Sandwich Reconstruction Technique for Severe Glenoid Bone Loss in Reverse Shoulder Arthroplasty Using Iliac Crest Autograft and Coracoid Transfer
Vasileios Akrivos, Gabriel Levy, Jeanni Zbinden, Philippe Collin, Alexandre Lädermann

TL;DR
This paper introduces a new surgical technique for shoulder replacement in patients with severe bone loss, using two types of grafts to improve implant stability.
Contribution
The novel 'sandwich' technique combines iliac crest and vascularized coracoid grafts with a wedge-augmented baseplate for enhanced stability in severe glenoid bone loss.
Findings
The sandwich grafting technique restores native glenoid anatomy and improves implant stability.
The method is suitable for severe glenoid bone loss classified as Walch B3, C, and D.
Dual-graft approach overcomes limitations of single-graft techniques and augmented baseplates.
Abstract
This Technical Note describes a sandwich grafting technique that combines a posterior tricortical iliac crest autograft with an anterior vascularized coracoid graft, secured with a full wedge-augmented baseplate. The method enhances fixation by leveraging the mechanical stability of the iliac crest graft, the biological integration of the vascularized coracoid, and the stability provided by the wedge-augmented baseplate. The screws are positioned in 2 axes to optimize stability and promote graft incorporation. This dual-graft approach addresses the limitations of single-graft techniques and augmented baseplates by restoring native glenoid anatomy and improving implant stability. The technique is particularly suited for cases with severe anterior-posterior or global glenoid bone loss, as classified by the Walch B3, C, and D categories.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1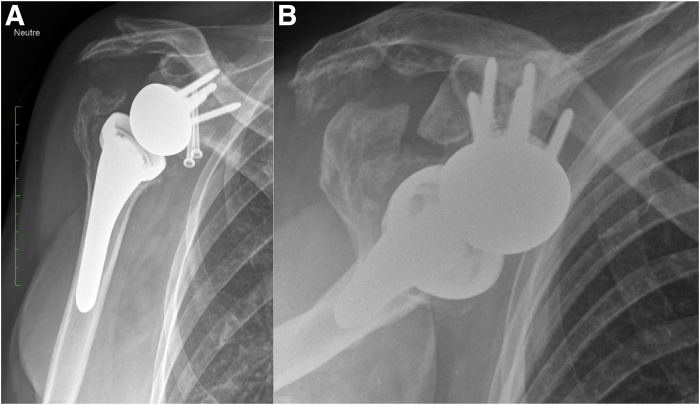 Figure 2
Figure 2 Figure 3
Figure 3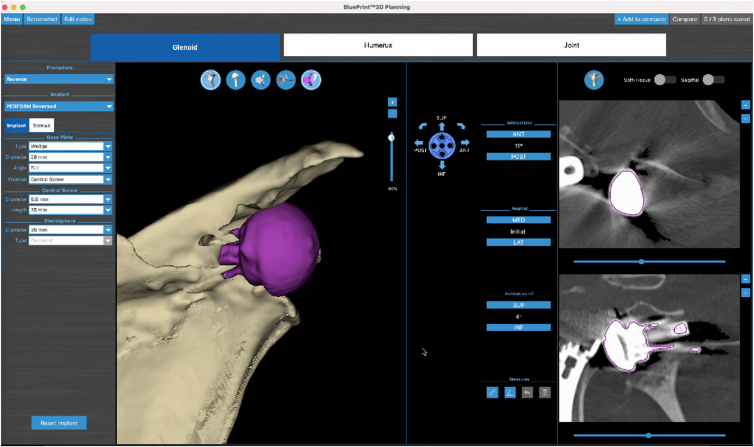 Figure 4
Figure 4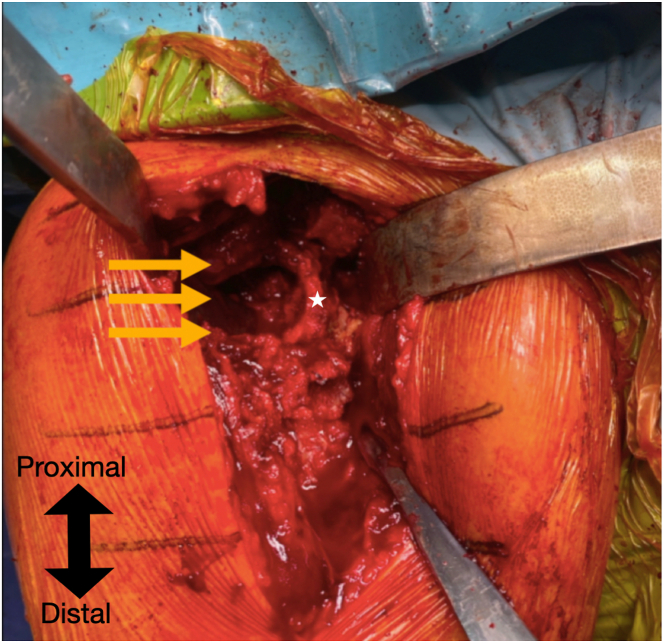 Figure 5
Figure 5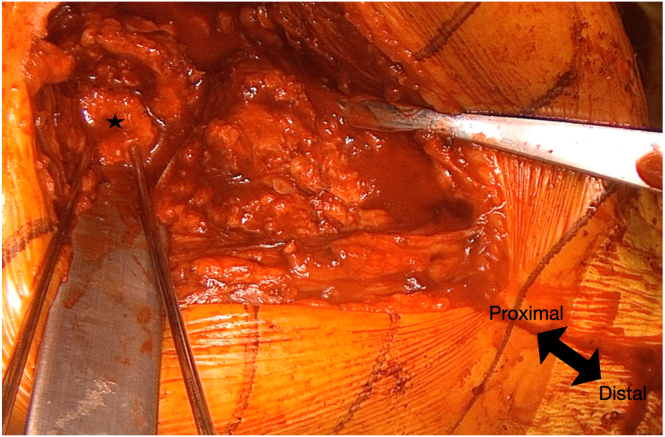 Figure 6
Figure 6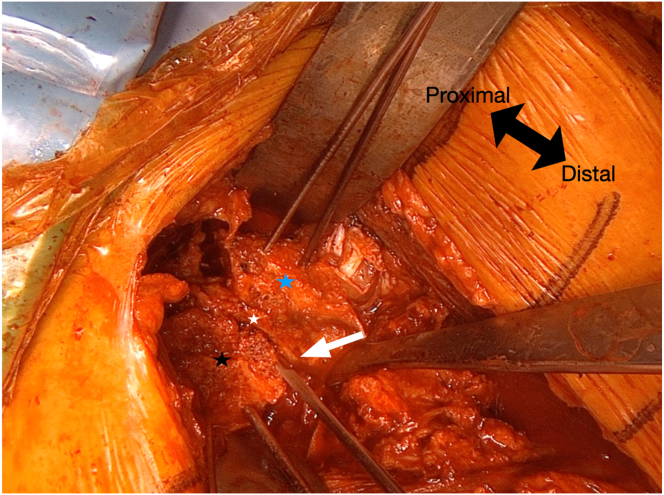 Figure 7
Figure 7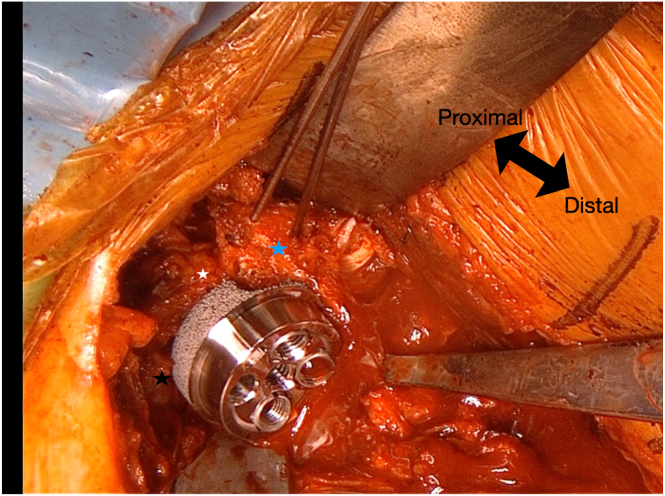 Figure 8
Figure 8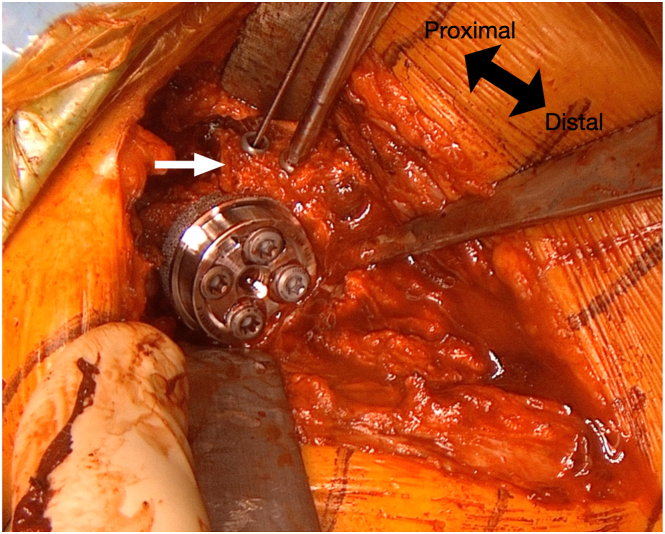 Figure 9
