Impact of COVID‐19 on the Prevalence and Drug Resistance of Haemophilus influenzae in Shandong Province: A Multicenter Retrospective Study
Yanmeng Sun, Mengyuan Wang, Zheng Li, Sijin Man, Shifu Wang

TL;DR
This study shows how the COVID-19 pandemic affected the spread and drug resistance of Haemophilus influenzae in Shandong Province.
Contribution
The study reveals how pandemic measures changed the epidemiology and resistance patterns of H. influenzae in a specific region.
Findings
The isolation rate of H. influenzae dropped significantly during the pandemic, reaching a low in 2020.
Resistance to ampicillin increased from 76.2% before the pandemic to 89.2% after it.
β-lactamase positivity rates rose annually, while β-lactamase-negative ampicillin-resistant strains declined.
Abstract
The COVID‐19 pandemic has profoundly impacted global public health, particularly the epidemiology and antimicrobial resistance patterns of pathogens. This study aimed to assess the influence of COVID‐19 on the isolation rates of Haemophilus influenzae in Shandong Province, providing data support for empirical precision treatment in clinical practice and offering insights for future pandemic response strategies. A retrospective analysis was conducted on laboratory results and clinical records of H. influenzae reported by the Shandong Pediatric Antimicrobial Resistance Surveillance System from 2017 to 2023. A total of 39,043 isolates were included to analyze epidemiological trends and resistance patterns. The isolation rate of H. influenzae significantly declined during the COVID‐19 period, reaching its lowest point in 2020, followed by a rebound in 2023. Male patients accounted for a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
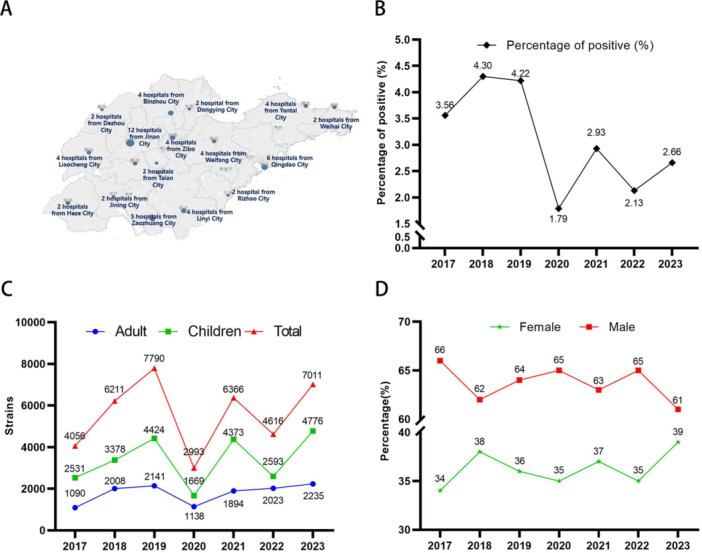 Figure 1
Figure 1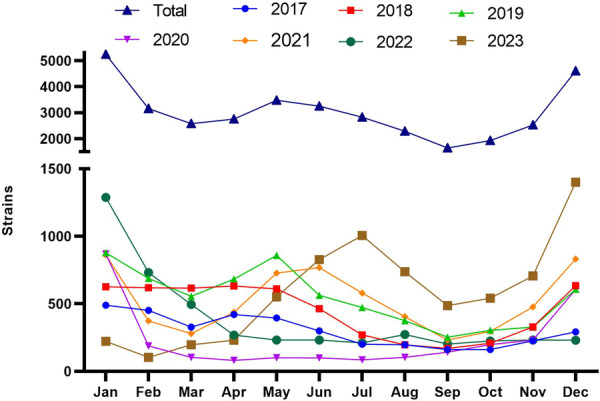 Figure 2
Figure 2| Group | Species | 2017–2019 | 2020–2022 | 2023 |
|---|---|---|---|---|
|
|
|
|
| |
| Sputum | 11172 (91.1%) | 8043 (91.8%) | 4440 (93.0%) | |
| Throat | 497 (4.1%) | 257 (2.9%) | 89 (1.9%) | |
| BALF | 173 (1.4%) | 210 (2.4%) | 124 (2.6%) | |
| vulvar secretion | 155 (1.3%) | 131 (1.5%) | 47 (1.0%) | |
| Ear | 105 (0.9%) | 30 (0.3%) | 5 (0.1%) | |
| Blood | 25 (0.2%) | 23 (0.3%) | 7 (0.1%) | |
| Nose | 19 (0.2%) | 21 (0.2%) | 25 (0.5%) | |
