The Impact of Preoperative Hepatic Impairment on the Development of Postoperative Delirium: A Systematic Review and Meta-Analysis
Will S Roberts, Vaibhav Mittal, Michael N Ryan, Alexander D Knight, Sarah Schaffer, Andrew Clifford, Jean-Pierre P Ouanes

TL;DR
This study finds that preoperative liver problems increase the risk of post-surgery delirium, but specific biomarkers like bilirubin are not significant.
Contribution
This is the first systematic review and meta-analysis quantifying the risk of postoperative delirium from specific hepatic impairments.
Findings
History of alcohol consumption increases POD risk (OR: 2.59).
History of hepatic encephalopathy increases POD risk (OR: 3.42).
MELD score ≥15 increases POD risk (OR: 3.73).
Abstract
Postoperative delirium (POD) is one of the most common psychiatric and neurologic complications experienced by patients undergoing general anesthesia. While it is widely hypothesized that hepatic impairment is associated with POD, the increased risk that various forms of preoperative hepatic impairment contribute to the development of POD is not well defined in the literature. A database search was performed on Embase, Web of Science, and MEDLINE-PubMed searching for articles containing keywords regarding the association between hepatic impairment and POD, ultimately yielding 34 studies for inclusion. Adjusted odds ratios (ORs) were extracted, with two-sided p-values <0.05 deemed significant. A total of 12,089 patients were included in this review, of which 2,663 developed POD (overall incidence of 22.03%). Inverse variance random-effects meta-analysis reveals that history of alcohol…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
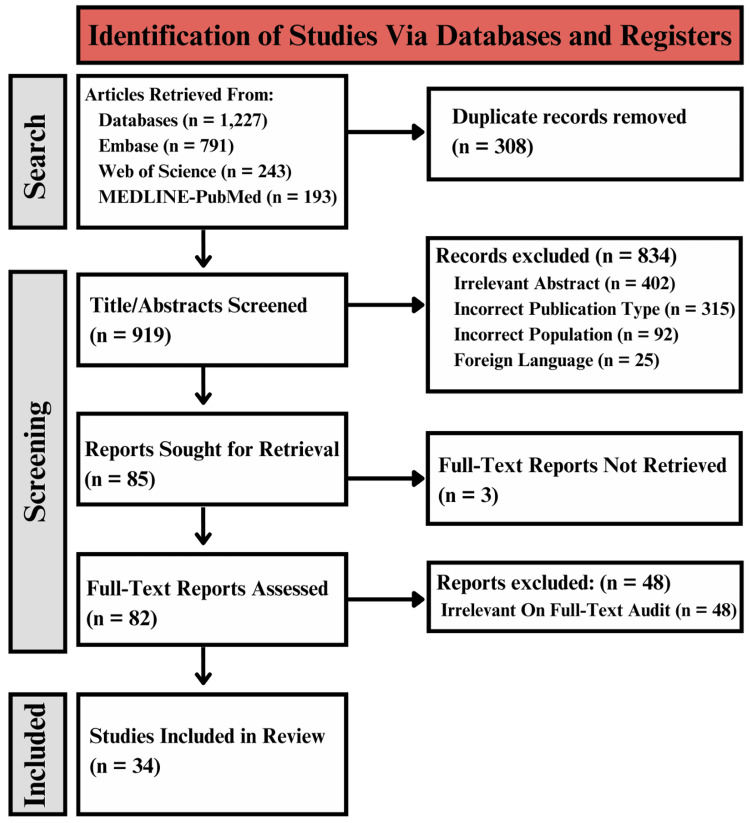 Figure 1
Figure 1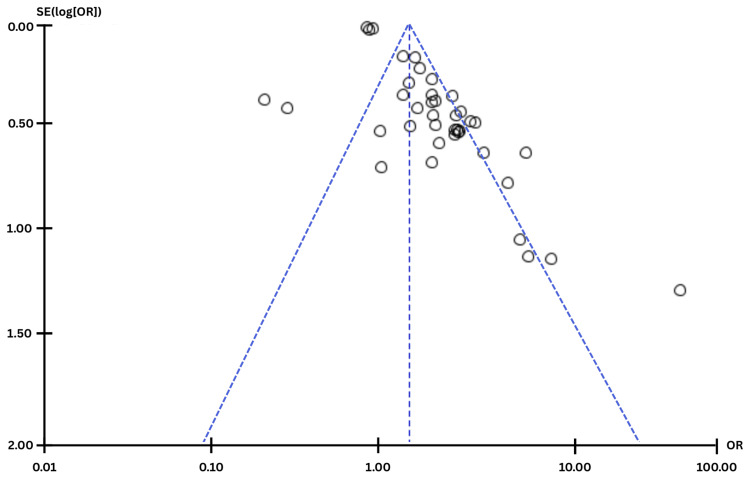 Figure 2
Figure 2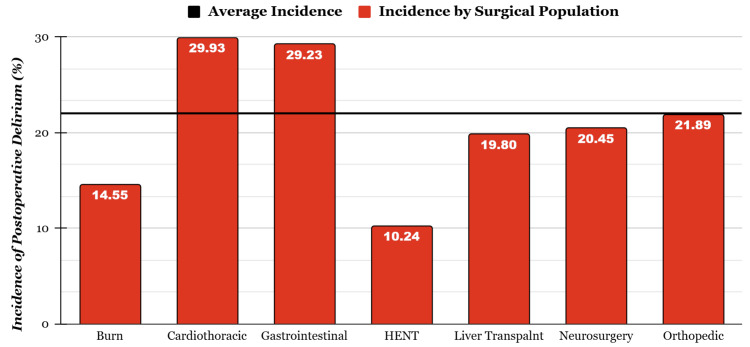 Figure 3
Figure 3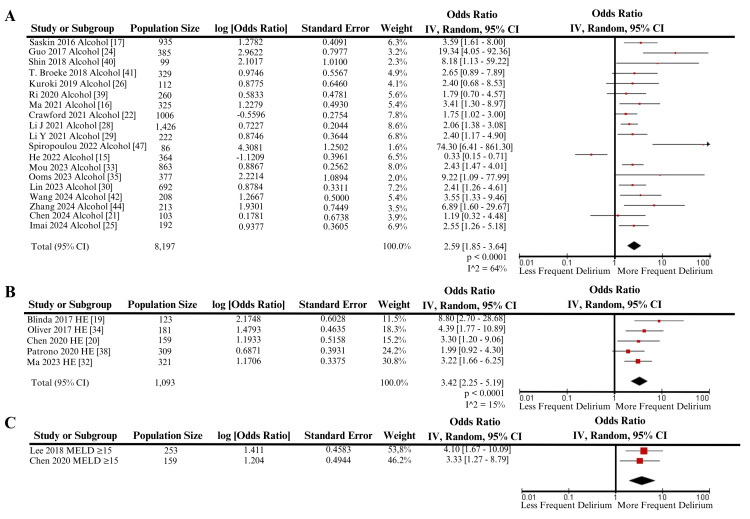 Figure 4
Figure 4| Study | Population size | Delirium screening scale | Avg. SE | Indirectness | Other limitations | Quality of evidence |
| Densky et al., 2019 [ | 515 | DSM-IV | 0.3537 | N/A | N/A | High |
| He and Fang, 2022 [ | 364 | CAM-ICU | 0.3961 | N/A | N/A | High |
| Ma et al., 2021 [ | 325 | CAM | 0.4930 | N/A | N/A | High |
| Şaşkın et al., 2016 [ | 935 | CAM-ICU | 0.4091 | N/A | N/A | High |
| Bhattacharya et al., 2017 [ | 144 | DOSS | 0.0159 | NOR | LT population | Moderate |
| Blinda et al., 2017 [ | 123 | CAM-ICU | 0.6028 | N/A | LT population | Moderate |
| Chen et al., 2020 [ | 159 | CAM-ICU | 0.5158 | N/A | LT population | Moderate |
