CO2 Insufflation in Cartilage Repair Using Minced Autologous Cartilage, Platelet-rich Plasma, and Autologous Thrombin: Enhancing Techniques for Repairing Knee Articular Cartilage Defects
Umer Butt, Filip Vuletić, Riccardo Cristiani, Mahenau Afridi, Zainab Aqeel Khan, Yasir Hussain, Anders Stålman

TL;DR
This paper introduces a new technique for knee cartilage repair using CO2 insufflation to improve graft placement and integration.
Contribution
The novel use of CO2 insufflation in the AutoCart technique enhances precision and biological effectiveness during cartilage repair.
Findings
CO2 insufflation creates a dry environment for more accurate defect preparation and graft placement.
It prevents biologically active components from being washed away, improving graft integration.
The method reduces fluid accumulation and leakage into surrounding tissues.
Abstract
Injuries to the articular cartilage are challenging to treat because of its limited intrinsic healing capacity, leading to the exploration of various repair methods. The AutoCart technique combines minced autologous cartilage, platelet-rich plasma, and autologous thrombin, with promising clinical results. A key advancement is the use of carbon dioxide (CO2) insufflation during arthroscopy, which creates a dry environment and significantly improves the accuracy of defect preparation and graft placement. Unlike traditional fluid distention, CO2 insufflation prevents biologically active components of the graft from being washed away, allowing for precise placement and integration within the cartilage defect. Furthermore, it reduces fluid accumulation and leakage into the surrounding soft tissue. In this Technical Note, we describe a technique for performing AutoCart cartilage repair using…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1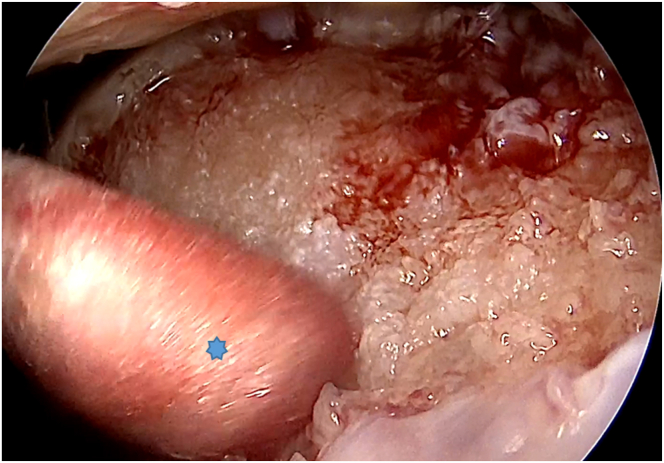 Figure 2
Figure 2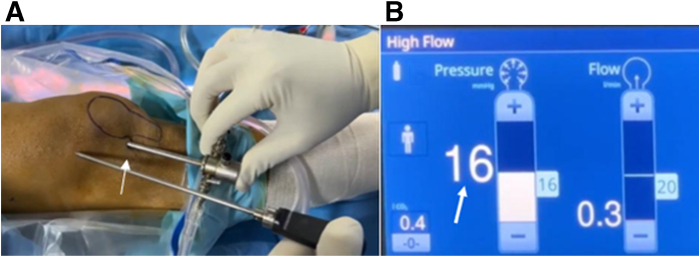 Figure 3
Figure 3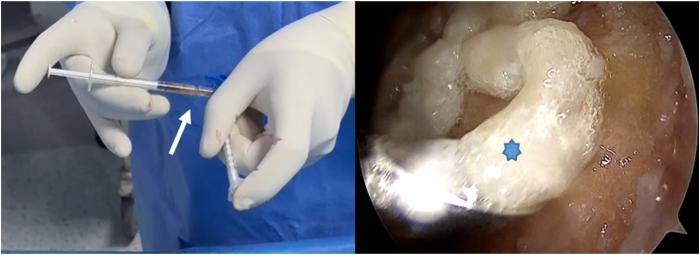 Figure 4
Figure 4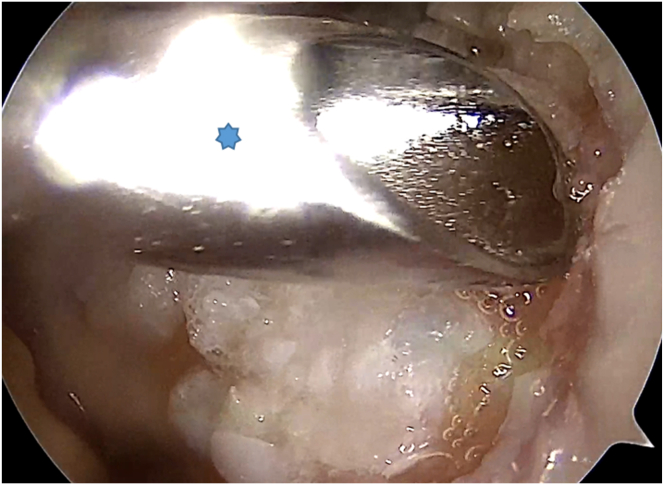 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsKnee injuries and reconstruction techniques · Osteoarthritis Treatment and Mechanisms · Periodontal Regeneration and Treatments
Articular cartilage injuries in the knee remain challenging as a result of the tissue's limited intrinsic healing capacity.1 Various repair strategies have been developed, including microfracture, autologous chondrocyte implantation, and osteochondral graft transplantation.2 Clinical outcomes appear to be linked to the quality of the repair tissue, with cell-based approaches showing promising results.3^,^4 In this context, the AutoCart (Arthrex, Munich, Germany) technique has emerged as a potential option.5
