The Rising Menace: Carbapenem-Resistant Klebsiella pneumoniae in a Tertiary Care Center and Co-dominance of blaNDM, blaOXA-48 Along With the Emergence of blaVIM
Fatima Muneer, Nikhil Raj, Anupam Das, Vikramjeet Singh, Manodeep Sen, Jyotsna Agarwal

TL;DR
This study examines the spread of antibiotic-resistant Klebsiella pneumoniae in a hospital, finding that resistance genes like blaNDM and blaOXA-48 are common and pose a serious threat.
Contribution
The study reports the co-dominance of blaNDM and blaOXA-48 genes and the emergence of blaVIM in CR-Kp isolates in a hospital setting.
Findings
64.52% of Klebsiella pneumoniae isolates were carbapenem-resistant.
blaNDM was detected in 100% of tested CR-Kp isolates, and blaOXA-48 in 65%.
CR-Kp isolates showed high resistance to fluoroquinolones, cephalosporins, and aminoglycosides.
Abstract
Background and objective Carbapenem-resistant Klebsiella pneumoniae (CR-Kp) has become a significant cause of hospital-acquired infections, with significant implications for patient outcomes due to limited treatment options and high mortality rates. This study aimed to determine the prevalence, phenotypic resistance patterns, and molecular characteristics of CR-Kp isolates. Methods This was a cross-sectional study conducted for a period of one year. A total of 186 non-duplicate Klebsiella pneumoniae (K. pneumoniae) isolates from various samples were subjected to antibiotic susceptibility testing. Phenotypic detection of carbapenemase production was performed using the modified Hodge test (MHT), modified carbapenem inactivation method (mCIM), and combined disc testing (CDT). Genotypic analysis using PCR was performed on 20 representative CR-Kp isolates to detect blaNDM, blaKPC,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
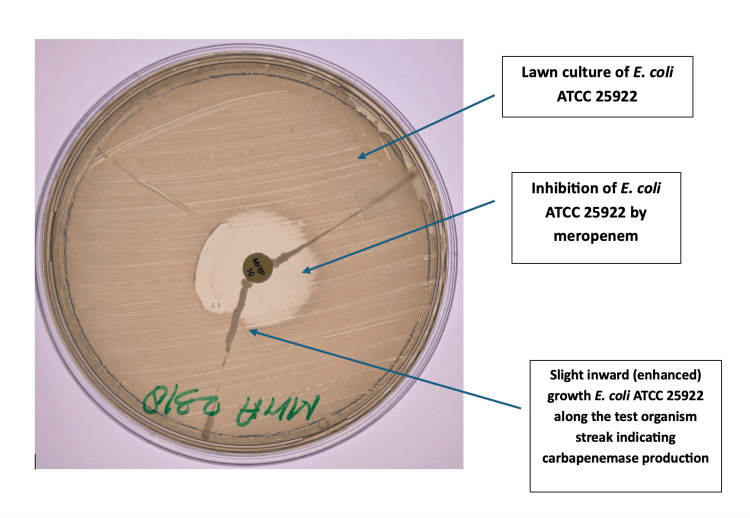 Figure 1
Figure 1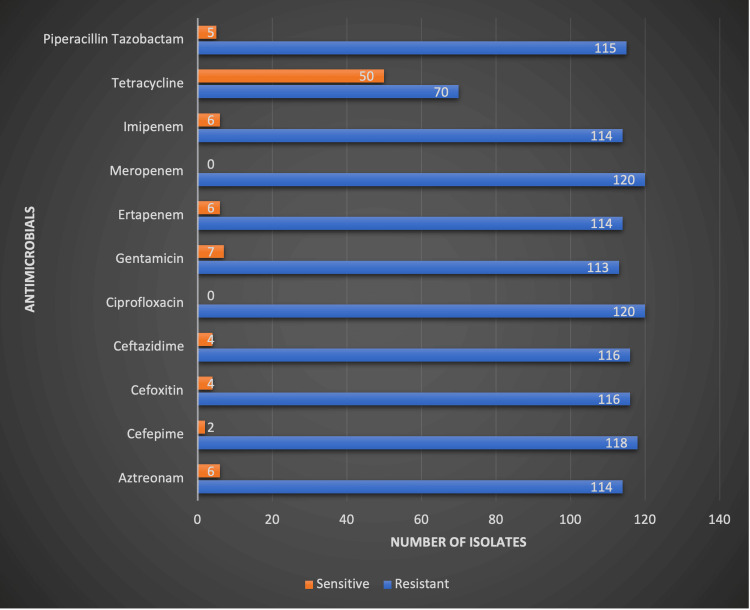 Figure 2
Figure 2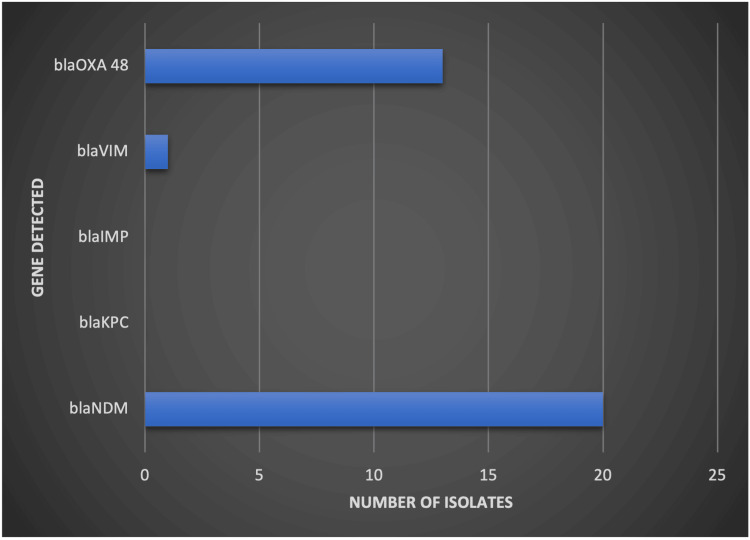 Figure 3