| Chen et al., 2024 [ | 103 | CAM | 0.6738 | NOR | N/A | Moderate |
| Crawford et al., 2021 [ | 1006 | EMR mention of delirium | 0.2754 | N/A | N/A | Moderate |
| Guo et al., 2016 [ | 572 | CAM | 0.0198 | N/A | Age >65 years | Moderate |
| Guo et al., 2017 [ | 385 | CAM | 0.7977 | N/A | Burn Population | Moderate |
| Imai et al., 2024 [ | 192 | CAM | 0.9377 | N/A | N/A | Moderate |
| Kuroki et al., 2019 [ | 112 | DSM-IV | 0.6460 | N/A | N/A | Moderate |
| Lee et al., 2018 [ | 253 | CAM-ICU | 0.4583 | N/A | LT population | Moderate |
| Li J. et al., 2021 [ | 1,426 | CAM-ICU | 0.2044 | N/A | Age >65 years | Moderate |
| Li Y. et al., 2021 [ | 222 | CAM | 0.3644 | NOR | Age >65 years | Moderate |
| Lin et al., 2023 [ | 692 | CAM-ICU | 0.3311 | NOR | N/A | Moderate |
| Lu et al., 2022 [ | 402 | CAM-ICU | 0.4295 | N/A | LT population | Moderate |
| Ma et al., 2023 [ | 321 | CAM-ICU | 0.3375 | N/A | LT population | Moderate |
| Mou et al., 2023 [ | 863 | DSM-V | 0.2562 | N/A | Age >65 years | Moderate |
| Oliver et al., 2017 [ | 181 | EMR mention of delirium | 0.4635 | N/A | LT population | Moderate |
| Ooms et al., 2023 [ | 377 | CAM-ICU | 1.0894 | N/A | N/A | Moderate |
| Park et al., 2017 [ | 196 | DSM-V | 0.5026 | N/A | N/A | Moderate |
| Park et al., 2020 [ | 325 | DSM-IV/ CAM | 0.3322 | N/A | LT population | Moderate |
| Patrono et al., 2020 [ | 309 | CAM | 0.3931 | N/A | LT population | Moderate |
| Ri et a.l, 2020 [ | 260 | DSM-IV | 0.4781 | NOR | LT population | Moderate |
| Shin et al., 2018 [ | 99 | CAM-ICU | 1.0100 | N/A | N/A | Moderate |
| Broeke et al., 2018 [ | 329 | DOSS | 0.5567 | N/A | N/A | Moderate |
| Wang et al., 2024 [ | 208 | CAM-ICU | 0.5000 | N/A | Age >65 years | Moderate |
| Wu et al., 2021 [ | 228 | CAM-ICU | 0.4715 | NOR | N/A | Moderate |
| Zhang et al., 2024 [ | 213 | DSM-V | 0.7449 | N/A | N/A | Moderate |
| Cao et al., 2024 [ | 80 | CAM | 1.1034 | NOR | N/A | Low |
| Chang et al., 2022 [ | 84 | CAM-ICU | 0.6030 | N/A | LT population | Low |
| Spiropoulou et al., 2022 [ | 86 | CAM-ICU | 1.2502 | N/A | Age >65 years | Low |
| Study | Study design | Surgical population | Population size | Incidence of POD (%) | Variable assessed | OR | 95% CI | P-value |
| Park et al., 2017 [ | Retrospective observational cohort study | GI | 196 | 0.224 | Anti-HCV antibody-positive | 1.181 | 0.441 - 3.164 | 0.7406 |
| Park et al., 2020 [ | Retrospective observational cohort study | LT | 325 | 0.212 | Alcoholic liver disease | 1.63 | 0.850 - 3.127 | 0.141 |