Figure 9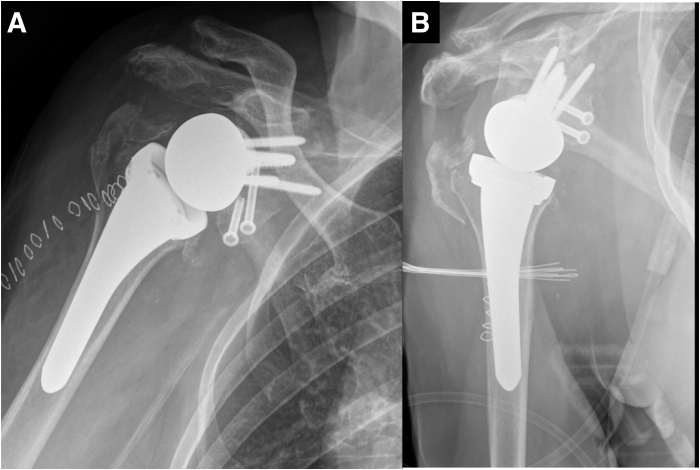 Figure 10
Figure 10Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsShoulder Injury and Treatment · Shoulder and Clavicle Injuries · Trauma Management and Diagnosis
The number of cases with glenoid bone loss is expected to increase in the future as a result of the increasing prevalence of prosthetic implants, longer life expectancy, and the greater functional demands of patients.1^,^2 Aseptic glenoid baseplate loosening occurs in 2.69% of cases involving osteoarthritis with bone loss, with an increased incidence of 6.8% in revision procedures involving baseplate failure. The standard baseplates may be insufficient for achieving optimal fixation in the presence of compromised bone stock, potentially leading to instability, early loosening, and implant failure.3, 4, 5, 6
Structural bone grafting during reverse shoulder arthroplasty (RSA) typically is considered when native bone coverage of the baseplate is less than 50%.7 Although various grafting techniques—including humeral head autografts in primary cases, tricortical iliac crest grafts, and allografts—have been proposed for glenoid bone loss, each presents limitations such as graft availability, morbidity, or insufficient mechanical integrity.8 In revision cases and primary cases with massive uncontained bone loss, humeral head autograft is either unavailable or insufficient, necessitating alternatives such as an iliac crest autograft or various allografts. However, iliac crest bone graft harvest is associated with a 15% donor-site morbidity rate, whereas allografts demonstrate low incorporation rates and high complication rates.9, 10, 11
An alternative approach for surgeons is the use of augmented components and patient-specific implants. The use of custom 3-dimensional−printed implants for managing severe glenoid bone loss in both primary and revision RSA has demonstrated significant clinical improvements in this complex patient population. However, these options are associated with greater costs.12 This Technical Note describes a composite "sandwich" grafting technique that combines an iliac crest autograft posteriorly with a pediculated coracoid graft anteriorly, along with a full wedge-augmented baseplate.