Figure 3| Age group, years | Number of patients | Percentage | ||
| Male | Female | Total | ||
| 0-20 | 9 | 8 | 17 | 9.13% |
| 21-40 | 21 | 34 | 55 | 29.56% |
| 41-60 | 42 | 30 | 72 | 38.71% |
| 61-80 | 29 | 12 | 41 | 22.04% |
| 81-90 | 1 | 0 | 1 | 0.53% |
| TOTAL | 102 | 84 | 186 | 100% |
| Sample | No. of | No. of carbapenem-resistant | No. of carbapenem-sensitive | Chi-square test | P-value |
| Sputum and BAL | 46 (24.7) | 36 (30.0) | 10 (15.1) | 3.79 | 0.051 |
| Blood | 20 (10.8) | 17 (14.2) | 03 (4.5) | 3.66 | 0.055 |
| Urine | 86 (46.2) | 44 (36.7) | 42 (63.6) | 6.69 | 0.009 |
| Body fluids | 04 (2.2) | 02 (1.7) | 02 (3.0) | 0.36 | 0.54 |
| CVP | 07 (3.8) | 02 (1.7) | 05 (7.6) | 3.95 | 0.046 |
| Pus | 23 (12.4) | 19 (15.8) | 04 (6.1) | 3.28 | 0.069 |
| Carbapenemase detection method | Carbapenemase detected, n (%) | Carbapenemase not detected, n (%) |
| MHT | 76 (40.86%) | 110 |
| mCIM test | 91 (48.92%) | 95 |
| CDT | 114 (61.29%) | 72 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntibiotic Resistance in Bacteria · Antibiotic Use and Resistance · Nephrotoxicity and Medicinal Plants
Introduction
Klebsiella pneumoniae (K. pneumoniae) is a major infectious agent implicated in both community-based and hospital-associated infections. In healthy people, K. pneumoniae is a normal component of the gastrointestinal microbiota; nevertheless, in some circumstances, especially in immunocompromised people or those with underlying medical disorders, it can become harmful [1,2]. Its ability to acquire multidrug resistance, particularly to carbapenems, has made it a significant public health concern. The main cause of K. pneumoniae pathogenicity includes certain virulence factors.. Lipopolysaccharide (LPS) on the bacterial cell wall plays a key role in immune evasion and inflammatory response modulation. Siderophores, iron-binding molecules, enable K. pneumoniae to access vital nutrients like iron from the host environment, aiding in its survival and proliferation [3,4].