A single-stage procedure combining minced autologous cartilage, platelet-rich plasma (PRP), and autologous thrombin has been developed to promote cartilage repair and regeneration.5 Although evidence remains limited, early in vitro and in vivo studies, along with recent clinical follow-up, suggest encouraging outcomes, including pain reduction and improved activity levels up to 5 years postoperatively.5, 6, 7 Carbon dioxide (CO_2_) insufflation, widely used in laparoscopic surgery because of its rapid absorption and exhalation, has been adapted for knee arthroscopy to create a dry environment and enhance visualization.8, 9, 10 Recent studies suggest that CO_2_ improves joint distraction, reduces surgical time, and facilitates clearer visualization compared with traditional saline distention, without significant complications reported.10
In cartilage repair procedures like AutoCart, maintaining a dry environment is crucial for effective graft placement, because it reduces washout of bioactive components.11 CO_2_ insufflation may decrease postoperative swelling and discomfort by limiting fluid extravasation.11^,^12 Although early results are promising, further research is needed to validate the benefits of CO_2_ in knee cartilage repair. This Technical Note outlines the AutoCart technique with CO_2_ insufflation, providing key surgical steps, tips, and common pitfalls for practitioners in arthroscopic cartilage surgery (Video 1).
Surgical Technique
Patient Setup, Cartilage Harvesting, and Bone Bed Preparation (Fluid Arthroscopy)
The patient is positioned supine, and a high-padded tourniquet is applied. An anterolateral portal is created for diagnostic evaluation, followed by the creation of an anteromedial portal. Hoffa’s fat pad may be resected for better visibility. The cartilage defect is assessed, and unstable cartilage is debrided with a curette. Cartilage fragments are collected using a 3-mm Arthrex Sabre (Arthrex, Munich, Germany) shaver for graft preparation (Fig 1).Fig 1. An arthroscopic view of the right knee through the anterolateral portal shows a trochlear defect, with cartilage fragments being removed from its edges using a 3-mm Arthrex Sabre shaver (asterisk) from the anteromedial portal.
