Assessment of asymptomatic Leishmania infection in people living with HIV: a long-term follow-up study in Northeastern Brazil
Matheus Henrique Gonçalves Aguiar, Diego Lins Guedes, Walter Lins Barbosa Júnior, Elis Dionísio da Silva, Gilberto Silva Nunes Bezerra, Cristine Vieira Bonfim, Amanda Virginia Batista Vieira, Bruna Eduarda Freitas Monteiro, Roberta dos Santos Souza, Lucyo Flávio Bezerra Diniz

TL;DR
This study tracks HIV patients in Brazil over six years to assess the risk of developing leishmaniasis and highlights the importance of long-term monitoring.
Contribution
The study provides long-term follow-up data on asymptomatic Leishmania-HIV coinfected individuals, revealing higher progression to visceral leishmaniasis.
Findings
Leishmania-HIV coinfected individuals were 10.4 times more likely to develop visceral leishmaniasis than non-coinfected HIV patients.
Five coinfected patients remained positive for VL in 2023, and two HIV patients seroconverted to VL.
Relapse and mortality rates were higher in the Leishmania-HIV coinfected group.
Abstract
In people living with HIV (PLWH), surveillance for Leishmania infection is crucial for identify those at risk of developing visceral leishmaniasis (VL). Leishmania-HIV coinfection worsens patient outcomes and increases mortality and relapse rates. We conducted a prospective study (2017–2023) in Northeast Brazil to assess the long-term outcomes of asymptomatic Leishmania-HIV coinfected outpatients and Leishmania-negative PLWH. Participants were drawn from a cross-sectional study performed in 2017, which identified both Leishmania-HIV coinfected and Leishmania-negative PLWH. Epidemiological, clinical, and laboratory data were collected from medical records (2017–2023). In 2023, these individuals were retested for Leishmania using serological tests and conventional polymerase chain reaction (PCR). Categorical variables were compared using the chi-square test, and non-parametric tests were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
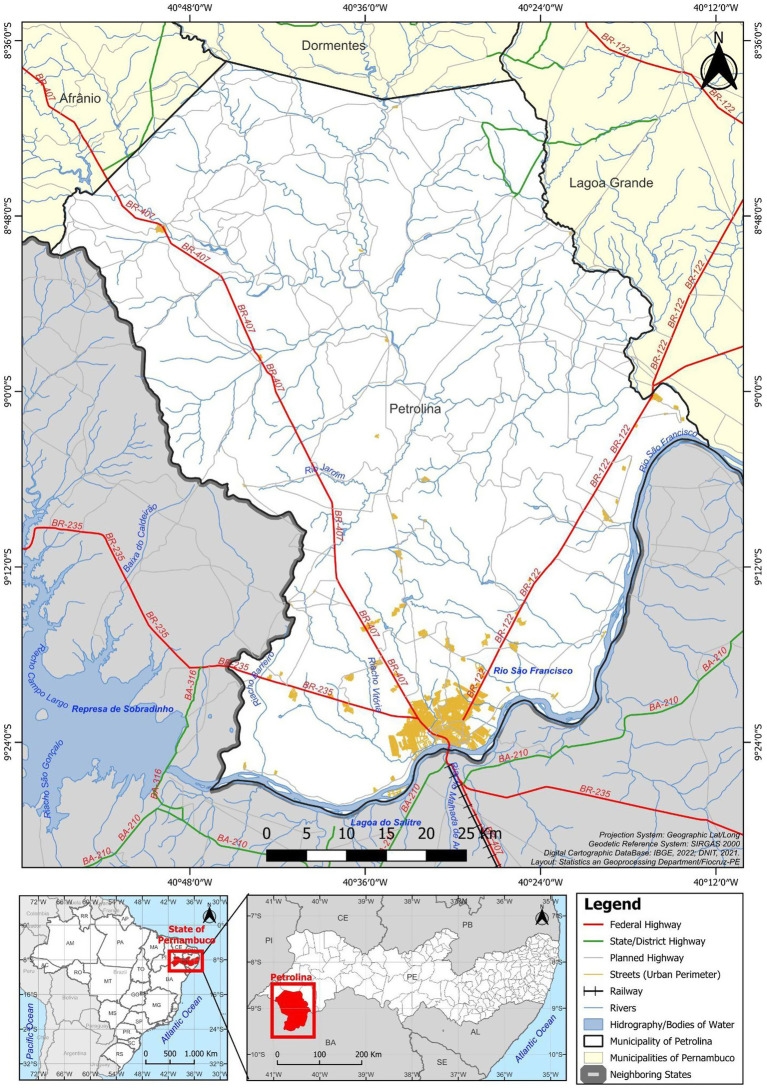 Figure 1
Figure 1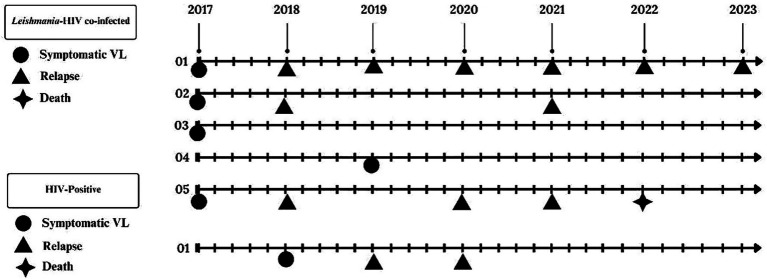 Figure 2
Figure 2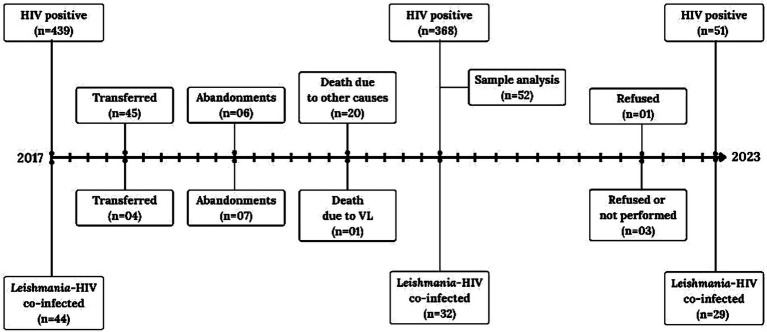 Figure 3
Figure 3| VL tests | 2017 | 2018 | 2019 | 2020 | 2021 | 2022 | 2023 |
|---|---|---|---|---|---|---|---|
| Bone marrow aspirate | 3 | 4 | 1 | 2 | 3 | 1 | 1 |
| ELISA-rK39 | 12 | – | – | – | – | – | 2 |
| rK39-ICT | 5 | – | – | – | – | – | 0 |
| DAT | 17 | – | – | – | – | – | 0 |
| PCR kDNA | 11 | – | – | – | – | – | 0 |
| DAT and rK39 ICT | 1 | – | – | – | – | – | 0 |
| ELISA-rK39 and DAT | 0 | – | – | – | – | – | 1 |
| ELISA-rK39 + DAT + rK39-ICT | 0 | – | – | – | – | – | 1 |
| ELISA-rK39 + DAT + rK39-ICT + PCR kDNA | 0 | – | – | – | – | – | 1 |
| Total (at last one positive test) |
|
| |||||
| Variables | PLWH | OR | |||||
|---|---|---|---|---|---|---|---|
| % | % | OR | 95% CI | ||||
| Gender | |||||||
| Male | 33 | 64.7 | 15 | 51.7 | |||
| Female | 18 | 35.3 | 14 | 48.3 | 1.71 | 0.68–4.33 | 0.268 |
| Age (years) | |||||||
| 18–28 | 3 | 5.9 | 2 | 6.9 | |||
