B‐Type Natriuretic Peptides Levels in Patients With Beta‐Thalassemia Major and Correlations With Biomarkers: A Systematic Review and Meta‐Analysis
Mohamed S. K. Salih, Amna H. Mohamed, Elsara M. A. Mirghani, Mohammed Y. K. Makki, Ola A. M. Ahmed, Esraa T. S. Mohammed, Hana H.M. Hassan, Nada Omar, Esraa M. A. Garalnabi, Sagad O. O. Mohamed

TL;DR
This study finds that patients with beta-thalassemia major have elevated B-type natriuretic peptides, indicating a higher risk of heart problems.
Contribution
The study provides a meta-analysis of BNP and NT-proBNP levels in beta-thalassemia major and their correlations with biomarkers.
Findings
NT-proBNP and BNP levels are significantly higher in beta-thalassemia major patients compared to healthy controls.
NT-proBNP is significantly correlated with serum ferritin, E/E′ ratio, and patient age.
Elevated B-type natriuretic peptides suggest early myocardial stress and subclinical heart disease in these patients.
Abstract
Patients with beta‐thalassemia major are prone for developing cardiovascular complications. Early identification of patients at risk is important. B‐type natriuretic peptides such as brain natriuretic peptide (BNP) and N‐terminal pro‐BNP (NT‐proBNP) are sensitive indicators of cardiac dysfunction. This review synthesizes the existing evidence on the levels of B‐type natriuretic peptides in beta‐thalassemia major and their relationship with markers of cardiac dysfunction and other biomarkers. A systematic review was conducted according to PRISMA guidelines. The search was performed in the PubMed, Web of Science, ScienceDirect, and World Health Organization Virtual Health Library Regional Portal. Pooled standardized mean differences (SMD) and correlation coefficients (r) with 95% confidence intervals (CI) were calculated to investigate the differences in B‐type natriuretic peptides…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
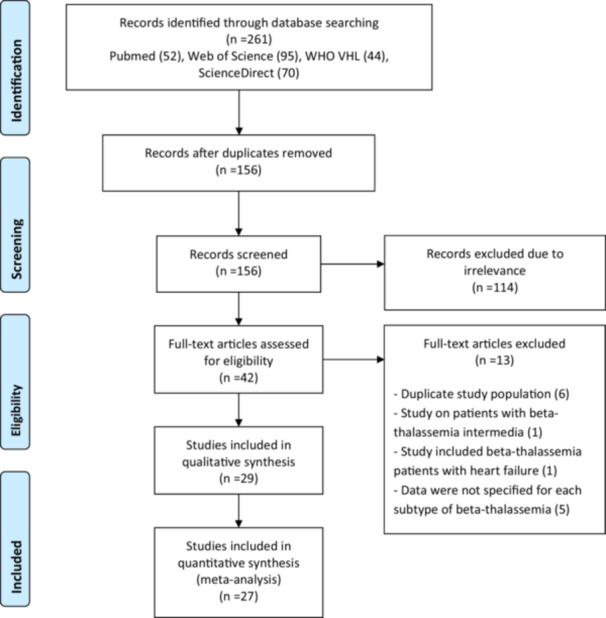 Figure 1
Figure 1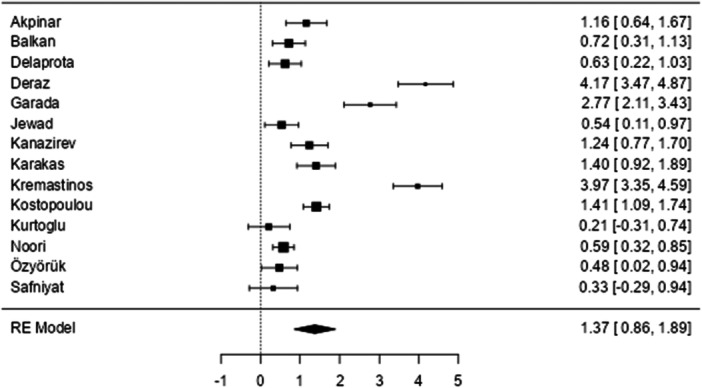 Figure 2
Figure 2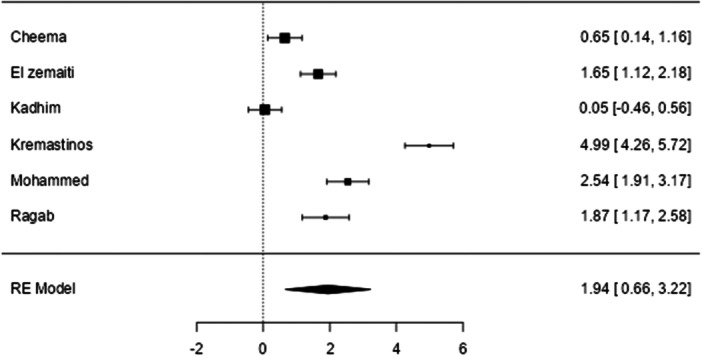 Figure 3
Figure 3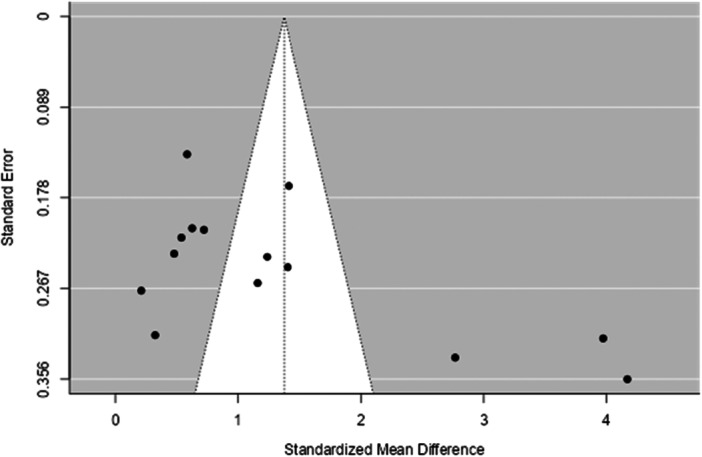 Figure 4
Figure 4| Study | Year | Country | Age group | Age mean | No. of patients | B‐type natriuretic peptides | Quality assessment |
|---|---|---|---|---|---|---|---|
| Akpinar et al. | 2007 | Turkey | Adults | 23.5 (4.5) | 34 | NT‐proBNP | 6/8 |
| Alizadeh et al. | 2016 | Iran | 11–35 years | Mean of 17.9 | 50 | NT‐proBNP | 7/8 |
| Ambrawati et al. | 2016 | Indonesia | Children | 10.9 (2.16) | 34 | NT‐proBNP | 6/8 |
| Aygunes et al. | 2022 | Turkey | Children | 82.2 months (59.1) | 39 | Pro‐BNP | 6/8 |
| Balkan et al. | 2011 | Turkey | Adults | 24 (4.2) | 49 | NT‐proBNP | 6/8 |
| Cheema et al. | 2012 | Pakistan | 6‐21 years | Median of 12 | 62 | BNP | 8/8 |
| Chrysohoou et al. | 2006 | Greece | Adults | 25.54 [ | NT‐proBNP | 6/8 | |
| Delaprota et al. | 2013 | Greece | Adults | 34 (6.02) | 187 | NT‐proBNP | 8/8 |
| Deraz et al. | 2020 | Egypt | Children | 10.5 (2.7) | 50 | NT‐proBNP | 6/8 |
| Elzemaiti et al. | 2019 | Egypt | 16‐45 years | n/a | 45 | BNP | 6/8 |
| Garada et al. | 2016 | Bahrain | Adults | 15.92 (8.92) | 38 | NT‐proBNP | 6/8 |
