbronchi.
Discussion
This case demonstrates that WLL under VA-ECMO support can save the lives of patients with severe hypoxemia caused by extensive sand aspiration. In cases of severe hypoxemia with shock, WLL with VA-ECMO may minimize the risk of worsening hypoxemia and cardiovascular instability. No cases of WLL for near drowning with sand aspiration have been reported, and evidence for its safety is lacking. WLL is usually indicated for alveolar proteinosis and is considered an overall safe procedure [1], although complications such as hypoxemia, pleural effusion, and pneumothorax have been reported [4]. Centella et al. reported a case of cardiac arrest after WLL in a young man with alveolar proteinosis and severe hypoxemia [5]. WLL with VV-ECMO was performed after resuscitation. The patient in that case was hypoxemic despite ventilatory management on admission (assist-control mode; pressure control 12 cmH₂O; PEEP 10 cmH₂O; FiO₂ 1.0), with a systolic blood pressure of 80 mmHg and a heart rate of 150 bpm, and was in shock; therefore, WLL was considered difficult to perform. In contrast, sand and mud cause extensive peripheral airway obstruction, resulting in increased airway pressure and severe hypoxemia, making early removal of the aspirated material necessary. In this case, although PAP decreased after the WLL, improvement in oxygenation was insufficient, necessitating a switch to VV-ECMO. While the WLL may have prevented secondary pulmonary barotrauma, it is unclear whether it contributed to reducing pulmonary inflammation.
We performed WLL with VA-ECMO support. VV-ECMO may only be considered for severe hypoxemia without shock. VA-ECMO with preserved left ventricular function is associated with increased cardiac afterload. Once cardiac function improves, switching from VA-ECMO to VV-ECMO, as in this case, may also be beneficial. This procedure should not be applied to all drowning patients who have aspirated sand; its applicability must be carefully considered. It should be carefully evaluated in cases with impaired cardiac function.
WLL and bronchoalveolar lavage (BAL) may also be useful for removing small aspirated materials from the alveoli. Ramirez et al. [6] reported the use of WLL to treat alveolar proteinosis. Recently, Shang et al. [7] reported its use in treating exogenous lipoid pneumonia. In WLL, isolated lung ventilation is performed under general anesthesia, and the non-ventilated lung is washed with saline solution. For alveolar proteinosis, lung lavage is performed until 5-40 liters of saline become clear [8]. In this case, WLL was repeated five times, each time using 5 liters of 37℃ normal saline. However, WLL is not widely used to remove aspirated material in sand aspiration and should be considered only when aspirated material is widely distributed throughout the lung field, endotracheal suctioning is inadequate to remove aspirated material, and hypoxemia is present. In addition, BAL, which is less invasive than WLL, should be considered. In 2009, Kapur et al. [9] performed BAL to remove aspirated sand and administered surfactant. BAL may be more effective than WLL when the aspirated material does not extend to the whole lung field but remains at a certain segmental branch level.
During the WLL procedure, the patient was placed in the prone position. Although several positions for patients undergoing WLL have been reported, the optimal position remains unknown. In alveolar proteinosis, the supine position, the lateral position with the washed lung above, the lateral position with the washed lung below, and the prone position have been reported [2,10]. The aspirated material usually accumulates dorsally rather than ventrally. Because sand has a higher specific gravity than water, the prone position may facilitate dorsal drainage during WLL with sand suction after drowning. In our case, WLL was initially performed in the supine position, but only a small amount of sand was discharged into the wash solution. The patient was then repositioned to the prone position, and sand discharge was successfully achieved. However, careful attention should be paid to circulatory changes associated with changes in position because complications such as hypotension and hypoxemia may occur in the prone position. In this case, the patient was placed in the prone position during VA-ECMO. Although hypotension and hypoxemia developed, the procedure was performed safely with precautions specific to patients on ECMO in the prone position, such as preventing the cannula from kinking and ensuring proper blood suctioning of the ECMO circuit.
Conclusions
Herein, we present a rare case of drowning-related massive sand aspiration successfully managed using VA-ECMO-assisted WLL. This approach may be considered for patients with severe hypoxemia and impaired cardiac function when conventional suction fails. Further studies are required to clarify the safety and efficacy of this strategy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Efficacy and safety of whole-lung lavage for pulmonary alveolar proteinosis: a protocol for a systematic review and meta-analysis BMJ Open Liu S Cui X Xia K Duan Y Xiong M Li G 012202210.1136/bmjopen-2021-057671 PMC 902177235443958 · doi ↗ · pubmed ↗
- 2Bilateral whole lung lavage in pulmonary alveolar proteinosis-a retrospective study Rev Port Pneumol Silva A Moreto A Pinho C Magalhães A Morais A Fiuza C 2542592020142504229110.1016/j.rppneu.2014.04.004 · doi ↗ · pubmed ↗
- 3Management of a case of oil drowning with whole lung lavage-challenges and solutions Indian J Anaesth Thondebhavi SM Himashweta G Agarwal D Mehta R 7057066520213476450910.4103/ija.IJA_1_21PMC 8577710 · doi ↗ · pubmed ↗
- 4Whole lung lavage-technical details, challenges and management of complications J Thorac Dis Awab A Khan MS Youness HA 16971706920172874068610.21037/jtd.2017.04.10PMC 5506114 · doi ↗ · pubmed ↗
- 5The use of a membrane oxygenator with extracorporeal circulation in bronchoalveolar lavage for alveolar proteinosis Interact Cardiovasc Thorac Surg Centella T Oliva E Andrade IG Epeldegui A 447449420051767045410.1510/icvts.2005.110320 · doi ↗ · pubmed ↗
- 6Pulmonary alveolar proteinosis: a new technique and rationale for treatment Arch Intern Med RAJ SCRB DURE 41943111219631404529010.1001/archinte.1963.03860030173021 · doi ↗ · pubmed ↗
- 7The efficacy and safety of therapeutic lung lavage for exogenous lipoid pneumonia: a systematic review Clin Respir J Shang L Gu X Du S Wang Y Cao B Wang C 1341461520213294039910.1111/crj.13273 · doi ↗ · pubmed ↗
- 8Whole lung lavage therapy for pulmonary alveolar proteinosis: a global survey of current practices and procedures Orphanet J Rare Dis Campo I Luisetti M Griese M 1151120162757792610.1186/s 13023-016-0497-9PMC 5006612 · doi ↗ · pubmed ↗