| 29–39 | 12 | 23.5 | 6 | 20.7 | 0.75 | 0.10–5.77 | 0.794 |
| 40–49 | 7 | 13.7 | 8 | 27.6 | 2.29 | 0.22–13.41 | 0.652 |
| >50 or more | 29 | 56.9 | 13 | 44.8 | 0.39 | 0.10–4.52 | 0.695 |
| Years of schooling | |||||||
| 0–8 | 22 | 43.1 | 14 | 48.3 | |||
| 9–11 | 4 | 7.8 | 3 | 10.3 | 1.18 | 0.23–6.08 | 0.846 |
| 12 or more | 25 | 49.0 | 12 | 41.4 | 0.64 | 0.29–1.97 | 0.576 |
| Area | |||||||
| Urban | 48 | 94.1 | 20 | 69.0 | |||
| Rural | 3 | 5.9 | 9 | 31.0 | 7.20 | 1.76–29.40 | 0.004 |
| Dogs at home | |||||||
| No | 29 | 56.9 | 14 | 48.3 | |||
| Yes | 22 | 43.1 | 15 | 51.7 | 1.41 | 0.57–3.53 | 0.471 |
| VL in patients’ household | |||||||
| No | 50 | 98 | 28 | 96.6 | |||
| Yes | 1 | 2.0 | 1 | 3.4 | 1.79 | 0.11–29.67 | 0.725 |
| VL in patients’ neighborhood | |||||||
| No | 44 | 86.3 | 27 | 93.1 | |||
| Yes | 7 | 13.7 | 2 | 6.9 | 0.47 | 0.09–2.41 | 0.388 |
| Resident in an endemic area (last 2 years) | |||||||
| No | 12 | 23.5 | 6 | 20.7 | |||
| Yes | 39 | 76.5 | 23 | 79.3 | 1.18 | 0.39–3.57 | 0.788 |
| Variables | PLWH | OR | |||||
|---|---|---|---|---|---|---|---|
| % | % | OR | 95% CI | ||||
| Presence of fever | |||||||
| No | 43 | 84.3 | 24 | 82.8 | |||
| Yes | 8 | 15.7 | 5 | 17.2 | 1.12 | 0.33–3.81 | 0.850 |
| Presence of hepatomegaly | |||||||
| No | 43 | 84.3 | 27 | 93.1 | |||
| Yes | 2 | 3.9 | 2 | 6.9 | 1.59 | 0.21–11.98 | 0.676 |
| Presence of splenomegaly | |||||||
| No | 43 | 84.3 | 27 | 93.1 | |||
| Yes | – | – | 2 | 6.9 | – | – | – |
| Presence of hepatosplenomegaly | |||||||
| No | 43 | 84.3 | 27 | 93.1 | |||
| Yes | 2 | 3.9 | 2 | 6.9 | 1.59 | 0.21–11.98 | 0.676 |
| Presence of cough | |||||||
| No | 43 | 84.3 | 26 | 89.7 | |||
| Yes | 13 | 25.5 | 3 | 10.3 | 0.38 | 0.10–1.47 | 0.161 |
| Presence of diarrhea | |||||||
| No | 43 | 84.3 | 27 | 93.1 | |||
| Yes | 7 | 13.7 | 2 | 6.9 | 0.46 | 0.09–2.35 | 0.373 |
| Presence of dyspnea | |||||||
| No | 43 | 84.3 | 25 | 86.2 | |||
| Yes | 8 | 15.7 | 4 | 13.8 | 0.86 | 0.23–3.15 | 0.843 |
| Presence of bleeding | |||||||
| No | 43 | 84.3 | 24 | 82.8 | |||
| Yes | 6 | 11.8 | 5 | 17.2 | 1.49 | 0.41–5.41 | 0.550 |
| Presence of weight loss | |||||||
| No | 43 | 84.3 | 19 | 65.5 | |||
| Yes | 6 | 11.8 | 10 | 34.5 | 3.77 | 1.20–11.88 | 0.025 |
| Presence of mucous pale | |||||||
| No | 43 | 84.3 | 27 | 93.1 | |||
| Yes | 3 | 5.9 | 2 | 6.9 | 1.06 | 0.17–6.77 | 0.936 |
| Patients with Diabetes mellitus | |||||||
| No | 43 | 84.3 | 26 | 89.7 | |||
| Yes | 11 | 21.6 | 3 | 10.3 | 0.45 | 0.12–1.77 | 0.264 |
| Patients with hypertension | |||||||
| No | 43 | 84.3 | 24 | 82.8 | |||
| Yes | 15 | 29.4 | 5 | 17.2 | 0.60 | 0.19–1.85 | 0.387 |
| Patients with obesity | |||||||
| No | 43 | 84.3 | 27 | 93.1 | |||
| Yes | 1 | 2.0 | 2 | 6.9 | 3.19 | 0.28–36.85 | 0.405 |
| Patients with cardiovascular disease | |||||||
| No | 43 | 84.3 | 29 | 100.0 | |||
| Yes | 3 | 5.9 | – | – | – | – | – |
| Patients with neoplasm | |||||||
| No | 43 | 84.3 | 28 | 96.6 | |||
| Yes | 1 | 2.0 | 1 | 3.4 | 1.54 | 0.09–25.57 | 0.795 |
| Patients with respiratory disease | |||||||
| No | 43 | 84.3 | 27 | 93.1 | |||