| Goudarzipour et al. | 2017 | Iran | Children | 17.1 (5.3) | 35 | NT‐proBNP | 7/8 |
| Jewad et al. | 2024 | Iraq | All groups | 12.2 (3.8 | 46 | NT‐proBNP | 6/8 |
| Kadhim et al. | 2024 | Iraq | Adults | 22.67 (4.78) | 30 | BNP | 6/8 |
| Kanazirev et al. | 2017 | Bulgaria | Adults | 31.6 (9.56) | 87 | NT‐proBNP | 6/8 |
| Karakas et al. | 2022 | Turkey | 11 to 21 years | 17.15 (3.13) | 82 | NT‐proBNP | 8/8 |
| Karamanou et al. | 2013 | Greece | Adults | 36 (8.2) | 88 | NT‐proBNP | 8/8 |
| Kautsar et al. | 2019 | Indonesia | adolescent | 14.01 (1.662) | 68 | NT‐proBNP | 8/8 |
| Kostopoulou et al. | 2013 | Greece | 5 to 51 years | 29 [ | 180 | NT‐proBNP | 8/8 |
| Kremastinos et al. | 2010 | Greece | Adults | 26.49 (11.55) | 120 | ProBNP & NT‐proBNP | 8/8 |
| Kurtoglu et al. | 2017 | Turkey | Adults | 23.87 (2.76) | 56 | NT‐proBNP | 7/8 |
| Mehrzad et al. | 2016 | Iran | Adults | 28 (6.4) | 50 | NT‐proBNP | 8/8 |
| Mohammed et al. | 2019 | Egypt | Children | 12.15 (2.28) | 70 | BNP | 7/8 |
| Noori et al. | 2019 | Iran | Children | Mean of 16.7 | 114 | NT‐proBNP | 7/8 |
| Özyörük et al. | 2014 | Turkey | Children | 8.9 (3.5) | 78 | NT‐proBNP | 6/8 |
| Ragab et al. | 2015 | Egypt | 4 to 20 years | 10.9 (4.86) | 45 | BNP | 8/8 |
| Safniyat et al. | 2020 | Iran | 8 to 40 years | 26.3 (7.5) | 123 | NT‐proBNP | 7/8 |
| Singh et al. | 2017 | India | > 10 years | 16.4 (5.1) | 105 | NT‐proBNP | 7/8 |
| Tanner et al. | 2006 | UK & Italy | Adults | 30 (5.3) | 167 | NT‐proBNP | 6/8 |
| Study | Main findings |
|---|---|
| Aessopos et al. | BNP was higher in thalassemia patients with heart failure. BNP was correlated with echocardiographic parameters (E and E/A ratio) in those with normal systolic function. |
| Akpinar et al. | NT‐proBNP was significantly associated with E/A ratio |
| Alizadeh et al. | NT‐proBNP was not correlated with age, sex, Hb level, or diastolic dysfunction |
| Ambrawati et al. | NT‐proBNP was correlated with vitamin D, but not with age, ferritin, and Hb levels |
| Aygunes et al. | ProBNP values were correlated with endocan and Asymmetric dimethyl arginine (ADMA) |
| Balkan et al. | NT‐proBNP was correlated with serum ferritin and echocardiographic parameters (E |
| Cheema et al. | BNP was correlated with E/E′ ratio. The ROC curve analysis for BNP at a cut‐off value of 84.3 pg/mL was highly accurate (AUC = 0.86) in ruling out diastolic dysfunction (based on E/E′ ratio), with a sensitivity of 80% and specificity of 88%. |
| Chrysohoou et al. | BNP was significantly associated with echocardiographic parameter (E/A ratio, S′, and deceleration time) |
| Delaprota et al. | NT‐proBNP was correlated with age, cardiac iron concentration, hs‐CRP, and NTBI. |
| Deraz et al. | NT‐proBNP was correlated with serum ferritin and echocardiographic parameters (E, E/A ratio, E/E ratio, and S |
| Elzemaiti et al. | NT‐proBNP was correlated with serum ferritin and frequency of blood transfusion |
| Garada et al. | NT‐proBNP was correlated with the E/E′ ratio |
| Goudarzipour et al. | NT‐proBNP was correlated with heart failure and cardiac MRI‐T2 |
| Jewad et al. | NT‐proBNP was correlated with age, GDF‐15, and renalase, but not with sex or serum ferritin |