| Chen et al., 2024 [ | Prospective randomized and double-blinded controlled trial | GI | 103 | 0.184 | History of alcohol use | 1.195 | 0.319 - 4.476 | 0.791 |
| Crawford et al., 2021 [ | Retrospective observational cohort study | HENT | 1006 | 0.075 | History of alcohol use | 1.75 | 1.02 - 23.0 | 0.0422 |
| Guo et al., 2017 [ | Retrospective observational cohort study | Burn | 385 | 0.145 | History of alcohol use | 19.34 | 4.05 - 92.25 | 0.0002 |
| He and Fang, 2022 [ | Retrospective observational cohort study | CT | 364 | 0.255 | History of alcohol use | 0.326 | 0.15 - 0.71 | 0.706 |
| Imai et al., 2024 [ | Retrospective observational cohort study | HENT | 192 | 0.224 | History of alcohol use | 2.554 | 1.260 - 5.268 | 0.0098 |
| Kuroki et al., 2019 [ | Retrospective observational cohort study | GI | 112 | 0.277 | History of alcohol use | 2.405 | 0.678 - 8.534 | 0.175 |
| Li J. et al., 2021 [ | Retrospective observational cohort study | CT | 1,426 | 0.393 | History of alcohol use | 2.06 | 1.38 - 3.10 | <0.001 |
| Li Y. et al., 2021 [ | Prospective observational cohort study | GI | 222 | 0.41 | History of alcohol use | 2.398 | 1.174 - 4.900 | 0.016 |
| Ma et al., 2021 [ | Retrospective observational cohort study | Orthopedic | 325 | 0.178 | History of alcohol use | 3.414 | 1.299 - 8.975 | 0.013 |
| Mou et al., 2023 [ | Retrospective observational cohort study | Neurosurgery | 863 | 0.1 | History of alcohol use | 2.427 | 1.469 - 3.384 | 0.011 |
| Ooms et al., 2023 [ | Retrospective observational cohort study | HENT | 377 | 0.106 | History of alcohol use | 9.22 | 1.09 - 77.97 | 0.041 |
| Saskin et al., 2016 [ | Retrospective observational cohort study | CT | 935 | 0.225 | History of alcohol use | 3.59 | 1.61 - 7.98 | 0.002 |
| Shin et al., 2018 [ | Retrospective observational cohort study | Orthopedic | 99 | 0.404 | History of alcohol use | 8.18 | 1.13 - 16.60 | 0.0374 |
| Spiroopoulou et al., 2022 [ | Retrospective observational cohort study | CT | 86 | 0.256 | History of alcohol use | 74.3 | 6.41 - 861 | 0.0006 |
| Broeke et al., 2018 [ | Prospective observational cohort study | CT | 329 | 0.128 | History of alcohol use | 2.65 | 0.89 - 7.90 | 0.08 |
| Wang et al., 2024 [ | Retrospective observational cohort study | Neurosurgery | 208 | 0.524 | History of alcohol use | 3.549 | 1.332 - 9.459 | 0.0113 |
| Zhang et al., 2024 [ | Retrospective observational cohort study | Neurosurgery | 213 | 0.296 | History of alcohol use | 6.89 | 1.60 - 29.68 | 0.01 |