The resistance of carbapenems is due to the expression of a carbapenemase enzyme, efflux pump, or loss of porin channels [5]. Carbapenem resistance in* K. pneumoniae *is primarily mediated through carbapenemase enzymes such as KPC, NDM, OXA-48, VIM, and IMP, leading to high mortality rates in infected patients. Multidrug-resistant (MDR) *K. pneumoniae *is a concerning matter in Indian hospitals due to the potential transfer of resistance to different pathogens [6]. The distressing pattern of rising resistance to carbapenems poses a major public health threat [7]. The abrupt emergence and subsequent outbreaks of NDM-1 likely serve as the primary example of the increased prominence of MBLs as a disease cause [8]. This study aimed to determine the prevalence, phenotypic resistance patterns, and molecular characteristics of Carbapenem-resistant K. pneumoniae (CR-Kp) isolates.
Materials and methods
This was a cross-sectional study conducted over a period of one year. A total of 186 K. pneumoniae isolates were collected from urine, blood, respiratory samples, pus, and other body fluids of patients admitted in various wards, including the ICU and OPD. Blood culture bottles were incubated in the BacT/ALERT system and, once flagged positive, were inoculated on blood agar and MacConkey agar, followed by Gram staining of the isolates. Simultaneously, clinical samples were directly inoculated on MacConkey agar and blood agar and incubated aerobically at 37°C for 24-48 hours. Matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS) was used to detect bacterial growth.
Antimicrobial susceptibility testing (AST) of *K. pneumoniae *isolates was performed using the Kirby-Bauer disc diffusion method on Mueller-Hinton agar plates. Isolates resistant to any carbapenem (ertapenem, imipenem, or meropenem) as per the latest Clinical and Laboratory Standards Institute (CLSI) guidelines were considered carbapenem-resistant and included for further analysis.
Metallo-β-lactamase (MBL) production was screened using the imipenem (10 μg)-EDTA (750 μg) combined disk method. Imipenem-only and imipenem-EDTA discs were positioned on the surface of a lawn culture of the test organism that had been produced on Mueller-Hinton agar. The difference in zone diameter of ≥7 mm between the imipenem-only and the imipenem + EDTA discs after 16-18 hours of incubation at 37°C denotes MBL production. The modified Hodge test (MHT) was used to further assess carbapenemase activity in accordance with CLSI M100-S19 (2009) recommendations. A meropenem (10 μg) disc was positioned in the center of a Mueller-Hinton agar lawn culture of Escherichia coli (*E. coli) *ATCC 25922, and the test strain was streaked from the disc's edge to the plate margin. A cloverleaf-like indentation of E. coli growth during an overnight incubation at 35 ± 2 °C showed a successful outcome, as shown in Figure 1.
Modified Hodge Test (MHT)-positive Klebsiella pneumoniae isolateA lawn culture of Escherichia coli (E. coli) ATCC 25922 is streaked on Mueller–Hinton agar with a central meropenem (10 µg) disc. The test isolate of Klebsiella pneumoniae is streaked from the edge of the disc to the periphery. The characteristic cloverleaf-like indentation of E. coli growth along the streak indicates a positive MHT, confirming carbapenemase production
The modified carbapenem inactivation method (mCIM) was performed by incubating a 10-µg meropenem disc in tryptic soy broth inoculated with the test strain for two to three hours at 37 °C. The disc was then transferred onto a Mueller-Hinton agar plate previously inoculated with E. coli ATCC 25922 (0.5 McFarland). After overnight incubation at 37°C, a zone of inhibition ≤15 mm indicated carbapenemase production; ≥19 mm suggested a negative result, while 16-18 mm or zones with colonies were considered indeterminate.
Genotypic detection of carbapenem resistance genes was performed using the TRUPCR Total Nucleic Acid Extraction Kit for DNA isolation from bacterial cultures, followed by real-time PCR with the TRUPCR Carbapenem Resistance Detection Kit. This assay qualitatively detected and differentiated key carbapenemase genes (bla_KPC_, bla_NDM_, bla_VIM_, bla_OXA-48_, and bla_IMP_) using extracted nucleic acid from BHI broth-inoculated isolates.
Statistical analysis
Descriptive and inferential techniques were used in the statistical analysis. For the sample distribution, demographic factors, and patterns of antibiotic susceptibility, frequencies and percentages were computed. The relationship between sample type and carbapenem resistance was evaluated using the chi-square test; a p-value of less than 0.05 was deemed statistically significant.