Surgical Technique
Preoperative Planning
Radiographic imaging (Fig 1) revealed loosening of the glenoid baseplate, glenoid dislocation, and possible glenoid fracture. Computed tomography revealed the presence of a severe posterior glenoid defect and a smaller one in the anterior wall (Fig 2). Comprehensive preoperative imaging was essential for accurate assessment and surgical planning. Three-dimensional computed tomography with virtual planning software aided in evaluating glenoid morphology and classifying bone defects (Fig 3). Table 1 describes the indications and contraindications for the sandwich technique in glenoid reconstruction.Fig 1. An anteroposterior radiograph of the right shoulder demonstrating loosening of the glenoid baseplate, glenoid dislocation, and possible glenoid fracture.Fig 2. Three-dimensional model of the scapula illustrating the glenoid defect.Fig 3. Essential preoperative 3-dimensional planning for management of severe glenoid bone loss.Table 1. Indications and Contraindications for the Sandwich Technique in Glenoid ReconstructionIndicationsContraindicationsSevere anteroposterior glenoid bone lossPrevious Latarjet or Bristow procedureGlobal bone loss requiring robust fixationInsufficient iliac crest or coracoid sizePoor native glenoid bone qualityAdvanced infection or osteomyelitis
Surgical Approach and Glenoid Exposure
A deltopectoral approach is used upon reopening of the previous incision. The previous wound is removed with this standard incision beginning at the tip of the coracoid process extending distally. Aerobic and anaerobic samples are taken for microbiological analysis. The cephalic vein is preserved and retracted laterally. The subscapularis tendon, if still intact, is released via tenotomy to allow adequate glenoid exposure. A circumferential capsular release is carefully performed in order to protect the axillary nerve inferiorly. The anterior and posterior walls of the glenoid are meticulously cleaned to ensure complete visualization of the defects without soft tissue interference.