| Lin et al., 2023 [ | Retrospective observational cohort study | CT | 692 | 0.318 | History of alcohol use | 2.407 | 1.258 - 3.608 | 0.008 |
| Total bilirubin elevated | 1.907 | 1.402 - 2.513 | 0.0001 | |||||
| Serum IL-6 | 1.616 | 1.210 - 2.022 | 0.0011 | |||||
| Blinda et al., 2017 [ | Retrospective observational cohort study | LT | 123 | 0.122 | History of hepatic encephalopathy | 8.8 | 2.7 - 28.59 | 0.0003 |
| Chen et al., 2020 [ | Retrospective observational cohort study | LT | 159 | 0.264 | History of hepatic encephalopathy | 3.298 | 1.200 - 9.065 | 0.021 |
| MELD ≥15 | 3.334 | 1.265 - 8.786 | 0.015 | |||||
| Preoperative ammonia >46 umol/L | 3.513 | 1.306 - 9.455 | 0.013 | |||||
| Oliver et al., 2017 [ | Retrospective observational cohort study | LT | 181 | 0.21 | History of hepatic encephalopathy | 4.39 | 1.77 - 10.9 | 0.0014 |
| Patrono et al., 2020 [ | Retrospective observational cohort study | LT | 309 | 0.133 | History of hepatic encephalopathy | 1.988 | 0.920 - 4.296 | 0.8 |
| Cao et al., 2024 [ | Retrospective observational cohort study | Neurosurgery | 80 | 0.263 | IL-6 | 12.659 | 1.456 - 110.082 | 0.021 |
| Bhattacharya et al., 2017 [ | Retrospective observational cohort study | LT | 144 | 0.25 | MELD | 0.98 | 0.95 - 0.99 | 0.2028 |
| Lee et al., 2018 [ | Retrospective observational cohort study | LT | 253 | 0.17 | MELD ≥15 | 4.1 | 1.67 - 10.09 | 0.002 |
| Ma et al., 2023 [ | Retrospective observational cohort study | LT | 321 | 0.193 | MELD >22 | 3.4 | 1.468 - 7.876 | 0.004 |
| History of hepatic encephalopathy | 3.224 | 1.664 - 6.244 | 0.001 | |||||
| Ri et al., 2020 [ | Retrospective observational cohort study | LT | 260 | 0.142 | MELD | 1.02 | 0.967 - 1.076 | 0.458 |
| History of alcohol use | 1.792 | 0.702 - 4.573 | 0.222 | |||||
| Chang et al., 2022 [ | Retrospective observational cohort study | LT | 84 | 0.548 | Preop alcohol abstinence <3 months | 4.953 | 1.519 - 16.152 | 0.008 |
| Densky et al., 2019 [ | Retrospective observational cohort study | HENT | 515 | 0.109 | Preop alcohol abstinence <3 months | 0.24 | 0.12 - 0.51 | 0.0001 |
| Guo et al., 2016 [ | Prospective observational cohort study | Orthopedic | 572 | 0.21 | Total bilirubin >14 umol/L | 1.077 | 1.036 - 1.121 | 0.002 |
| Lu et al., 2022 [ | Retrospective observational cohort study | LT | 402 | 0.194 | Total bilirubin >3.3 mg/dL | 2.46 | 1.06 - 5.69 | 0.035 |
| Wu et al., 2021 [ | Prospective observational cohort study | Non-CT | 228 | 0.25 | Total or direct bilirubin elevated | 2.535 | 1.006 - 6.388 | 0.0485 |
| Outcome assessed | Pooled adjusted OR | 95% CI | P-value | I2 |