| Kadhim et al. | No correlation between NT‐ProBNP and serum ferritin or troponin |
| Kanazirev et al. | NT‐proBNP was correlated with only one echocardiographic parameter (left atrial volume index) based on NT‐pro‐BNP > 125 pg/ml or less categorization |
| Karakas et al. | NT‐proBNP was not correlated with cardiac MRI‐T2 |
| Karamanou et al. | BNP was higher in the diastolic dysfunction group (based on E/E′ ratio) without reaching statistical significance |
| Kautsar et al. | NT‐proBNP was not correlated with cardiac MRI‐T2 |
| Kostopoulou et al. | NT‐proBNP was significantly associated with iron load, serum ferritin, diastolic dysfunction (E/E′ ratio) and AF. |
| Kremastinos et al. | Both BNP and NT‐proBNP were correlated with serum ferritin and E/E′ ratio. The ROC analysis for NT proBNP at a cut point of 49.2 pg/mL was highly accurate (AUC = 0.97) in ruling out diastolic dysfunction (based on E/E′ ratio) with a sensitivity of 93.7% and a specificity of 89.6%. |
| Kurtoglu et al. | No significant difference detected in NT‐proBNP between patients and controls. |
| Mehrzad et al. | NT‐proBNP was not correlated with cardiac MRI‐T2, age, chelation therapy, or serum ferritin. |
| Mohammed et al. | BNP was correlated with Impaired EF%. The ROC curve analysis for BNP at a cut‐off value of 31 pg/mL was highly accurate (AUC = 0.99) in predicting myocardial dysfunction, with a sensitivity of 93% and specificity of 100%. |
| Noori et al. | NT‐proBNP was correlated with echocardiographic parameters (EF, FS, QT) and BMI |
| Özyörük et al. | NT‐proBNP was correlated with age and echocardiographic parameters (right ventricular E/E′ ratio, left ventricle mass index, and left ventricular end diastole diameter) |
| Ragab et al. | BNP was correlated with serum ferritin and echocardiographic parameters (E/E′ ratio, E, and IRT). The ROC curve analysis for BNP at a cut‐off value of 28.5 pg/ml was highly accurate (AUC = 0.86) in ruling out diastolic dysfunction based on E/E′ ratio, with a sensitivity of 100%, specificity of 81.9%, negative predictive value of 100%, and positive predictive value of 75%. |
| Safniyat et al. | NT‐proBNP was correlated with LVIDd but not with cardiac MRI‐T2, E/E′ ratio, and serum ferritin in all patients groups (including beta‐thalassemia intermedia). |
| Singh et al. | NT‐proBNP was correlated with diastolic dysfunction, LVESD, E/E, and E/A ratios. The ROC curve analysis for NT‐proBNP at a cut‐off value of 81 pg/mL was highly accurate (AUC = 0.868) in predicting of diastolic dysfunction, with a sensitivity of 87.5% and specificity of 85.7% |
| Tanner et al. | BNP was correlated with cardiac iron overload (MRI‐T2) |
| B‐type natriuretic peptides | Outcome | No. of studies | Pooled correlation | Begg′s test ( | Egger′s test ( | I2 test |
|---|---|---|---|---|---|---|
| NT‐proBNP | Age | 7 |
| 0.362 | 0.257 | 72.89% |
| Ferritin | 8 |
| 0.901 | 0.920 | 92.58% | |
| MRI‐T2 | 4 |
| 0.333 | 0.150 | 90.34% | |
| E/E ratio | 5 |
| 0.083 | 0.002 | 72.25% | |
| BNP | Ferritin | 4 |
| 1.00 | 0.877 | 66.41% |
- —The authors received no specific funding for this work.