After harvesting the cartilage, the size of the lesion is measured, and the bone bed is prepared using curettes and burrs to create a clean and stable surface while removing any debris or necrotic tissue. Once bone preparation is complete, any saline in the joint is drained, and residual moisture is removed with cotton swabs (Fig 2). CO_2_ insufflation is then initiated through the arthroscope, using a laparoscopic insufflator set at a pressure of up to 20 mm Hg and a flow rate of up to 20 L/min, establishing a dry working environment essential for accurate graft placement (Fig 3).Fig 2. An arthroscopic view of the right knee through the anterolateral portal shows residual moisture being removed with cotton swabs inserted through the anteromedial portal (asterisk).Fig 3(A) Arthroscope placed in a high anterolateral portal of the right knee (arrow). (B) A modified laparoscopic insufflator fills the knee joint with CO_2_ gas up to a pressure of 20 mm Hg (arrow).
Graft Preparation and Application (Dry Arthroscopy)
Minced cartilage chips are mixed with 0.5 to 1.0 mL of PRP for consistency (Fig 4). Before anesthesia, 10 to 15 mL of blood is drawn from the cubital vein, and 3 mL of PRP is processed with the Thrombinator system (Arthrex) for 10 to 15 minutes to create autologous thrombin. During implantation, autologous thrombin is applied to the cartilage-PRP mixture to enhance fibrin clot formation and stabilize the graft. Optionally, a thin layer of fibrin can be added for sealing. The graft is then spread with a spatula to fill about 80% to 90% of the defect height without needing to match the surrounding cartilage level (Fig 5). Steps of the surgical technique, along with tips and potential pitfalls, are outlined in Table 1.Fig 4. On the left side of the picture, minced cartilage chips are mixed with 0.5 to 1.0 mL of platelet-rich plasma to achieve a cohesive consistency (arrow), using 2 syringes. On the right side, there is an arthroscopic view of the right knee taken through the anteromedial portal, which shows a pasty graft substance (asterisk) applied through the obturator device.Fig 5. Arthroscopic view of the right knee through the anterolateral portal shows the graft being gently spread with a spatula or obturator device (asterisk) from the anteromedial portal, filling approximately 80% to 90% of the defect height.Table 1. Surgical Steps, Pearls, and Pitfalls of CO_2_ Insufflation for Performing the AutoCartSurgical StepPearlsPitfallsPortal creationUse a small stab incision and a hemostat clamp or blunt trocar to puncture the joint capsule. This technique seals soft tissue and reduces gas leakage.A “loose seal” portal may increase gas leakage.Placement of cannula and debridement of the Hoffa’s fat padReduces obstruction of the Hoffa’s fat pad and improves the visualization of the chondral defect.Potential interposition from the Hoffa’s fat pad.CO_2_ insufflationThe insufflation pump is set at 20 mm Hg.Nonoptimal pressure settings could impair visualization.Bony bed preparationCurettes and shavers create an even surface, which enhances graft placement.Improper bony bed preparation may lead to poor repair tissueformation.Graft preparationProper graft preparation is essential to create a pastelike substance for uniform distribution and initial stability in the defect area.Poor graft preparation can make the application more difficult.Graft applicationFilling from 80% to 90% of the surrounding healthy cartilage level is sufficient.13Overstuffing the defect may later lead to graft hypertrophy.CO_2_, carbon dioxide.