| History of alcohol use | 2.59 | 1.85 - 3.64 | <0.0001 | 64% |
| History of hepatic encephalopathy | 3.42 | 2.25 - 5.19 | <0.0001 | 15% |
| Elevated serum IL-6 | 3.38 | 0.49 - 23.43 | 0.22 | 71% |
| MELD score ≥15 | 3.73 | 1.93 - 7.20 | <0.0001 | 0% |
| Elevated total bilirubin | 1.57 | 0.94 - 2.63 | 0.09 | 88% |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntensive Care Unit Cognitive Disorders · Anesthesia and Neurotoxicity Research · Anesthesia and Sedative Agents
Introduction and background
The global incidence of hepatic-related deaths has been continually on the rise: from 110.6 per 100,000 in 1990 to 132.5 per 100,000 in 2017 [1]. There is a growing population of patients living with some form of hepatic disease and awaiting a liver transplant. In 2021, there was a 6.5% increase compared to the previous year in the number of liver transplants performed globally [1]. There are several indications for patients to receive a liver transplant, including viral hepatitis, non-alcoholic fatty liver disease, hepatocellular carcinoma, and alcoholic hepatitis; with many of these disease processes increasing in incidence [2,3]. Furthermore, patients with any form of liver disease often have comorbidities or complications that may require surgical intervention in addition to requiring a liver transplant. With the increased need for surgery among hepatically impaired patients, postoperative delirium (POD) is a common complication to be aware of.
The risk for POD is further heightened in patients with pre-existing health conditions compared to a healthier population. Diabetes and cardiovascular conditions have been well-established risk factors for POD [4]. The increased surgical risk and care complexities contribute to higher healthcare costs, as well as increase morbidity and negative outcomes among liver disease patients. Despite the growing prevalence of liver disease patients, there is limited research on methods to screen for the risk of POD. Alcohol abuse is a well-documented risk factor for POD [4]. However, there are limited studies on hepatic pathologies as a risk factor. There are multiple biomarkers used to indicate the presence and potential severity of hepatic impairment. In addition to biomarkers, Child-Pugh scores and MELD (Model for End-Stage Liver Disease) are widely used metrics, which combine a variety of factors, such as total bilirubin, serum albumin, international normalized ratio, and serum creatinine, among others, to evaluate patients with cirrhosis [2].