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHemoglobinopathies and Related Disorders · Heart Failure Treatment and Management · Erythropoietin and Anemia Treatment
Background
1
Beta‐thalassemia is a prevalent inherited blood disorder affecting approximately 1.5% of the global population [1]. It is particularly common in the Mediterranean, North Africa, and Central Africa, but due to increased migration, its incidence has significantly expanded into other areas, including Northern Europe and North America [2]. This genetic disorder results from mutations in the beta‐globin gene, leading to reduced or absent production of beta‐globin chains, which are essential components of hemoglobin [1, 2, 3, 4]. The defective hemoglobin function disrupts erythropoiesis, causing severe chronic anemia and a spectrum of clinical manifestations. Based on genetic defects and disease severity, beta‐thalassemia is classified into three major categories: beta‐thalassemia major, thalassemia intermedia, and thalassemia minor [2, 3]
A major complication of the disease is iron overload due to repeated blood transfusions, leading to iron deposition in various organs, including the liver, endocrine glands, and heart [5]. Among these, cardiac complications are the most severe and life‐threatening, with iron‐induced cardiomyopathy being a leading cause of mortality in this patient population [6]. With repeated blood transfusions, iron accumulates in the heart, increasing the risk of heart failure and arrhythmias [6]. Iron chelation therapy is crucial for mitigating these complications, but early and reliable markers of cardiac dysfunction are essential for timely intervention [7, 8]
While cardiac T2* magnetic resonance imaging (MRI‐T2) can detect iron‐related heart complications early, its practical limitations regarding high costs and lengthy scan times highlight the need for more practical and accessible biomarkers [9, 10]. Finding alternative diagnostic tools that are both practical and widely available would significantly improve the monitoring and management of these cardiac complications.
B‐type natriuretic peptides (Brain Natriuretic Peptide [BNP], ProBNP, and N‐terminal proBNP [NT‐proBNP]), are secreted by cardiomyocytes in response to ventricular wall stress and have been investigated as potential early indicators of cardiac dysfunction [11]. They serve as crucial biomarker for investigating both symptomatic and asymptomatic heart dysfunction and their levels correlate significantly with the severity of cardiac conditions, making them valuable tools in clinical settings [12]. Several studies have explored the correlation between B‐type natriuretic peptides levels and echocardiographic markers of cardiac dysfunction in the general population. However, findings from studies on beta‐thalassemia populations are limited and have been inconsistent across studies. Their clinical application in beta‐thalassemia is currently hampered by significant inconsistencies across published studies. Individual studies report conflicting findings on the strength of the correlation between NT‐proBNP and key cardiac parameters, and propose a wide range of diagnostic cut‐off values, making it difficult for clinicians to interpret results in a standardized way. This lack of consensus is a barrier to the development of evidence‐based clinical guidelines for cardiac monitoring in beta‐thalassemia population.
Therefore, this systematic review and meta‐analysis aims to address this study gap. We systematic review aims to synthesize available evidence and provide a comprehensive, generalizable estimate of the correlation between B‐type natriuretic peptides levels and markers of cardiac dysfunction in beta‐thalassemia patients, thereby contributing to improved clinical management and patient outcomes in this vulnerable patient population.
Methods
2
Search approach and studies inclusion criteria:
This review followed the guidelines outlined in the Preferred Reporting Items for Systematic Reviews and Meta‐Analyses (PRISMA) statement [13]. The systematic review was previously registered on the Open Science Framework platform (https://osf.io/zey9v). To identify relevant literature, an electronic literature search was conducted via the databases of PubMed, Web of Science, ScienceDirect, and World Health Organization Virtual Health Library Regional Portal. The search strategy did not impose any limitations based on geographical location or publication date, aiming to capture the widest possible range of relevant studies.
