Lemierre’s Syndrome
Kiyozumi Suzuki, Hiromasa Otsuka

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
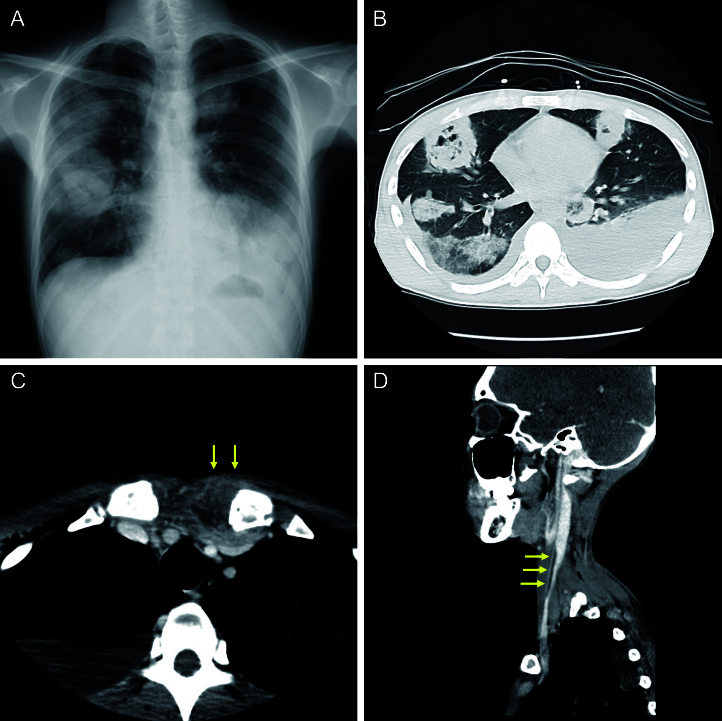 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOtolaryngology and Infectious Diseases · Infectious Diseases and Tuberculosis · Hematological disorders and diagnostics
A previously healthy 23-year-old man presented to a local clinic with a 1-week history of fever and sore throat, which progressed to cough, hemoptysis, chest pain, and dyspnea. The patient was in shock and experiencing respiratory failure. A chest radiograph revealed multiple pulmonary masses (Figure 1A), raising suspicion for metastatic lung cancer, and prompting transfer to our hospital.
On arrival, laboratory data revealed elevated inflammatory markers, multiorgan dysfunction, and disseminated intravascular coagulation. Computed tomography showed numerous cavitating pulmonary lesions suggestive of septic emboli, empyema (Figure 1B), sternoclavicular arthritis (Figure 1C), and a thrombus in the right internal jugular vein (Figure 1D). Blood cultures yielded growth of Fusobacterium necrophorum, susceptible to most β-lactam antibiotics and clindamycin. These findings confirmed the diagnosis of Lemierre’s syndrome (LS). The patient was administered meropenem and underwent chest drainage. After significant clinical improvement, antibiotic therapy was switched to oral amoxicillin-clavulanic acid, completing a full 3-month antibiotic course, which resulted in full recovery.
LS is a rare but life-threatening condition that primarily affects otherwise healthy young adults and is characterized by an antecedent oropharyngeal infection, Fusobacterium septicemia, thrombophlebitis, and metastatic infections ^(1)^. The lungs are the most commonly affected site of metastatic infection in LS, often presenting with bilateral necrotic pulmonary emboli, pleural effusions, empyema, or lung abscesses ^(1)^.
Although imaging studies are key diagnostic tools for LS, early diagnosis and appropriate therapy require a thorough understanding of this distinctive condition. Clinicians encountering oropharyngeal infections in routine clinical practice should be familiar with the clinical features of this potentially fatal disease.
Article Information
Author Contributions
Kiyozumi Suzuki: Writing - Original draft, Methodology. Hiromasa Otsuka: Methodology, Writing - review & editing. All authors critically reviewed the manuscript.
Conflicts of Interest
None
IRB Approval Code and Name of the Institution
In this study, Institutional Review Board approval was not required. Consent was obtained from the patient for the use of images for publication.
The reference list from the paper itself. Each links out to its DOI / PubMed record.