To optimize glenoid exposure, the humeral metaphysis and stem are removed, and the dislocated glenosphere and baseplate are extracted, revealing complete destruction of the glenoid (Fig 4). The primary finding in the glenoid is a posterior defect extending from the 12-o’clock to the 6-o’clock position, measuring approximately 25 mm in length and 7 mm in width (Video 1). The anterior defect is smaller, extending from the 3-o’clock to the 6-o’clock position, with dimensions of 9 mm in length and 4 mm in width. The proximal-to-distal length of the posterior defect is measured to determine the required dimensions of the iliac crest graft.Fig 4. After removal of the previous implants, a severe posterior glenoid defect is observed (yellow arrows). The anterior glenoid wall remnant is indicated by the white star.
Graft Harvesting
Iliac Crest Graft
A tricortical iliac crest graft of appropriate dimensions is harvested through a separate incision over the anterolateral iliac crest. The graft is meticulously shaped to fit the posterior glenoid defect and compensated with the glenoid anatomy, ensuring a flat surface for graft-to-bone contact. The cortical surface provides structural integrity, while the cancellous portion enhances integration.
Coracoid Graft
A coracoid osteotomy is performed at its base using a curved osteotome (Video 1). Soft-tissue attachments, including the conjoined tendon, are preserved to maintain vascularity. The graft is then rotated 90°, contoured to fit the anterior glenoid defect.
Sandwich Grafting Technique
The sandwich grafting technique involves impacting the tricortical iliac crest graft with gentle pressure and stabilizing it in the posterior glenoid, initially securing it with 2 K-wires to create a flat, smooth surface (Video 1, Fig 5). The native glenoid remnant serves as the central layer of the construct. Anteriorly, the coracoid graft is fixed in the anterior defect below the glenoid equator with 2 K-wires, ensuring proper alignment with the native glenoid curvature.13 These 2 K-wires simultaneously stabilize the tricortical crest autograft as they are directed toward the tricortical iliac crest.Fig 5. The graft is stabilized using 2 K-wires, one positioned superiorly and one inferiorly. The tricortical iliac crest autograft is indicated by the black star.
Using the baseplate K-wire guide, a K-wire is placed inferiorly, flush with the inferior border of the glenoid (Fig 6). In the anteroposterior axis, half of the baseplate is positioned over the tricortical autograft, while the other half is placed over the glenoid remnant and coracoid graft (Fig 7). This technique allows for secure fixation of the posterior graft with 2 screws. The central peg hole is then drilled into the glenoid remnant, and a 15° full-wedge augmented baseplate (Perform Reverse; Stryker, Bloomington, MN) with a central screw is positioned at the glenoid.Fig 6. The glenoid baseplate guide (white arrow) is positioned at the central and inferior aspect of the glenoid. The coracoid process (blue star), anterior glenoid wall remnant (white star), and the tricortical iliac crest autograft (black star) are clearly visualized, comprising the key components of the "sandwich technique" construct.Fig 7. In the anteroposterior axis, half of the baseplate is positioned over the tricortical autograft, while the other half rests on the glenoid remnant and coracoid graft. This configuration enables secure fixation of the posterior graft with two screws. The central peg hole is drilled into the glenoid remnant, and a 15° full-wedge augmented baseplate with a central screw is positioned at the glenoid. The coracoid process (blue star), anterior glenoid wall remnant (white star), and tricortical iliac crest autograft (black star) are indicated.