We sought to determine whether there is a significant difference in the levels of B‐type natriuretic peptides (BNP, ProBNP, and NT‐proBNP) between beta‐thalassemia patients and healthy subjects, and to investigate the relationship between these peptides and any identified markers of cardiac dysfunction in beta‐thalassemia patients. Therefore, PECO and PEO models were used to frame the following research questions:
Primary research question: in patients with beta‐thalassemia (Population), how does the presence of beta‐thalassemia (Exposure) compared to healthy individuals (Comparator) affect the levels of natriuretic peptides (Outcome)? Secondary research question: in patients with beta‐thalassemia (Population), how do varying levels of natriuretic peptides (Exposure) correlate with any identified markers of cardiac dysfunction (Outcome)?
The electronic search was conducted on literature from inception up to December 2024, using the following key words: (thalassemia OR “beta‐thalassemia” OR β‐thalassemia) AND (Natriuretic peptide OR B‐type natriuretic peptide OR brain natriuretic peptide OR BNP OR Amino terminal pro‐brain natriuretic peptide OR NT‐proBNP OR pro‐BNP OR proBNP OR NTproBNP OR N‐terminal pro‐brain natriuretic peptide OR N‐terminal pro‐BNP). The details of the search strategy used for this review were presented in (Additional file 1). In addition, the references in the included articles were screened to make sure that no relevant studies have been missed. To identify potentially relevant gray literature, we conducted searches in Google Scholar along with our searches in major databases. All the publications were uploaded to Endnote software for initial screening of titles and abstracts as well as to remove duplicates.
Inclusion and Exclusion Criteria
2.1
The selection process involved a two‐step approach. Initially, the titles and abstracts of all identified articles were screened by three independent reviewers to identify potentially relevant studies. Then, we did a full‐text review of the selected studies in detail to assess their eligibility according to our set inclusion criteria. The inclusion criteria for the articles in this review were cross‐sectional, case‐control, and cohort studies that supplied data on B‐type natriuretic peptides levels. Case reports, editorials, reviews, abstracts, and studies with incomplete data for the variables of interest were excluded. The initial inter‐reviewer agreement for study selection was calculated with a kappa statistic of 0.70.
Quality assessment and data extraction:
To evaluate the methodological rigor of the studies included for potential biases, critical appraisal checklists from the Joanna Briggs Institute were utilized (https://jbi.global/critical-appraisal-tools). These checklists facilitate assessment of the possibility of bias in study design, conduct, and data analysis. Data retrieved from every study included author, year, region, number of patients, age group of participants, and levels of B‐type natriuretic peptides for all groups. In cases where a study reported medians and interquartile ranges, mean and SD were estimated using the method described by Wan et al. [14]. In cases where a study provided means and SDs for multiple groups of asthmatic patients, we combined them into a single set of values for each study [15]. Any discrepancies during data extraction or quality assessment were resolved through discussion and consensus.
Statistical Analysis
2.2
The statistical analyses were performed by using Jamovi software (https://www.jamovi.org) to calculate the pooled standardized mean difference (SMD) and its 95% confidence intervals (CI). In addition, a meta‐analysis of correlation coefficient (r) was done to investigate the relationships between B‐type natriuretic peptides and various biomarkers in beta‐thalassemia patients. To obtain standardized effect sizes for each correlation coefficient, Fisher′s r‐to‐z transformation was applied by transforming the correlation coefficients into z‐scores, which are normally distributed, allowing for a more accurate estimation of the overall effect size and standard error. The overall pooled correlation coefficients were obtained by transforming the values back to the r scale using the inverse of the Fisher′s r‐to‐z transformation.
A random‐effects model, using DerSimonian–Laird method, was used for calculation of the pooled effect sizes to account for studies heterogeneity, which was evaluated using the I² statistic. To test for the presence of publication bias—a potential source of bias due to the tendency for studies with statistically significant results to be published more often—we performed statistical analyses using both Begg′s and Egger′s regression tests. In addition, funnel plots were visually checked to evaluate publication bias for analyses involving more than 10 studies [16, 17]. When there was evidence of a publication bias, the Duval and Tweedie trim‐and‐fill method was applied to account for potentially missing studies [18].
Due to the specific functionalities of OpenMeta‐Analyst software (version 10.10) (http://www.cebm.brown.edu/openmeta/) [19], leave‐one‐out sensitivity analyses was conducted, using this software, to evaluate the robustness of the meta‐analyses through assessing the influence of individual studies. In addition, meta‐regression was done to assess how specific study characteristics are associated with variation in effect sizes. The significance level for all analyses was set at 0.05.
Results
3
Studies characteristics:
The schematic flow of the study identification and selection process is presented in Figure 1. The initial electronic database search yielded a total of 261 records. Following the removal of duplicate entries, 156 studies remained. These 156 studies underwent a thorough title and abstract screening process. During this stage, 114 studies were excluded for failing to meet our pre‐specified inclusion criteria. Full texts of the remaining 42 records were screened, leading to the exclusion of 13 records due to the reasons listed in Figure 1. Ultimately, a total of 29 studies were selected for the systematic review [8, 11, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46].