A significant history of alcohol consumption has been previously implicated in the development of POD, among other surgical complications [5]. It is widely known to stem from a multifactorial etiology, and that alcohol can affect several organs, not just the liver. It is hypothesized that the association between alcohol consumption and POD stems from alcohol's disruption of acetylcholine and dopamine levels [6,7]. Alcohol has been linked to an elevation of dopamine levels, which has subsequently been linked to POD [8]. Also, alcohol has been implicated in increased acetylcholine levels [9]. Additionally, several pharmacological agents utilized during general anesthesia undergo major hepatic elimination pathways. Inhibition of these pathways could theoretically lead to overaccumulation of metabolites, especially opioid metabolites that can cross the blood-brain barrier [10]. Alcohol consumption in severe cases can also result in delirium as a function of thiamine depletion and Wernicke encephalopathy [11]. Lastly, a withdrawal from alcohol can precipitate delirium and delirium tremens, as patients are likely to deviate from their normal alcohol consumption leading up to surgery [12].
The objective of this systematic review and meta-analysis was to identify the role that specific indicators of preoperative hepatic impairment contribute to increased risk for POD. We aimed to identify the incidence rate of POD in different surgical populations. To the knowledge of the authors of this review, there are no similar reviews in the literature that address this research topic.
Review
Materials and methods
Review Registration
The review was registered in PROSPERO under the identification number CRD42024627855..
Database Search and Screening
Embase, Web of Science, and OVID-MEDLINE databases were searched for relevant keywords including: aspartate aminotransferase (AST), alanine aminotransferase (ALT), alkaline phosphatase (ALP), gamma-glutamyl transferase (GGT), alpha-fetoprotein (AFP), ceruloplasmin, nucleotidase (NTP), bilirubin, cirrhosis, alcohol, alcoholic, hepatitis, hepatocellular carcinoma (HCC), hemochromatosis and the resulting incidence of POD. Studies isolated from the databases were subjected to a standardized screening process in Rayyan that required the fulfillment of the following metrics: 1. English language, 2. randomized controlled trial, retrospective observational, prospective observational, or case-control study designs, 3. adult, human population, 4. full-text availability, and 5. reporting of a multivariate odds ratio (OR) for the association of aforementioned metrics of hepatic impairment and the incidence of POD (Figure 1) [13]. This search was carried out entirely on December 15th, 2024.
The PRISMA diagram depicting the selection of studiesPRISMA: The Preferred Reporting Items for Systematic Reviews and Meta-Analyses
Quality Assessment of Included Studies
All studies included in this review underwent a standardized quality assessment consisting of five independent metrics: the tool used to screen for delirium, at least 100 patient population size, OR standard error less than or equal to 0.5, presence of indirectness, and any evidence of other limitations (Table 1). If a study met all of these criteria, then it was considered of “high” quality for this review. If a study only met four or three of these criteria, then it was considered of “moderate” quality for this review. Lastly, if a study met less than three of these criteria, it was considered of “low” quality for this review.
Meta-Analysis
Multivariate ORs were isolated from the included studies. Inverse variance meta-analysis was performed within ReviewManager 5.4.1. Adjusted ORs were pooled for associations with POD under a random effects model based on a 95% confidence interval (CI). Two-sided p-values less than 0.05 were considered statistically significant. Pooled adjusted ORs for associations between indicators of preoperative hepatic impairment and POD were tabulated.
Publication Bias Assessment
Publication bias was evaluated visually using a funnel plot generated in Review Manager (RevMan) version 5.4. For the generic inverse variance meta-analysis, study-specific effect estimates and their standard errors were plotted on the horizontal and vertical axes, respectively. A pooled effect estimate was calculated using inverse-variance weighting, and a triangular 95% confidence region was overlaid. Symmetry of the plot was assessed qualitatively to identify potential small-study effects or missing studies. Egger’s regression test was performed by regressing the standard normal deviate of each study’s effect estimate against its precision (1/SE). A significant non-zero intercept was interpreted as evidence of small-study effects.