| Yes | 3 | 5.9 | 2 | 6.9 | 1.06 | 0.17–6.77 | 0.936 |
| TCD4 + count (cells/mm3) | |||||||
| <200 | 5 | 9.8 | 6 | 20.7 | |||
| 200–349 | 9 | 17.6 | 4 | 13.8 | 0.37 | 0.07–1.97 | 0.279 |
| >350 | 37 | 72.5 | 19 | 65.5 | 0.43 | 0.12–1.59 | 0.223 |
| HIV viral load (copies/mL) | |||||||
| Undetectable (<50) | 39 | 76.5 | 21 | 72.4 | |||
| 50–100,000 | 9 | 17.6 | 6 | 20.7 | 1.24 | 0.39–3.95 | 0.721 |
| >100,000 | 3 | 5.9 | 2 | 6.9 | 1.24 | 0.19–8.00 | 0.819 |
| In use of ART | |||||||
| No | 3 | 5.9 | – | – | – | – | – |
| Yes | 48 | 94.1 | 29 | 100.0 | – | – | – |
| General Laboratory – Median (IQR) to the variables below | |||||||
| White blood cells (cells/mm3) | 5600 (4600–7010) | 5250 (4302.5–6407.5) | 0.360 | ||||
| Neutrophils | 3086 (2189.3–3860.5) | 3096 (2239–3634) | 0.931 | ||||
| Lymphocytes | 1999.5 (1722.8–2689.5) | 1875 (1388.5–2587) | 0.224 | ||||
| Hemoglobin (g/dL) | 13.6 (12.5–15.1) | 14.2 (13.2–14.7) | 0.361 | ||||
| Platelets (cells/mm3) | 237 (197.5–274.5) | 217.5 (176.5–269) | 0.187 | ||||
| HTC | 42.3 (37.5–46.1) | 41.8 (39.3–43.6) | 1.000 | ||||
| AST (U/L) | 26 (19.3–32.5) | 25 (22.8–37) | 0.413 | ||||
| ALT (U/L) | 24.5 (17.3–36.8) | 25.5 (18.5–36.3) | 0.632 | ||||
| Creatinine (mg/dL) | 0.9 (0.8–1.1) | 0.9 (0.7–1.1) | 0.762 | ||||
| Groups | Symptomatic infection | OR | 95% CI | ||||
|---|---|---|---|---|---|---|---|
| No | Yes | ||||||
| % | % | ||||||
| PLWH | 50 | 98.0 | 1 | 3.4 | |||
| 24 | 47.1 | 5 | 17.2 | 10.4 | 1.2–94.2 | 0.023 | |
- —Oswaldo Cruz Foundation10.13039/501100006507
- —Foundation for Scientific and Technological Development in Health
- —Conselho Nacional de Desenvolvimento Científico e Tecnológico10.13039/501100003593
- —Coordenação de Aperfeiçoamento de Pessoal de Nível Superior – Brasil
- —Fundação de Amparo à Ciência e Tecnologia do Estado de Pernambuco10.13039/501100006162
- —Oswaldo Cruz Foundation10.13039/501100006507
- —Sistema Único de Saúde (SUS): Ministry of Health, Health Departments of Pernambuco and the Municipality of Petrolina
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsResearch on Leishmaniasis Studies · Trypanosoma species research and implications
Introduction
1
Visceral leishmaniasis (VL) is a serious systemic disease caused by protozoa of the Leishmania donovani complex. In Brazil, the causative parasite is Leishmania infantum (1, 2). Typical symptoms of VL include recurrent fever, weight loss, hepatosplenomegaly, and pancytopenia (3, 4). Pederiva et al. (5) demonstrated that asymptomatic Leishmania infection is frequent in VL-endemic regions, particularly in developing countries such as Brazil and India.