The first inserted screw is the superior cortical screw, which compresses the baseplate against the glenoid. The remaining 3 screws are locking screws, with the posterior and inferior screws further stabilizing the tricortical autograft. Next, two 4.5-mm partial-threaded anterior screws are inserted to stabilize the coracoid (Fig 8). Both screws are also directed to engage the posterior tricortical iliac crest autograft for additional support. Afterward, the 2 K-wires stabilizing the iliac crest graft are removed. The wedge design provides inferior tilt, converting shear forces into compressive forces to enhance fixation and graft integration. Screws positioned in 2 axes ensure stability of the baseplate in both the anteroposterior and mediolateral directions. Finally, a 36-mm glenosphere is implanted (Perform Reverse; Stryker) and a short stem (Medacta Shoulder System; Medacta, Castel San Pietro, Switzerland) is implanted (implant mismatch).14 Surgical pearls and pitfalls and advantages and disadvantages of this technique are summarized in Tables 2 and 3, respectively. Figures 9 and 10 show radiographs immediately postoperative and at 9 months, respectively.Fig 8. The coracoid process is further stabilized using 2 cannulated 4.5-mm partially threaded anterior screws (white arrow). Both screws are directed to engage the posterior tricortical iliac crest autograft, providing additional structural support to the construct.Table 2. Surgical Pearls and Pitfalls for the Sandwich Grafting TechniquePearlsPitfallsUse a full wedge baseplate for enhanced stabilityRisk of improper wedge positioningHarvest iliac graft with sufficient cortical supportRisk of graft fracture during screw placementEnsure proper orientation of coracoid graftIncorrect alignment leading to instabilityDrill multiple holes in glenoid to enhance integrationTable 3Advantages and Disadvantages of the Sandwich TechniqueAdvantagesDisadvantagesCombines vascularized and structural graftsTechnically demandingImproves graft integration ratesIncreased operative timeEnhances fixation and stabilityPotential morbidity from iliac crest harvestingReduces risk of graft lysisSize of coracoid graft may limit applicabilityBenefits from full-wedge baseplate designRequires specialized instrumentationFig 9Postoperative anteroposterior (A) and lateral (B) radiographic views of the right shoulder, demonstrating the final position of the baseplate, screws, coracoid graft, and posterior tricortical iliac crest autograft.Fig 10. Anteroposterior (A) and lateral (B) radiographic views of the right shoulder at 9 months postoperatively, demonstrating maintained position and integration of the baseplate, coracoid graft, and posterior tricortical iliac crest autograft.
Closure and Postoperative Protocol
If possible, the subscapularis is reattached with nonabsorbable sutures15 and eventually reinforced16 to restore anterior stability and functional internal rotation.17 The presence of a graft behind the subscapularis, even without subscapularis split, is not known to induce symptomatic impingement.13^,^18 A layered closure is performed, ensuring adequate soft-tissue coverage. Postoperatively, the arm is immobilized in an abduction pillow for 6 weeks. Passive range-of-motion exercises begin afterward, with gradual progression toward active movements to restore function and optimize outcomes.
Discussion
The sandwich technique is indicated for patients with severe anteroposterior or global bone loss based on Walch classification types B3, C, and D, when standard reconstruction methods are inadequate. This technique integrates biological and mechanical fixation by using a structural autograft, a vascularized autograft, and a metallic baseplate. The vascularized coracoid graft promotes healing and integration, whereas the iliac crest graft provides a stable, rigid foundation for the glenoid construct. The full-wedge baseplate enhances stability by converting shear forces into compressive forces. This dual-graft approach effectively addresses the challenge of achieving stable fixation in cases in which single-graft techniques or augmented baseplates are inadequate.
Glenoid bone grafting in the setting of conversion to RSA has an overall failure rate of 18% regardless of graft type, whether autograft or allograft. Fliegel et al.19 underscored this limitation in their review on biologic graft augmentation for glenoid bone loss during the conversion of failed anatomic shoulder arthroplasty to RSA. Similar findings were reported by Malahias et al.20 in their review, indicating that the all-cause implant re-revision rate for revision RSA with glenoid bone grafting was 21.1%.
Stability is the key advantage of this technique. The anteroposterior orientation of the screws securing the iliac crest and coracoid grafts creates a compressive force across the sandwich construct, enhancing mechanical interlock. In addition, the screws of the baseplate are strategically angled to cross from lateral to medial, providing superior stabilization by integrating the grafts and the native glenoid. The full wedge augmented baseplate further contributes to this stability by transforming shear forces into compressive ones.21 The fixation screws positioned in both the anteroposterior and mediolateral axes further reinforce construct stability which is critical for promoting graft healing and integration.