Funnel plot assessing for publication biasThis figure depicts the funnel plot generated from the summary statistic used to assess for publication bias. Egger's test intercept for the summary statistic dataset was 1.92 with a p-value of 0.79, indicating a low risk for publication bias in the meta-analysisSE: standard error; OR: odds ratio
Results
Summary of Results
A total of 12,089 patients were included in this review, of which 2,663 developed POD, indicating an overall incidence of 22.03%. In total, nine different indicators of preoperative hepatic impairment were included in the review, namely: presence of anti-HCV antibodies, history of alcoholic liver disease, history of alcohol use, history of hepatic encephalopathy, elevated total bilirubin >3.3 mg/dL, elevated serum IL-6, elevated MELD score, elevated preoperative ammonia >46 umol/L, and alcohol abstinence within three months of undergoing general anesthesia (Table 2).
POD in Different Surgical Populations
Across the 34 included studies, seven different surgical populations were included: liver transplantation, gastrointestinal (other than liver transplantation), cardiothoracic, head-ears-nose-throat, orthopedic, neurosurgery, and burn populations. The incidence of delirium was the highest in the cardiothoracic population at 29.93% and the lowest in the head, ears, nose, throat (HENT) population at 10.24% (Figure 3).
Incidence of POD in different surgical populationsThis figure includes the incidence of POD by the surgical population weighted by population size. Burn - [24]; cardiothoracic - [15,17,28,30,41,47]; gastrointestinal - [21,26,29,36]; HENT- [14,22,25,35]; liver transplant - [18,19,20,27,31,32,34,37,38,39,46]; neurosurgery - [33,42,44,45]; orthopedic - [16,23,40]POD: postoperative delirium; HENT: head, ears, nose, throat
Meta-Analysis Results
Figure 4 is a forest plot that displays the significant outcomes resulting from inverse variance meta-analysis. Three hepatic variables met statistical significance: history of alcohol use (OR: 2.59, 1.85 - 3.64, p<0.0001), history of hepatic encephalopathy (OR: 3.42, 2.25 - 5.19, p<0.0001) (Table 3), and MELD ≥15 (OR: 3.73, 1.93 - 7.20, p<0.0001). Two other variables were analyzed by meta-analysis but did not find significance: elevated serum IL-6 (OR: 3.38, 0.49 - 23.43, p=0.22), and elevated total bilirubin (OR: 1.57, 0.94 - 2.63, p=0.09) (Table 3).
Forest plots of meta-analysis examining the association between alcohol use (A), hepatic encephalopathy (B), and MELD ≥15 with postoperative delirium riskThis figure depicts the forest plots for significant meta-analyses. Panel A: forest plot examining the association between alcohol use and postoperative delirium. Panel B: forest plot examining the association between HE (hepatic encephalopathy) and postoperative delirium. Panel C: forest plot examining the association between MELD ≥15 and postoperative deliriumIV: inverse variance; MELD: Model for End-Stage Liver Disease; CI: confidence interval
Discussion
The goal of this systematic review and meta-analysis was to identify the role that specific indicators of preoperative hepatic impairment contribute to increased risk for POD. We aimed to identify the incidence rate of POD in different surgical populations. To the knowledge of the authors of this review, there are no similar reviews in the literature that address this research question. The final results of our study reveal that known indicators of hepatic impairment in a patient’s past medical history, namely alcohol use and previous diagnosis of hepatic encephalopathy, are significant factors for POD (Table 3). Also, a MELD score ≥15 was found to be a risk factor. Specifically, patients with a history of alcohol use were 2.59 times more likely to develop POD, whereas a history of hepatic encephalopathy carried a 3.42 times increased risk (Table 3), and a MELD score ≥15 carried a 3.73 times increased risk.
A history of hepatic encephalopathy is a logical risk factor for POD, as the most significant risk factor for POD in general is preoperative cognitive dysfunction [48]. While hepatic encephalopathy can present with varying symptoms, the most common are confusion, forgetfulness, and slurred speech, all of which coincide with delirium [49]. The symptoms of hepatic encephalopathy are largely attributed to elevated ammonia levels [50, 51]. Only one study reported a multivariate odds ratio for preoperative ammonia level > 46 umol/L, which found significance and reported an odds ratio of 3.513 (CI 1.306 - 9.455) for association with POD [20]. Overall, alcohol and hepatic encephalopathy are significant risk factors for POD, and care should be taken to mitigate other factors that may put these predisposed patients at further risk.