Flow chart for studies selection process.
Most of the included studies focused on measuring NT‐proBNP, whereas a smaller group of six studies evaluated BNP, and only one study examined proBNP. Study publications ranged from 2006 to 2024, with a total of 1128 patients with beta‐thalassemia major. The main features of the selected studies, as well as risk of bias assessment, are presented in Table 1.
B‐Type Natriuretic Peptides Measurements
3.1
We conducted meta‐analyses to assess the difference in the mean levels of B‐type natriuretic peptides between patients and the healthy individuals (Figures 2, 3). The results showed that people with beta‐thalassemia major had significantly higher NT‐proBNP measurements than healthy individuals, with pooled effect size SMD = 1.37 (95% CI: 0.856–1.893, p < 0.001). Heterogeneity was high according to the I^2^ test (94.59%). The publication bias test was significant for Egger′s test (p = 0.001) but not for Begg′s test (p = 0.101) (Figure 4). The Duval and Tweedie trim‐and‐fill analysis did not identify any missing studies, an indication that the adjusted estimate was consistent with the original finding and unaffected by substantial publication bias.
Forest plot for the pooled SMD of NT‐proBNP between patients with beta‐thalassemia major and healthy individuals.
Forest plot for the pooled SMD of BNP between patients with beta‐thalassemia major and healthy individuals.
Funnel plot for the analysis of pooled SMD of NT‐proBNP between patients with beta‐thalassemia major and healthy individuals.
There were six studies with explicit data to calculate the SMD of BNP estimates among patients with beta‐thalassemia major. The results showed that the patients had significantly higher BNP values than healthy individuals, with pooled effect size SMD = 1.94 (95% CI: 0.665–3.220, p = 0.003). Heterogeneity was high (96.47%) according to the I^2^ test. The publication bias test was significant for both Egger′s test (p < 0.001) and Begg′s test (p = 0.017). The Duval and Tweedie trim‐and‐fill analysis did not identify any missing studies, indicating that the adjusted estimate was consistent with the original finding and unaffected by substantial publication bias. Regarding Pro‐BNP, the findings from the only study that assessed proBNP showed a significant increase in proBNP amongst patients compared to healthy controls [23].
Moderators of Heterogeneity
3.2
The leave‐one‐out sensitivity analyses were conducted to assess the influence of individual studies on the pooled effect estimates. For NT‐proBNP, the results showed that all re‐analyses, where each study was removed one at a time, yielded a statistically significant pooled effect estimate (p < 0.001), indicating that the effect size from each individual study was always consistent and did not cause excessive change to the pooled estimates. Furthermore, meta‐regression analyses were conducted to analyze whether continuous variables (number of patients and publication year) affected the heterogeneity in the meta‐analysis. The results showed that neither number of patients (r = −0.004, p = 0.646) nor publication year (r = −0.032, p = 0.650) had a significant moderating effect on the outcome.
Regarding BNP, the leave‐one‐out sensitivity analysis showed that excluding each study individually did not substantially alter the overall statistical significance. However, it was noteworthy that removing the study conducted by Kremastinos et al. lead to in a much lower but still significant pooled estimate (SMD = 1.336, p = 0.003). The meta‐regression analyses showed that the outcome was affected by the number of patients enrolled in studies. Specifically, studies with larger sample sizes may have slightly larger effect sizes compared to studies with smaller sample sizes. However, this correlation was weak (r = 0.088, p < 0.001), indicating that the practical impact of sample size on the outcome may be small. On the other hands, the outcome was not significantly affected by publication year (r = −0.207, p = 0.063).
Associations Between B‐Type Natriuretic Peptides and Various Biomarkers
3.3
Multiple investigations have evaluated the association of B‐type natriuretic peptides with a broad range of markers of cardiac function and other biomarkers in beta‐thalassemia patients (Table 2). Some of the included studies evaluated diastolic function by measuring mitral valve inflow velocities (E and A) and mitral annular tissue velocities (E′ and A′) during early and late diastole. The most commonly identified factors were serum ferritin levels, patients age, and diastolic dysfunction based on the E/E′ ratio. Other echocardiographic parameters, like the E/A ratio, systolic wave velocity (S′), and deceleration time, also demonstrated significant correlations with B‐type natriuretic peptides in few studies. Conversely, several studies reported no significant association between B‐type natriuretic peptides and other variables such as cardiac MRI‐T2. Interestingly, some research assessed the diagnostic utility of B‐type natriuretic peptides by identifying cut‐off values that can accurately detect diastolic dysfunction based on E/E′ ratio. Despite considerable variation across studies, all of these cut‐off values showed high levels of sensitivity and specificity according to the ROC analyses (Table 2).