People living with HIV (PLWH) in VL-endemic areas have an elevated risk of Leishmania infection compared with HIV-negative individuals (6–8). In the Americas, Brazil accounts for 93% of all reported cases of Leishmania–HIV coinfection (9, 10). The majority of these cases are caused by Leishmania infantum in the country’s Northeast region (7, 11–16). HIV infection accelerates the clinical progression from asymptomatic Leishmania infection to symptomatic VL. In patients with advanced immunosuppression, the disease can present with more severe and atypical manifestations (17). These atypical manifestations may include hemorrhagic events (e.g., epistaxis, ecchymosis, and hematuria), as well as dyspnea, diarrhea, and the involvement of organs not typically affected by Leishmania. Reported atypical sites include the skin, oral mucosa, larynx, lungs, pleura, esophagus, stomach, small intestine, pancreas, and kidneys (18).
Detection of asymptomatic Leishmania-HIV coinfection relies on serological, molecular, and parasitological tests (4, 5). The “gold standard” for VL diagnosis, however, is parasitological confirmation. In Brazil, highly sensitive parasitological diagnoses, such as spleen, liver, and bone marrow aspiration, are commonly employed (19). However, there is currently no gold-standard test or consensus definition for diagnosing asymptomatic Leishmania infection (20, 21). Therefore, optimal surveillance for PLWH in VL-endemic areas requires a combination of diagnostic methods to identify asymptomatic infections and detect atypical clinical manifestations during follow-up (7, 22). Molina et al. (21) demonstrated that HIV-infected individuals with asymptomatic Leishmania infection may transmit the parasite to sand flies, thereby contributing to the maintenance of VL transmission in endemic areas like the Mediterranean (23). To the best of our knowledge, few longitudinal studies have focused exclusively on the outcomes of asymptomatic coinfected patients. This prospective study (2017–2023) aimed to assess the clinical outcomes of asymptomatic Leishmania-HIV coinfected patients and *Leishmania-*negative PLWH in Northeast Brazil.
Materials and methods
2
Study design and samples
2.1
This was a prospective cohort study conducted from January 2017 to September 2023. We followed a cohort of PLWH, including those with asymptomatic Leishmania-HIV coinfection, in the city of Petrolina, State of Pernambuco, Northeast Brazil (7) (Figure 1).
Location of the municipality of Petrolina in the state of Pernambuco, Brazil. Statistics and Geoprocessing Department, Instituto Aggeu Magalhães, Fundação Oswaldo Cruz (IAM/FIOCRUZ), 2025.
The cohort was established based on a 2017 prevalence study that screened 483 PLWH, which identified 44 individuals as having asymptomatic Leishmania-HIV coinfection (7). Inclusion criteria at that time were PLWH 18 years or older who were being treated at the local HIV care service and were on regular Antiretroviral Therapy (ART). Exclusion criteria included current VL treatment, clinical symptoms of VL, or irregular ART use (7).
From 2017 to 2023, longitudinal clinical data were collected from medical records, specifically focusing on incident symptomatic VL, relapse, cause of death, treatment abandonment, and transfer of care. In 2023, the original participants were invited for retesting for Leishmania. A total of 29 asymptomatic Leishmania-HIV coinfected patients and 51 *Leishmania-*negative PLWH from the original cohort were successfully retested.