| Pus | 24 (0.2%) | 11 (0.1%) | 10 (0.2%) | |
| Cerebrospinal fluid | 5 (0.0%) | 5 (0.1%) | 1 (0.0%) | |
| Others | 86 (0.7%) | 27 (0.3%) | 28 (0.6%) | |
|
|
|
|
| |
| Sputum | 5433 (93.7%) | 4934 (94.6%) | 2111 (94.5%) | |
| Throat | 46 (0.8%) | 22 (0.4%) | 10 (0.4%) | |
| BALF | 83 (1.4%) | 118 (2.3%) | 70 (3.1%) | |
| vulvar secretion | 24 (0.4%) | 33 (0.6%) | 14 (0.6%) | |
| Ear | 6 (0.1%) | 0 | 1 (0.0%) | |
| Blood | 28 (0.5%) | 21 (0.4%) | 10 (0.4%) | |
| Nose | 14 (0.2%) | 22 (0.4%) | 1 (0.0%) | |
| Pus | 15 (0.3%) | 4 (0.1%) | 2 (0.1%) | |
| Cerebrospinal fluid | 4 (0.1%) | 0 | 0 | |
| Others | 143 (2.5%) | 63 (1.2%) | 16 (0.7%) |
| Year | Number | P% | Mean P% | BLNAR | BLNAR% | Mean BLNAR% | |
|---|---|---|---|---|---|---|---|
| 2017–2019 | 2017 | 2473 | 63.0 | 70.6 | 241 | 9.7 | 8.3 |
| 2018 | 3000 | 72.1 | 237 | 7.9 | |||
| 2019 | 4518 | 76.6 | 328 | 7.3 | |||
| 2020–2022 | 2020 | 1779 | 77.1 | 82.0 | 122 | 6.9 | 5.3 |
| 2021 | 3579 | 84.1 | 172 | 4.8 | |||
| 2022 | 2262 | 85.0 | 92 | 4.1 | |||
| 2023 | 2023 | 4768 | 88.0 | 88.0 | 178 | 3.7 | 3.7 |
| Antibiotic | Drug resistance rate ( |
| |||||
|---|---|---|---|---|---|---|---|
| Total | 2017–2019 ( | 2020–2022 ( | 2023 ( | 2017–2019 vs. 2020–2022 | 2020–2022 vs. 2023 | 2017–2019 vs. 2023 | |
| Ampicillin | 81.6 | 76.2 | 85.0 | 89.2 | < 0.001 | < 0.001 | < 0.001 |
| A/S | 49.9 | 42.9 | 53.0 | 61.9 | < 0.001 | < 0.001 | < 0.001 |
| Cefuroxime | 60.6 | 49 | 67.2 | 74.1 | < 0.001 | < 0.001 | < 0.0001 |
| Cefotaxime | 6.8 | 8.3 | 6.1 | 5.4 | < 0.001 | 0.26 | < 0.001 |
| Meropenem | 1.1 | 0 | 1.0 | 0.6 | 0.01 | 0.02 | < 0.001 |
| Levofloxacin | 1.3 | 1.8 | 1.0 | 0.8 | < 0.001 | 0.24 | < 0.001 |
| Azithromycin | 43.2 | 42.5 | 41.5 | 47.5 | 0.22 | < 0.001 | < 0.001 |
| SXT | 72.9 | 72.8 | 74.7 | 68.5 | 0.007 | < 0.001 | < 0.001 |
| Chloramphenicol | 5.6 | 5.7 | 5.5 | 5.6 | 0.61 | 0.73 | 0.86 |
| Antibiotic | 2017–2019 ( | 2020–2022 ( | 2023 ( | ||||||
|---|---|---|---|---|---|---|---|---|---|
| B+ ( | B− ( |
| B+ ( | B− (n = 1315) |
| B+ ( | B− ( |
| |
| Ampicillin | 97.4 | 18.6 | < 0.001 | 96.5 | 24.7 | < 0.001 | 97.6 | 27.4 | < 0.001 |
| A/S | 48.5 | 23.1 | < 0.001 | 62.4 | 28 | < 0.001 | 70.2 | 23.7 | < 0.001 |
| Cefuroxime | 53.8 | 33.8 | < 0.001 | 73.9 | 47.8 | < 0.001 | 78.2 | 53.6 | < 0.001 |