Another major advantage of the sandwich technique is the reduced risk of graft lysis. In contrast to allografts, which have a greater incidence of resorption and lysis because of their lack of vascularity, this method employs autografts that integrate more effectively with the host bone.11 The vascularized coracoid graft further enhances this integration, reducing the risk of resorption and ensuring a more durable reconstruction.
The incorporation of the full wedge baseplate offers additional advantages over traditional baseplate designs. By providing a large contact area and inferior tilt, the wedge design ensures greater stability and minimizes micromotion at the graft-baseplate interface. These features, as highlighted in recent literature, make it particularly effective for cases of severe glenoid bone loss.22, 23, 24 Limitations are discussed in the Tables 2 and 3.
The sandwich grafting technique provides a biomechanically stable and biologically integrative solution for severe glenoid bone loss. By combining structural and vascularized autografts with a wedge-augmented baseplate, this method enhances fixation, promotes graft incorporation, and restores native glenoid anatomy.
Declaration of generative AI and AI-assisted technologies in the writing process
During the preparation of this work the author(s) used ChatGPT in order to improve grammar, syntax, and clarity of the relevant section. After using this tool/service, the author(s) reviewed and edited the content as needed and take(s) full responsibility for the content of the publication.
Disclosures
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: A.L. is a paid consultant for Arthrex, Stryker, Medacta, and Enovis; received royalties from Stryker and Medacta; is the (co-)founder of FORE, Med4Cast, and BeeMed; owns stock options in Follow Health; is on the board of the French Arthroscopic Society. P.C. reports that he receives royalties from and is a consultant and paid speaker for Stryker and Enovis; is the co-founder of Med4Cast and Follow and is on the board of SECEC and IBSES. All other authors (V.A., G.L., J.Z.) declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Porcellini G.Micheloni G.M.Tarallo L.Paladini P.Merolla G.Catani F.Custom-made reverse shoulder arthroplasty for severe glenoid bone loss: Review of the literature and our preliminary results J Orthop Traumatol 22202123346442510.1186/s 10195-020-00564-6PMC 7815862 · doi ↗ · pubmed ↗
- 2Michelin R.M.Manuputy I.Rangarajan R.Lee B.K.Schultzel M.Itamura J.M.Primary and revision reverse total shoulder arthroplasty using a patient-matched glenoid implant for severe glenoid bone deficiency J Shoulder Elbow Surg 332024 S 93S 1033849262910.1016/j.jse.2024.03.005 · doi ↗ · pubmed ↗
- 3Achors K.Diaz M.A.Simon P.Avoiding glenoid baseplate fixation failure by altering surgical technique for varying bone densities JB JS Open Access 72022 e 22.0000310.2106/JBJS.OA.22.00003 PMC 947831536128255 · doi ↗ · pubmed ↗
- 4John M.P.2nd Wilson J.T.Mesa L.Simon P.Frankle M.A.Revision reverse shoulder arthroplasty for the management of baseplate failure: An analysis of 676 revision reverse shoulder arthroplasty procedures J Shoulder Elbow Surg 3320247077143754327910.1016/j.jse.2023.06.039 · doi ↗ · pubmed ↗
- 5Markes A.R.Cheung E.Ma C.B.Failed reverse shoulder arthroplasty and recommendations for revision Curr Rev Musculoskelet Med 1320201103195694310.1007/s 12178-020-09602-6PMC 7083982 · doi ↗ · pubmed ↗
- 6Rojas J.Choi K.Joseph J.Srikumaran U.Mc Farland E.G.Aseptic glenoid baseplate loosening after reverse total shoulder arthroplasty: A systematic review and meta-analysis JBJS Rev 72019 e 710.2106/JBJS.RVW.18.0013231145263 · doi ↗ · pubmed ↗
- 7Wagner E.Houdek M.T.Elhassan B.T.Sanchez-Sotelo J.Sperling J.W.Cofield R.H.Glenoid bone-grafting in revision to a reverse total shoulder arthroplasty: Surgical technique JBJS Essent Surg Tech 62016 e 353023392810.2106/JBJS.ST.15.00023 PMC 6132614 · doi ↗ · pubmed ↗
- 8Nabergoj M.Denard P.Collin P.Options for glenoid reconstruction: Graft vs. metal vs. combined Franceschi F.Athwal G.Lädermann A.Giovannetti de Sanctis E.Revision shoulder arthroplasty 2024 Springer Cham New York 169186