Cases definitions
2.2
Asymptomatic Leishmania-HIV coinfection: An HIV-positive individual with at least one positive serological or molecular test for VL, but without clinical symptoms (7).Symptomatic Leishmania-HIV coinfection: An HIV-positive patient with laboratory confirmation of VL (parasitological, serological, or molecular test) and clinical symptoms (e.g., fever ≥ 2 weeks, hepatomegaly, splenomegaly, cough, diarrhea, dyspnea, bleeding, weight loss, or mucous pallor) (24).Relapse: Recurrence or worsening of one or more clinical signs (e.g., fever, cytopenia, and hepatosplenomegaly) within 12 months after clinical cure (24).*Leishmania-*negative PLWH: HIV-positive individuals testing negative for Leishmania markers (24).VL-related death: A death in a PLWH with VL symptoms and/or positive Leishmania tests where the cause of death was attributed to VL (24).Abandonment (loss to follow-up): Patients who failed to attend health services for over 3 months after starting treatment or missed appointments for over 6 months, including medication discontinuation or the breakdown of the patient-healthcare provider relationship (24).Transfer of care: Patients unable to continue attending the health center due to relocation (e.g., moving to a different city or state) (24).Regular ART use: Continuous antiretroviral therapy for at least 6 months (24).Seroreversion (or Reversion to negative): A change from positive to negative Leishmania markers in PLWH (25).
Clinical procedures and laboratory analysis
2.3
Baseline (2017) and follow-up (2017–2023) data collection
2.3.1
In 2017, PLWH participants underwent interviews, physical examinations, and peripheral venous blood and urine samples were collected for Leishmania testing (7). From 2017 to 2023, medical records were reviewed for symptomatic VL, relapses, causes of death, abandonment, and transfers of care.
Retesting procedures (2023)
2.3.2
In 2023, participants were re-evaluated with interviews, physical examinations, and peripheral blood collection. Leishmania testing included: Enzyme-Linked Immunosorbent Assay (ELISA)-rK39, the LSH Ab ECO rapid immunochromatographic test (ICT), the Direct Agglutination Test (DAT), and Polymerase Chain Reaction (PCR).
Serological and immunological tests
2.3.3
For the ELISA-rK39 test, we used the recombinant lipoprotein antigen rK39 (Rekom Biotech, Granada, Spain). The assays were performed according to the protocol described by Pedras et al. (26) with minor adaptations. The LSH Ab ECO test (Eco Diagnóstica, Nova Lima, MG, Brasil) (27), which uses rK39 recombinant antigen, was executed the manufacturer’s instructions. For the DAT, we utilized a kit from the Institute of Tropical Medicine Antwerp (ITM-A), Belgium, following the instruction manual. Titers of ≥ 1:1600 were considered positive (28, 29).
Molecular analysis (PCR)
2.3.4
For PCR, we targeted the kinetoplast DNA (kDNA) of Leishmania species. The primers used were 150 (5′-GGG(G/T)AGGGGCGTTCT(C/G)CGAA3’) and 152 (5′-(C/G)(C/G)(C/G)(A/T)CTAT(A/T)TTACACCAACCCC-3′). These primers amplify a 120 bp fragment common to all Leishmania species. PCR conditions were described by Souza et al. (30). To confirm the species as L. infantum, we used the following primers, which amplify a 230 bp product, according to Gualda et al. (31): RLC2 (5’-GGGAAATTGGCCTCCCTGAG-3′) and FLC2 (5’-GTCAGTGTCGGAAACTAATCCGC-3′). Results were analyzed by electrophoresis on 1.5% agarose gels stained with ethidium bromide and visualized under ultraviolet light.
Additional laboratory data
2.3.5
Data on blood count, biochemistry, CD4 + T cell count, and HIV viral load were obtained from medical records.
Ethics statement
2.4
The study protocol was approved by the Ethics Committee of the Instituto Aggeu Magalhães – Oswaldo Cruz Foundation in Pernambuco (approval number 33320920.3.0000.5190). All participants were informed about the study procedures and provided Written Informed Consent (WIC).
Data analysis
2.5
Data were entered and stored in spreadsheets using Microsoft Excel Professional Plus 2016 (Microsoft Corp., Redmond, WA, United States). Statistical analysis was performed using R software, version 4.2.2.
The incidence rate of symptomatic VL was calculated by dividing the number of incident symptomatic VL cases by the total person-time of follow-up among the asymptomatic Leishmania-HIV coinfected patients and the *Leishmania-*negative PLWH groups at baseline.
We also calculated the rate of seroreversion (reversion to negative Leishmania markers) among previously diagnosed Leishmania-HIV coinfected patients. This rate was defined as the number of patients with all negative Leishmania tests at the end of follow-up, divided by the total number of asymptomatic *Leishmania-*HIV coinfected individuals, and presented per 100 people (28).
For descriptive statistics, frequencies with 95% Confidence Intervals (CIs) were calculated. Measures of central tendency were reported as medians and Interquartile Ranges (IQRs) or means and Standard Deviations (SDs), depending on the data distribution. A bivariate analysis was performed to assess the relationship between variables and the outcome. Categorical variables were compared using the Odds Ratio (OR), estimated via the Wald statistic. The significance level was set at 5%, and tests yielding a p-value ≤ 0.05 were considered statistically significant.