Results
Out of 186 K. pneumoniae isolates tested, 120 (64.52%) were found to be carbapenem-resistant based on the Kirby-Bauer disc diffusion method. The majority of infections were seen in male patients (55%) compared to females (45%). The age group of 41-60 years had the highest prevalence of CR-Kp at 38.71%, followed by the age group of 21-40 years at 29.56% (Table 1).
The distribution of K. pneumoniae isolates among clinical specimens showed the highest number from urine samples (n = 86), of which 44 were carbapenem-resistant. Sputum and bronchoalveolar lavage (BAL) samples contributed 46 isolates with a high resistance rate (36/46), followed by blood (17/20). Statistical analysis revealed a significant association between sample type and carbapenem resistance in urine (p = 0.009) and central venous pressure (CVP) tip cultures (p = 0.046) (Table 2).
Among the phenotypic methods used for carbapenemase detection in CR-Kp isolates, the combined disk test (CDT) showed the highest sensitivity with 114 (61.29%) positive results, followed by the mCIM in 91 isolates (48.92%), and MHT in 76 isolates (40.86%) (Table 3).
Antibiotic susceptibility testing of the 120 CR-Kp isolates revealed high resistance rates across most antibiotics tested. All isolates were resistant to meropenem and ciprofloxacin. High levels of resistance were also seen with ceftazidime (96.7%), cefotaxime (96.7%), and aztreonam (95%). Only tetracycline showed moderate susceptibility, with 41.7% (50/120) of isolates being sensitive. The complete resistance profile is shown in Figure 2.
Antimicrobial susceptibility pattern of carbapenem-resistant Klebsiella pneumoniae isolates
Genotypic detection was performed on 20 CR-Kp isolates using real-time PCR. All 20 isolates (100%) were positive for the bla_NDM_ gene, while bla OXA-48 was detected in 13 isolates (65%). Additionally, bla_VIM_ was found in only one isolate (5%), whereas bla_KPC and *bla_IMP *were not detected in any of the tested isolates. The distribution of these genes is presented in Figure 3.
Distribution of carbapenemase genes among carbapenem-resistant Klebsiella pneumoniae isolates
Discussion
The results of this study demonstrate a high prevalence of carbapenem resistance (120/186; 64.52%) among *K. pneumoniae *isolates, highlighting a significant concern for nosocomial infections and antimicrobial resistance management. This finding is consistent with regional data, where a systematic review reported the highest prevalence of CR-Kp in South Asia at 66.04%, with India specifically reporting 67.62% [9].
Indrajith et al. reported carabapenem resistance in 58% of K. pneumoniae isolates [10]. The observed resistance rate also aligns with recent studies from India, the Middle East, and Southern Europe, where co-production of bla_OXA-48_ and bla_NDM_ has been frequently reported. These results highlight the critical necessity for strict infection control protocols and strong antibiotic stewardship in order to stop the development of resistant bacteria in healthcare environments. The overall prevalence of carbapenem resistance in Enterobacteriaceae was found to be 29.35% in a study by Srivastava et al. [11].
In this study, sputum and BAL samples (46 isolates) showed a high carbapenem resistance rate of 78.2% (36 CR-Kp isolates), indicating a significant role of CR-Kp in ventilator-associated pneumonia (VAP) and respiratory tract infections (RTIs). Bloodstream infections (BSIs) demonstrated the highest resistance, with 85% (17 out of 20 cases) of isolates being CR-Kp, highlighting their impact in sepsis at our institute. Demographic data showed that males (55%) had a higher infection rate than females (45%), consistent with previous findings on* K. pneumoniae *infections. Abbasi et al. have similarly reported that 67.7% of cases were males and 32.2% were females [12]. In our study, phenotypic detection of carbapenemase production was performed using MHT, CDT, and mCIM, which detected carbapenemase activity in 76 (40.86%), 114 (61.29%), and 91 (48.92%) isolates, respectively. Similar observations were reported in the study by Manandhar et al., where CDT was described as the most sensitive method for MBL detection [13].