There are a few limitations to this study that should be addressed. First, our systematic review was specific in its inclusion criteria. Specifically, we required multivariate odds ratios with corresponding 95% confidence intervals and p-values for inclusion. Our goal was to synthesize a focused review, which may have led to some tangentially beneficial studies being excluded. The quality assessment cut-off values for the average standard error and population size, although consistent, are rigidly selected. They did not differentiate studies that were very close to satisfying the requirement from those that were not. One of the more common etiologies of POD is active infection, which was not controlled for in this review.
Furthermore, some studies were nonspecific in the reporting of their outcomes, as outlined in Table 1. This is especially true for the studies that reported a history of alcohol use, as this is an extremely difficult metric to standardize. This likely contributed to substantial heterogeneity between meta-analyzed studies when pooling nonspecific outcomes. Lastly, an elevated MELD score ≥15 was found to be a significant risk factor; however, only two studies were included that utilized this stringent cut-off. Further research should be conducted to analyze the role MELD scoring may play in POD prediction. Confounding effects were minimized by requiring multivariate odds ratios and utilizing an inverse variance meta-analysis.
Conclusions
Based on the results of this study, it is evident that individuals with a known medical history of hepatic pathology are at increased risk of developing POD. Namely, alcohol consumption and history of hepatic encephalopathy were both found to be statistically significant contributors to POD. However, specific biomarkers (elevated bilirubin and serum IL-6) linked to hepatic function did not show significance in our study. Likewise, an elevated MELD score did not meet statistical significance in contributing to POD. While specific hepatic biomarkers were not necessarily implicated in POD, further research in quantifying the effects of lifestyle factors (consumption of alcohol) and history of gross liver impairment (hepatic encephalopathy) is warranted to better understand how overall liver function affects postoperative outcomes when general anesthesia is required.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Liver transplantation 2023: status report, current and future challenges Clin Gastroenterol Hepatol Terrault NA Francoz C Berenguer M Charlton M Heimbach J 215021662120233708492810.1016/j.cgh.2023.04.005 · doi ↗ · pubmed ↗
- 2Liver Transplantation Dababneh Y Mousa OY Treasure Island, FL Stat Pearls Publishing 2025 https://www.ncbi.nlm.nih.gov/books/NBK 559161/32644587 · pubmed ↗
- 3Trends in liver disease etiology among adults awaiting liver transplantation in the United States, 2014-2019 JAMA Netw Open Wong RJ Singal AK 03202010.1001/jamanetworkopen.2019.20294 PMC 1212473232022875 · doi ↗ · pubmed ↗
- 4Postoperative Delirium Janjua MS Spurling BC Arthur ME Treasure Island, FL Stat Pearls Publishing 2025 https://www.ncbi.nlm.nih.gov/books/NBK 534831/30521252 · pubmed ↗
- 5Alcohol-related predictors of delirium after major head and neck cancer surgery Arch Otolaryngol Head Neck Surg Shah S Weed HG He X Agrawal A Ozer E Schuller DE 26627113820122243187110.1001/archoto.2011.1456 · doi ↗ · pubmed ↗
- 6Long-term alcohol consumption alters dorsal striatal dopamine release and regulation by D 2 dopamine receptors in rhesus macaques Neuropsychopharmacology Salinas AG Mateo Y Carlson VC 143214414620213345243010.1038/s 41386-020-00938-8PMC 8209056 · doi ↗ · pubmed ↗
- 7Voluntary ethanol intake increases extracellular acetylcholine levels in the ventral tegmental area in the rat Alcohol Alcohol Larsson A Edström L Svensson L Söderpalm B Engel JA 3493584020051604343610.1093/alcalc/agh 180 · doi ↗ · pubmed ↗
- 8Alcohol and dopamine Alcohol Health Res World Di Chiara G 108114211997 https://pubmed.ncbi.nlm.nih.gov/15704345/15704345 PMC 6826820 · pubmed ↗