Discussion
Gas insufflation during the arthroscopic AutoCart cartilage repair procedure offers several benefits but also presents specific limitations (Table 2). Dry arthroscopy enhances visualization and minimizes technical errors, and although CO_2_ was once the preferred method because of its high solubility in blood, it has largely been replaced by saline.8, 9, 10, 11, 12, 13, 14 Notably, Riddell13 used CO_2_ in more than 3,000 knee arthroscopies without complications, showcasing its effectiveness. In 2006, Coletti et al.15 showed its use during matrix-induced autologous chondrocyte implantation and reported no complications linked to CO_2_. In a review, Vascellari et al.16 found no complications related to the use of CO_2_ in Coletti et al.’s patient group. Continuous CO_2_ inflation may maintain a stable joint environment, promoting graft integration and reducing fluid leakage into soft tissues.13^,^16 Earlier studies have shown that dry arthroscopic procedures reduce swelling and accelerate recovery after joint surgeries.10^,^14^,^16 This reduction in swelling can alleviate postoperative pain and promote quicker rehabilitation.10 However, it is essential to recognize its limitations and consider the existing literature. The dry arthroscopy method requires a system for fluid irrigation and gas insufflation, necessitating alternating phases for rinsing and the procedure itself.9 Current literature indicates no increased systemic risks associated with gas leakage.10^,^16 It highlights the importance of the surgeon's experience and the need for risk mitigation strategies during the procedure.10^,^13^,^15^,^16Table 2. Advantages and Disadvantages of CO_2_ Insufflation for Performing the AutoCartAdvantagesDisadvantagesDry conditions enable the precise placement of biomaterials without risking the washout of bioactive components.CO_2_ can cause lens fogging, requiring anti-fogging measures.It removes floating debris and blood, providing a clearer view of cartilage defects.Limited experience with CO_2_ insufflation among orthopaedic surgeons.Less fluid extravasation leads to decreased joint swelling and discomfort after surgery.Current evidence on long-term outcomes is still scarce.Minimal risk of gas embolism.Specialized pumps are required for CO_2_ insufflation and may not be widely available.CO_2_, carbon dioxide.
In conclusion, CO_2_ insufflation improves visualization and creates favorable conditions for cartilage repair in knee arthroscopy.15^,^16 Yet, careful management of intra-articular pressure and attention to the learning curve are essential, with further research needed on its long-term effects.
Disclosures
All authors (U.B., F.V., R.C., M.A., Z.A.K., Y.H., A.S.) declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Solanki K.Shanmugasundaram S.Shetty N.Kim S.J.Articular cartilage repair & joint preservation: A review of the current status of biological approach J Clin Orthop Trauma 22202110160210.1016/j.jcot.2021.101602 PMC 848824034631411 · doi ↗ · pubmed ↗
- 2Richter D.L.Schenck R.C.Jr.Wascher D.C.Treme G.Knee articular cartilage repair and restoration techniques: A review of the literature Sports Health 820161531602650218810.1177/1941738115611350 PMC 4789925 · doi ↗ · pubmed ↗
- 3Jarecki J.Waśko M.K.Widuchowski W.Knee cartilage lesion management-current trends in clinical practice J Clin Med 12202364343789257710.3390/jcm 12206434 PMC 10607427 · doi ↗ · pubmed ↗
- 4Roelofs A.J.Rocke J.P.De Bari C.Cell-based approaches to joint surface repair: A research perspective Osteoarthritis Cartilage 2120138929002359817610.1016/j.joca.2013.04.008PMC 3694304 · doi ↗ · pubmed ↗
- 5Blanke F.Warth F.Oehler N.Siegl J.Prall W.C.Autologous platelet-rich plasma and fibrin-augmented minced cartilage implantation in chondral lesions of the knee leads to good clinical and radiological outcomes after more than 12 months: A retrospective cohort study of 71 patients J Exp Orthop 112024 e 7005110.1002/jeo 2.70051 PMC 1148052139415804 · doi ↗ · pubmed ↗
- 6Ossendorff R.Walter S.G.Schildberg F.A.Biologic principles of minced cartilage implantation: A narrative review Arch Orthop Trauma Surg 1432023325932693638565510.1007/s 00402-022-04692-y PMC 10191961 · doi ↗ · pubmed ↗
- 7Runer A.Ossendorff R.Öttl F.Autologous minced cartilage repair for chondral and osteochondral lesions of the knee joint demonstrates good postoperative outcomes and low reoperation rates at minimum five-year follow-up Knee Surg Sports Traumatol Arthrosc 312023497749873763413610.1007/s 00167-023-07546-1PMC 10598129 · doi ↗ · pubmed ↗
- 8Park E.Y.Kwon J.Y.Kim K.J.Carbon dioxide embolism during laparoscopic surgery Yonsei Med J 5320124594662247698710.3349/ymj.2012.53.3.459PMC 3343430 · doi ↗ · pubmed ↗