Regarding meta‐analysis, few studies reported sufficient data for conducting meta‐analyses on correlations between NT‐proBNP and patients age, serum ferritin levels, E/E′ ratio, and cardiac MRI‐T2. An even smaller number of studies reported sufficient data for analyzing BNP correlations with serum ferritin levels.
The meta‐analyses results showed that NT‐proBNP was significantly correlated with serum ferritin levels (r = 0.471, 95% CI: 0.134–0.808; p = 0.006), E/E′ ratio (r = 0.528, 95% CI: 0.304–0.752; p < 0.001), and patients age (r = 0.259, 95% CI: 0.081–0.437; p = 0.004). However, NT‐proBNP was not significantly correlated with cardiac MRI‐T2 (r = ‐0.231, 95% CI: −0.747–0.285; p = 0.380). For BNP, the analysis revealed a significant correlation with serum ferritin levels (r = 0.347, 95% CI: 0.066–0.628; p = 0.015) (Additional file 2, Figure S1‐S5). Publication bias tests were not significant for most of these analyses (Table 3).
Discussion
4
This systemic review assessed the differences in B‐type natriuretic peptide levels between beta‐thalassemia major patients and healthy individuals and evaluated correlations between B‐type natriuretic peptide and various biomarkers. Our review found that BNP and NT‐proBNP are significantly elevated in beta‐thalassemia major patients compared to healthy individuals, with SMD of 1.37 for NT‐proBNP and SMD of 1.94 for BNP. These very high levels of both natriuretic peptides indicate that patients with beta‐thalassemia major experience considerably elevated cardiac stress and volume overload compared to healthy individuals, making these markers important indicators of cardiac dysfunction in this population. It is noteworthy that these markers were measured even in the absence of overt heart failure in all of the studies reviewed, suggesting subclinical cardiac dysfunction.
The analysis showed significant correlations between NT‐proBNP and other markers of cardiac dysfunction in beta‐thalassemia patients including serum ferritin and the E/E′ ratio, a marker of diastolic dysfunction. The pathophysiology underlying these associations is likely multifactorial. Chronic anemia and increased cardiac output leads to sustained myocardial stress which leads to ventricular remodeling and increased natriuretic peptide levels. Oxidative stress and iron overload, common in beta‐thalassemia, leads to myocardial fibrosis and diastolic dysfunction which may explain the correlations between NT‐proBNP and E/E′ ratio [24, 47].
The correlation with serum ferritin suggest a complex relationship between chronic transfusion related iron deposition and myocardial dysfunction. Interestingly, we found no significant correlation between NT‐proBNP and cardiac MRI‐T2, which measures myocardial iron content. This suggests that these natriuretic peptides are reflecting functional impairment, like diastolic dysfunction, rather than the amount of myocardial iron, which can be captured by MRI‐T2 [36]. Moreover, the discordance between NT‐proBNP and cardiac MRI‐T2 suggests that iron deposition is a necessary but not sufficient condition for cardiac dysfunction and functional deterioration may result from a combination of iron toxicity, inflammation and endothelial dysfunction [48].
Prolonged exposure to these stressors can lead to myocardial fibrosis, impaired relaxation and increased left ventricular filling pressures [24]. The correlations between NT‐proBNP levels and diastolic dysfunction shows that cardiac involvement in beta‐thalassemia is likely insidious. Therefore, these markers play a key role in assessing early cardiac involvement in beta‐thalassemia patients and it can be an early warning sign of myocardial stress, allowing for intervention before irreversible damage occur.
Additionally, some of the included studies identified diagnostic cut‐off values for BNP and NT‐proBNP that were highly accurate in ruling out diastolic dysfunction. The reported thresholds for diagnosing diastolic dysfunction in beta‐thalassemia patients showed considerable variation across studies. Other studies have investigated cut‐off values for NT‐proBNP in detecting early or subclinical cardiac dysfunction in the general population, as well as in other high‐risk populations for heart failure [49, 50, 51]. When comparing these values to beta‐thalassemia patients, our systematic review identified significantly lower NT‐proBNP cut‐off values for diastolic dysfunction. This finding has important clinical implications, indicating the need for more cautious cardiac monitoring and potentially earlier intervention in beta‐thalassemia patients. However, establishment of reliable cut‐offs for this patients population remains a knowledge gap that should be addressed in future research.
Defining precise cut‐off values would makes these biomarkers even more useful as screening tools to reduce the need for expensive and less accessible imaging. By adding these biomarkers to clinical algorithms, we can move towards a more proactive and individualized approach to managing cardiac complications in beta‐thalassemia. Future studies should look at the longitudinal trend of these biomarkers in beta‐thalassemia patients and refine the cut‐offs for risk stratification. Also, investigating the interplay between these peptides and biomarkers of fibrosis and inflammation will also help us understand the pathophysiology of cardiac dysfunction in this patients population.