Results
3
During the follow-up period (2017–2023), participant retention differed between the two groups. Out of the 44 participants in the asymptomatic Leishmania-HIV coinfected group, 32 remained in the study by 2023. Losses were attributed to: 7 loss to follow-up (abandonment), 1 death due to VL, and 4 transfers of care to other healthcare services. In the PLWH group (initial n = 439), 368 remained in 2023. Losses in this group were due to: 45 transfers of care, 6 loss to follow-up, and 20 deaths from causes unrelated to VL.
By 2023, 29 participants from the Leishmania-HIV coinfected group and 51 from the PLWH group were successfully retested. Three individuals from the coinfected group and one from the PLWH group refused to participate in the retesting procedures (Figure 2).
Participant flow during the prospective follow-up (2017–2023) of Leishmania-negative people living with HIV (PLWH) and asymptomatic Leishmania–HIV coinfected patients in Northeast Brazil.
Of the 29 retested asymptomatic Leishmania-HIV coinfected patients, five remained positive by one or more Leishmania tests during the follow-up. In the PLWH group (n = 51), two individuals seroconverted for Leishmania infection, testing positive by the ELISA-rK39 test (Table 1).
Clinical outcomes are summarized in Figure 3. A total of six participants developed symptomatic VL: five from the asymptomatic Leishmania-HIV coinfected group and one from the Leishmania-negative PLWH group. Three patients experienced VL relapse: one was from the PLWH group (the individual who seroconverted for Leishmania infection) and two were from the asymptomatic coinfected group. Regarding the relapse cases, two participants experienced two episodes each, while one individual suffered six episodes (one per year).
Incident VL, relapse, and mortality during prospective follow-up (2017–2023) of Leishmania-HIV coinfection in Northeast Brazil.
Comparison between groups revealed that both cohorts predominantly resided in urban areas; however, a significantly higher proportion of Leishmania-HIV coinfected participants lived in rural areas compared to Leishmania-negative PLWH (OR 7.20; 95% CI 1.76–29.4; p = 0.004). Asymptomatic coinfected patients were significantly more likely to report weight loss (OR 3.77; 95% CI 1.2–11.88; p = 0.025). In contrast, splenomegaly was only observed in the Leishmania-negative PLWH group (Tables 2, 3).
Table 4 summarizes the incidence of symptomatic VL. During follow-up, the cumulative incidence was 0.17 (5/29) in the asymptomatic Leishmania-HIV group, compared with 0.02 (1/51) in the Leishmania-negative PLWH group. The comparison showed that the coinfected group had a significantly higher cumulative incidence of VL (OR 10.4, 95% CI 1.2–94.2, p = 0.023). Among the 29 retested coinfected participants, 22 seroreverted to negative Leishmania markers, resulting in a seroreversion rate of 75.9 per 100 people over the 2017–2023 follow-up period.
Discussion
4
This study reports the outcomes of a six-year prospective follow-up among two outpatient groups: asymptomatic Leishmania-HIV coinfected individuals and Leishmania-negative PLWH. During the study period, five asymptomatic coinfected participants progressed to symptomatic VL, compared to only one participant in the PLWH group. Statistically, the coinfected group had a significantly higher cumulative incidence of VL (OR 10.4, 95% CI 1.2–94.2, p = 0.023). These findings strongly reinforce existing evidence (7, 28) that PLWH living in VL-endemic areas are at risk of acquiring Leishmania infection and that asymptomatic coinfection is a major risk factor for progression to symptomatic VL.
Few national-level studies in Brazil have addressed the prevalence of Leishmania-HIV coinfection (32, 33), consistently highlighted endemic regions for VL, including the Distrito Federal (34), Ceará (6), Maranhão (35), Mato Grosso (36), Mato Grosso do Sul (37), Minas Gerais (38, 39), Piauí (12), Rio Grande do Norte (40), Sergipe (41), and Tocantins (42). Specifically in Pernambuco, an endemic state for VL, Cavalcanti et al. (16) reported 10 symptomatic Leishmania-HIV coinfection cases among hospitalized PLWH, and Guedes et al. (43) identified a 16.9% prevalence in Recife. In Petrolina (the setting of our study), Diniz et al. (15) reported a 16.8% (107/181) of coinfection using secondary data. More recently, the baseline of the current study reported a 9.1% (44/483) prevalence of asymptomatic *Leishmania-*HIV coinfection in the same region (7). Crucially, this is the first prospective study in Brazil designed to follow and evaluate the long-term outcomes of this specific population.
The diagnosis of asymptomatic Leishmania infection in VL-endemic areas is critical for effective PLWH surveillance and enabling timely intervention should disease progression occur. The challenges in diagnosing asymptomatic Leishmania infection are underscored by the current lack of diagnostic consensus, resulting in the use of various techniques, including parasitological (culture and microscopy), molecular (cPCR, qPCR, LAMP), serological (ELISA, ICT, DAT), and cellular Leishmania skin test (LST), whole blood assay (WBA), cell proliferation assay (CPA) tests (44). In our study, we employed a combination of serological (ELISA, DAT, ICT) and molecular (cPCR) tests across both evaluation periods (2017 and 2023).