| Cefotaxime | 8.8 | 6.8 | < 0.001 | 6.1 | 0 | — | 5.9 | 5.2 | 0.63 |
| Meropenem | 1.2 | 0.9 | 0.2 | 0.5 | 0.4 | 0.67 | 0.3 | 0.7 | 0.14 |
| Levofloxacin | 1.5 | 3.3 | < 0.001 | 0.9 | 2.3 | < 0.001 | 0.5 | 1.3 | 0.07 |
| Azithromycin | 52.5 | 7 | < 0.001 | 42.1 | 8.4 | < 0.001 | 53.3 | 4.8 | < 0.001 |
| SXT | 76.9 | 60.2 | < 0.001 | 77.8 | 53.7 | < 0.001 | 70.3 | 52.2 | < 0.001 |
| Chloramphenicol | 6.2 | 4.2 | < 0.001 | 5.1 | 4.1 | 0.1414 | 5.2 | 1.1 | < 0.001 |
| Antibiotic | Vulvar secretion ( | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Total | Children ( | Adult ( | |||||||
| 2017–2019 ( | 2020–2022 ( | 2023 ( |
| 2017–2019 ( | 2020–2022 ( | 2023 ( |
| ||
| Ampicillin | 77.1 | 68.9 | 84.9 | 97.6 | < 0.001 | 46.7 | 71.4 | 72.7 | 0.31 |
| A/S | 56.1 | 36.4 | 54.3 | 76.9 | 0.004 | 27.3 | 58.3 | 81.8 | 0.01 |
| Cefuroxime | 60.9 | 52.2 | 63.3 | 83.3 | 0.001 | 25 | 66.7 | 90 | 0.001 |
| Cefotaxime | 9.2 | 9.1 | 4.9 | 11.1 | 0.98 | 25 | 12.5 | 0 | — |
| Meropenem | 0.5 | 0 | 1.1 | 0 | — | 33.3 | 0 | 0 | — |
| Levofloxacin | 1.2 | 0.7 | 0 | 0 | — | 20 | 0 | 0 | — |
| Azithromycin | 37.1 | 35.6 | 37 | 39.1 | 0.73 | 50 | 55.6 | 20 | 0.35 |
| SXT | 61.2 | 52.7 | 66.1 | 64.5 | 0.09 | 60 | 75 | 76.9 | 0.31 |
| Chloramphenicol | 6.4 | 3.1 | 5.1 | 14.8 | 0.02 | 25 | 14.3 | 0 | — |
- —This study was supported by Shandong Children's Health and Disease Clinical Medical Research Center Project (grant number: RC006), the special fund for high‐level talents in the medical and health ind
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBacterial Infections and Vaccines · Pneumonia and Respiratory Infections · Immune responses and vaccinations
Introduction
1
Haemophilus influenzae is a small, gram‐negative bacterium that commonly colonizes the nasopharynx of healthy individuals and is known for its role in various infections. While it is typically a benign resident, it can cause respiratory infections such as community‐acquired pneumonia and suppurative tonsillitis in children. It can also lead to local infections, including acute otitis media and cellulitis. In severe cases, H. influenzae can enter the bloodstream, potentially resulting in sepsis, suppurative meningitis, and other invasive infections, particularly in children, the elderly, and immunocompromised individuals [1, 2].