However, this review have some limitations. The high heterogeneity across studies likely due to different patient populations, study designs and methods may affect generalizability and should be taken into consideration when interpreting the pooled estimates. The inclusion of studies with both pediatric and adult populations may contributed to the observed heterogeneity. The inconsistency in reporting all clinically relevant outcomes across studies limited conducting further meta‐analyses on other variables relevant to the problem, especially the other markers of cardiac dysfunction. Future studies should aim for more methodological consistency and bigger sample sizes to strengthen the findings. By addressing these gaps, we can further refine the clinical use of natriuretic peptides and improve cardiac monitoring and outcomes in beta‐thalassemia patients. Finally, excluding non‐English studies could limit the breadth of conclusions.
Conclusion
5
This systematic review provides evidence that beta‐thalassemia major is associated with increased levels of B‐type natriuretic peptides, which reflects their increased cardiovascular risk. The significantly elevated levels of these molecules and their identified correlations emphasize clinical utility of them as markers of early myocardial stress and subclinical heart disease in beta‐thalassemia. In addition, the findings emphasize the need for regular assessment of in clinical practice to risk stratify patients and identify those at high risk for adverse cardiovascular outcomes, and to guide interventions to improve their outcomes and survival.
Author Contributions
Mohamed S K Salih: conceptualization, methodology, writing – original draft, writing – review and editing, project administration. Amna H Mohamed: writing – original draft, writing – review and editing, investigation, data curation. Elsara M A Mirghani: investigation, data curation. Mohammed Y K Makki: data curation, investigation. Ola A M Ahmed: data curation, investigation. Esraa T S Mohammed: data curation, investigation. Hana H Mohamed: writing – review and editing, writing – original draft. Nada Omar: investigation, data curation. Esraa M A Garalnabi: investigation, data curation. Sagad O O Mohamed: conceptualization, writing – original draft, writing – review and editing, formal analysis, supervision, investigation, methodology, data curation, visualization, project administration.
Conflicts of Interest
The authors declare that they have no competing interests.
Transparency Statement
1
The lead author Sagad O. O. Mohamed affirms that this manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
Supporting information
Additional file 1.
Additional file 2.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1A. T. Taher , K. M. Musallam , and M. D. Cappellini , “β‐Thalassemias.” in N Engl J Med, eds. D. L. Longo , 2021 Feb 25. 384, 727–743. 8.33626255 10.1056/NEJ Mra 2021838 · doi ↗ · pubmed ↗
- 2M. Sanchez‐Villalobos , M. Blanquer , J. M. Moraleda , E. J. Salido , and A. B. Perez‐Oliva , “New Insights Into Pathophysiology of β‐Thalassemia,” Frontiers in Medicine 9 (April 2022): 880752.35492364 10.3389/fmed.2022.880752 PMC 9041707 · doi ↗ · pubmed ↗
- 3R. Origa , “β‐Thalassemia,” Genetics in Medicine 19, no. 6 (June 2017): 609–619.27811859 10.1038/gim.2016.173 · doi ↗ · pubmed ↗
- 4Y. M. Lee , S. Y. Chuang , S. F. Wang , Y. T. Lin , and Y. M. A. Chen , “Epidemiology of Human Herpesvirus Type 8 and Parvovirus B 19 Infections and Their Association With HIV‐1 Among Men Who Have Sex With Men and Injection Drug Users in Taiwan,” Journal of Microbiology, Immunology and Infection 47, no. 3 (June 2014): 233–238.10.1016/j.jmii.2013.01.00623465711 · doi ↗ · pubmed ↗
- 5C. Hershko , “Pathogenesis and Management of Iron Toxicity in Thalassemia,” Annals of the New York Academy of Sciences 1202, no. 1 (August 2010): 1–9.20712765 10.1111/j.1749-6632.2010.05544.x · doi ↗ · pubmed ↗
- 6F. Koohi , T. Kazemi , and E. Miri‐Moghaddam , “Cardiac Complications and Iron Overload in Beta Thalassemia Major Patients—A Systematic Review and Meta‐Analysis,” Annals of Hematology 98, no. 6 (June 2019): 1323–1331.30729283 10.1007/s 00277-019-03618-w · doi ↗ · pubmed ↗
- 7S. Lekawanvijit and N. Chattipakorn , “Iron Overload Thalassemic Cardiomyopathy: Iron Status Assessment and Mechanisms of Mechanical and Electrical Disturbance Due to Iron Toxicity,” Canadian Journal of Cardiology 25, no. 4 (2009): 213–218.19340344 10.1016/s 0828-282x(09)70064-9PMC 2706758 · doi ↗ · pubmed ↗
- 8A. Kautsar , N. Advani , and M. Andriastuti , “N‐Terminal‐Pro‐B‐Type Natriuretic Peptide Levels and Cardiac Hemosiderosis in Adolescent β‐thalassemia Major Patients,” Annals of Pediatric Cardiology 12, no. 1 (2019): 32.30745767 10.4103/apc.APC_49_18PMC 6343373 · doi ↗ · pubmed ↗