Our PCR analysis revealed that all tested CR-Kp isolates (n=20) harbored the bla_NDM _gene (100%), with 65% also carrying bla_OXA-48_, and one isolate (5%) harboring bla_VIM_, while bla_IMP_ was not detected. These findings are consistent with previous Indian studies identifying bla_NDM_ and bla_OXA-48 as predominant carbapenemase genes [14-16]. A study in India reported a similar dominance of* bla_NDM,* though bla_OXA-48_ was less prevalent at that time [13]. Nordmann et al. have highlighted the global dissemination of *bla_NDM_ *and bla_OXA-48_, particularly in nosocomial outbreaks [16]. The detection of bla_VIM_, although rare, signals the emergence of Verona integron-encoded metallo-β-lactamase, known for broad β-lactam hydrolysis [16]. A prior study from our center reported NDM in 100% of carbapenem-resistant urinary isolates, followed by KPC (75%) and OXA-48 (60%), with no VIM detected [14]. Since bla_NDM _and bla_OXA-48_ are linked to substantial drug resistance (XDR) and strong transmission potential, their confluence in 65% of isolates is especially concerning.
NDM-positive K. pneumoniae is globally recognized for high-level resistance and widespread dissemination [9,10]. While bla_OXA-48_ confers carbapenem resistance, it often retains susceptibility to cefepime and aztreonam, complicating treatment [17]. The absence of bla_IMP_, typically reported in East Asia and Europe, further defines the regional resistance gene profile [18]. In a study by Mokhtari et al., the percentage of isolates with the carbapenemase expressing the *bla_ OXA-48_ *and bla _NDM-1 _genes was 96.7% and 66.7%, respectively [19]. These results align with global data, reinforcing the challenge of managing CR-Kp infections and the critical importance of robust surveillance and stewardship strategies.
Limitations
This study was limited by genotypic testing of only a small subset of isolates, restricting full representation of resistance mechanisms. Being a single-center cross-sectional study, the results may not be generalizable. In addition, clinical outcomes were not evaluated, preventing a correlation between resistance patterns and patient prognosis.
Conclusions
The high prevalence and antibiotic resistance of *Klebsiella pneumoniae *make it a serious challenge to hospital infection management. Effective surveillance, antimicrobial stewardship programs, and alternative treatment strategies are crucial to managing CR-Kp infections and preventing further dissemination.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Klebsiella pneumoniae capsular polysaccharide: mechanism in regulation of synthesis, virulence, and pathogenicity Virulence Xu L Li J Wu W Wu X Ren J 24395091520243966872410.1080/21505594.2024.2439509 PMC 11649230 · doi ↗ · pubmed ↗
- 2Klebsiella pneumoniae: going on the offense with a strong defense Microbiol Mol Biol Rev Paczosa MK Mecsas J 6296618020162730757910.1128/MMBR.00078-15PMC 4981674 · doi ↗ · pubmed ↗
- 3A review: virulence factors of Klebsiella pneumonia as emerging infection on the food chain Vet World Riwu KH Effendi MH Rantam FA Khairullah AR Widodo A 217221791520223634105910.14202/vetworld.2022.2172-2179 PMC 9631384 · doi ↗ · pubmed ↗
- 4Clinical epidemiology, risk factors, and control strategies of Klebsiella pneumoniae infection Front Microbiol Chang D Sharma L Dela Cruz CS Zhang D 7506621220213499258310.3389/fmicb.2021.750662 PMC 8724557 · doi ↗ · pubmed ↗
- 5Phenotypic and genotypic detection of carbapenemase production among Gram-negative bacteria isolated from hospital-acquired infections Saudi Med J Vamsi SK Moorthy RS Hemiliamma MN Chandra Reddy RB Chanderakant DJ Sirikonda S 2362434320223525649010.15537/smj.2022.43.3.20210809 PMC 9280532 · doi ↗ · pubmed ↗
- 6Emerging carbapenem resistance among nosocomial isolates of Klebsiella pneumoniae in South India Int J Pharma Bio Sci Parveen RM Harish BN Parija SC 11112010 https://www.ijpbs.net/abstract.php?article=NDU 4
- 7Carbapenems: past, present, and future Antimicrob Agents Chemother Papp-Wallace KM Endimiani A Taracila MA Bonomo RA 494349605520112185993810.1128/AAC.00296-11PMC 3195018 · doi ↗ · pubmed ↗
- 8Strategies to name metallo-β-lactamases and number their amino acid residues Antibiotics (Basel) Oelschlaeger P Kaadan H Dhungana R 161812202310.3390/antibiotics 12121746 PMC 1074099438136780 · doi ↗ · pubmed ↗