Our findings underscore the utility of serological tests for screening and surveillance asymptomatic coinfected individuals, consistent with previous studies (7, 25). However, the LSH Ab ECO rapid test showed a low detection rate, consistent with reports of limited sensitivity for detecting Leishmania infection in PLWH residing in L. infantum-endemic regions (45, 46). In contrast, the ELISA-rK39 test demonstrated the highest positivity rate in the coinfected group (47, 48), further supporting the use of combined diagnostic approaches for detecting asymptomatic infection.
The Brazilian Ministry of Health recommends performing Leishmania serology at the first post-HIV diagnosis appointment for individuals in endemic areas; nevertheless, this is not yet widely implemented in routine clinical practice. Despite implementation challenge, Leishmania testing for PLWH in VL-endemic areas is a core component of the Brazilian Ministry of Health’s control and elimination policies, which could significantly improve treatment and patient outcomes (15, 49, 50). Asymptomatic coinfection remains poorly understood (6, 51). Critically, these individuals may act as reservoirs of infection, potentially contributing to Leishmania transmission due to high parasitic loads, as noted by Molina et al. (21).
Clinical findings revealed a higher frequency of reported weight loss in asymptomatic Leishmania-HIV coinfected group compared to Leishmania-negative PLWH. This is notable, as other studies from Brazil (39, 43, 51, 52) and Ethiopia (53) have typically reported weight loss in symptomatic coinfected patients. HIV-induced immunosuppression weakens the body’s defenses against intracellular parasites like Leishmania species. Furthermore, Leishmania can promote the intracellular replication of HIV, which accelerates the clinical progression of HIV infection and increases symptoms (42). Since weight loss is common in both VL and advanced HIV infection, its higher frequency in our asymptomatic coinfected patients is particularly concerning.
Consistent with Cesse et al. (54), who demonstrated Leishmania transmission in urban areas of Petrolina, our study also identifies asymptomatic Leishmania-HIV coinfection in these settings. This urban finding aligns with the documented epidemiological shift in states like Rio Grande do Norte (55) and Piauí (56), where migration from rural to urban areas has led to Leishmania infection in urban or peri-urban populations. This pattern is not unique to Brazil; studies in Morocco (57, 58), Italy (10), Iran (59), Mexico (60), and Colombia (61) have similarly reported a higher proportion of symptomatic *Leishmania-*HIV coinfected patients in urban areas.
Our study showed that the majority of participants in both groups maintained a CD4^+^ T-cell count of > 350 cells/mm^3^ (p = 0.223), consistent with reports from PLWH in Rio Grande do Norte, Brazil (62). However, when observing patients with advanced immunosuppression (CD4^+^ < 200 cells/mm^3^), a higher proportion was noted in the Leishmania-HIV coinfected group (20.7%) than in the Leishmania-negative PLWH group (9.8%). The lower CD4^+^ T-cell count observed in Leishmania-HIV coinfected patients may be explained by reduced IFN-γ production in response to Leishmania antigens, contributing to atypical parasitic dissemination, frequent relapses, and treatment failure (63).
Our findings identified a non-significant trend toward a higher prevalence of diabetes mellitus, cardiovascular diseases, and hypertension among coinfected individuals compared to the PLWH (p > 0.05). The literature has already associated these comorbidities with PLWH in Brazil (64, 65) and Spain (66). For instance, Pandey et al. (67) reported a case of a 50-year-old Indian male coinfected with Leishmania and HIV who also presented with Parkinsonism, diabetes mellitus, and hyperuricemia. Comorbidities associated with aging, including diabetes, high blood pressure, and cardiovascular diseases, can further compromise the immune system. This increased susceptibility to infection in older adults, may exacerbate the vulnerability of those with HIV and Leishmania-HIV coinfection.
We found 22 cases of seroreversion to negative Leishmania tests among asymptomatic coinfected individuals, resulting in a seroreversion rate of 75.9 per 100 individuals over the 2017–2023 follow-up period. In comparison, a study from northwest Ethiopia (28) found that 16 of 49 individuals with prevalent infection at baseline seroreverted during follow-up (2015–2016), yielding a rate of 48.5 per 100 persons-year. The differences in these rates can be partially attributed to the varying follow-up durations between the two studies.
In the present study, the cumulative incidence of symptomatic VL was significantly higher among asymptomatic Leishmania-HIV coinfected patients compared to the Leishmania-negative PLWH. High frequencies of symptomatic VL, recurrence, and increased mortality, along with a higher rate of relapses and treatment failures, are typically observed among Leishmania-HIV coinfected patients (18, 68). During our follow-up, the risk of progression to symptomatic VL was 10.4 times higher in asymptomatic coinfected patients compared to PLWH living in an VL-endemic area from Northeast Brazil (OR 10.4; 95% CI 1.2–94.2; p = 0.023). Overall, three patients experienced relapse: one was the individual from the Leishmania-negative PLWH group who seroconverted, and two were from the asymptomatic Leishmania-HIV coinfected group.
Additionally, one VL-related death occurred in our study, originating from the asymptomatic Leishmania-HIV coinfected group. In a previous national analysis of 18,501 human VL cases in Brazil (2007–2011), researchers identified risk factors associated with death. The study reported that, at the time of clinical suspicion, death was predicted by the presence of leishmaniasis in PLWH patients (33). HIV seropositivity was the most significant predictor of death among individuals treated for VL, with HIV-infected individuals being four times more likely to die than HIV-negative individuals (69). This high mortality risk is compounded by the fact that, in Brazil, VL cases are often investigated only after severe symptoms are present, which hinders the timely diagnosis of asymptomatic or mild Leishmania infection (11).
Limitations of our study included the difficulty in performing repeated laboratory tests for Leishmania throughout the follow-up, given that patients were primarily monitored by local health services physicians. To mitigate this, information on clinical signs and symptoms was diligently obtained from medical records. Furthermore, the COVID-19 pandemic occurred during the study period, which resulted in changes to healthcare routines that may have affected the monitoring of HIV cases, including ART adherence. A critical limitation is the lack of standardized diagnostic and long-term follow-up protocols for asymptomatic Leishmania-HIV coinfection, which complicates care in HIV outpatient clinics in VL-endemic regions. Therefore, future prospective studies, building upon our findings, are essential to support the development of such protocols.
Conclusion
5
Our six-year prospective study provides critical insights into the long-term outcomes of Leishmania-HIV coinfected patients in VL-endemic areas. It demonstrates that asymptomatic coinfected individuals have a significantly elevated risk of progression to symptomatic VL and subsequent recurrence compared to Leishmania-negative PLWH. Research focusing on asymptomatic Leishmania carriers is crucial for evidence-based public health policymaking in endemic regions, directly contributing to the control and prevention of adverse outcomes. Our findings emphasize the critical need for routine, long-term surveillance and follow-up care for individuals with asymptomatic Leishmania-HIV coinfection to prevent disease progression and mitigate life-threatening complications.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lukes J Mauricio IL Schönian G Dujardin JC Soteriadou K Dedet JP. Evolutionary and geographical history of the Leishmania donovani complex with a revision of current taxonomy. Proc Natl Acad Sci USA. (2007) 104:9375–80. doi: 10.1073/pnas.0703678104, PMID: 17517634 PMC 1890502 · doi ↗ · pubmed ↗
- 2Schwabl P BoitéMC Bussotti G Jacobs A Andersson B Moreira O. Colonization processes and genetic diversification of Leishmania infantum in the Americas. Commun Biol. (2021) 4:139. doi: 10.1038/s 42003-021-01658-5, PMID: 33514858 PMC 7846609 · doi ↗ · pubmed ↗
- 3Lindoso JAL Cunha MA Queiroz IT Moreira CHV. Leishmaniasis–HIV coinfection: current challenges. HIV AIDS. (2016) 8:147–56. doi: 10.2147/HIV.S 93789, PMID: 27785103 PMC 5063600 · doi ↗ · pubmed ↗
- 4Das VNR Bimal S Siddiqui NA Kumar A Pandey K Sinha SK. Conversion of asymptomatic infection to symptomatic visceral leishmaniasis: a study of possible immunological markers. P Lo S Negl Trop Dis. (2020) 14:e 0008272. doi: 10.1371/journal.pntd.0008272, PMID: 32555598 PMC 7326279 · doi ↗ · pubmed ↗
- 5Pederiva MMC Santos SMD Rivarola LGS Guerreiro VJ Lopes KS Lima Junior MSDC. Asymptomatic Leishmania infection in humans: a systematic review. J Infect Public Health. (2023) 16:286–94. doi: 10.1016/j.jiph.2022.12.021, PMID: 36630836 · doi ↗ · pubmed ↗
- 6Távora LGF Nogueira MB Gomes ST. Visceral leishmaniasis/ HIV co-infection in Northeast Brazil: evaluation of outcome. Infect Dis. (2015) 19:651–6. doi: 10.1016/j.bjid.2015.07.004, PMID: 26361839 PMC 9425356 · doi ↗ · pubmed ↗
- 7Guedes DL Justo AM Barbosa Júnior WL Silva EDD Aquino SR Lima Junior MSDC. Asymptomatic Leishmania infection in HIV-positive outpatients on antiretroviral therapy in Pernambuco, Brazil. P Lo S Negl Trop Dis. (2021) 15:e 0009067. doi: 10.1371/journal.pntd.0009067, PMID: 33476331 PMC 7853496 · doi ↗ · pubmed ↗
- 8Kantzanou M Karalexi MA Theodoridou K Kostares E Kostare G Loka T. Prevalence of visceral leishmaniasis among people with HIV: a systematic review and meta-analysis. Eur J Clin Microbiol Infect Dis. (2023) 42:1–12. doi: 10.1007/s 10096-022-04530-4, PMID: 36427170 PMC 9816214 · doi ↗ · pubmed ↗