During the COVID‐19 pandemic, many countries implemented stringent containment measures to combat the virus. These include social distancing, restrictions on movement and travel, contact tracing, restrictions on gatherings, and restrictions on outdoor activity [3]. While these actions were essential for protecting public health, they also had significant effects on people's lifestyles and habits, altering the transmission dynamics and epidemiological characteristics of various pathogens [4]. Our objective is to assess the impact of the COVID‐19 pandemic on H. influenzae isolated in Shandong region by exploring the characteristics and epidemiological features of the isolates before, during and after the pandemic. This impact may either alter its original epidemic patterns, such as changing the seasonal distribution characteristics, infection rate and drug resistance rate, or it may not. We aim to provide data support for early empirical and precise clinical treatment.
Materials and Methods
2
Study Site
2.1
This study was a retrospective, observational, multicenter surveillance initiative officially launched in 2017 by the Microbiology Laboratory at the Children's Hospital affiliated with Shandong University, which served as the core institution. The study included 59 participating medical institutions, consisting of 52 tertiary hospitals and 7 secondary hospitals, collectively forming the Shandong Province Pediatric Antimicrobial Resistance Surveillance System (SPARSS) net (Figure 1A). The selection of SPARSS network members was guided by principles of geographic representation and demographic distribution to ensure comprehensive coverage and high data representativeness. The network encompassed 16 major cities in Shandong Province. Within the SPARSS network, each participating hospital designated a laboratory liaison officer responsible for data collection and transmission. This arrangement ensured that the core laboratory could receive high‐quality monitoring data for the preceding year at the start of each year. Additionally, the SPARSS network maintained a commitment to open cooperation and resource sharing in scientific research, hosting annual academic conferences where member institutions engaged in detailed discussions on research advancements, technical challenges, and data interpretation, and collaboratively analyzed the previous year's monitoring data. This study was reviewed and approved by the Ethical Review Committee of Children's Hospital Affiliated to Shandong University (approval no. SDFE‐IRB/P‐2022017).
Distribution of Haemophilus influenzae from 2017 to 2023 in Shandong Province. (A) Map of the 59 member units of the SPARSS network. (B) The isolation rate of H. influenzae. (C) Number of strains isolated from adult and child. (D) Male and female proportion of H. influenzae.
Ethics Statement
2.2
This study was reviewed and approved by the Ethical Review Committee of Children's Hospital Affiliated to Shandong University (approval no. SDFE‐IRB/P‐2022017).
Strain Source
2.3
Surveillance data on H. influenzae were collected from 59 member units between January 2017 and December 2023. Data from adult populations across all member units were also gathered to compare differences in pathogen profiles and drug resistance between adults and children. Duplicate isolates from the same source were excluded from the analysis. The inclusion criteria: H. influenzae strains isolated from sterile‐site specimens; for nonsterile‐site specimens, H. influenzae strains grown as pure culture or the dominant bacteria on the selective medium. The exclusion criterion: repeated isolation of H. influenzae strain from the same child. The inclusion criteria: H. influenzae strains isolated from sterile‐site specimens; for nonsterile‐site specimens, H. influenzae strains grown as pure culture or the dominant bacteria on Haemophilus selective medium. The exclusion criterion: repeated isolation of H. influenzae strain from the same child.
Methods
2.4
For strain identification, we utilized matrix‐assisted laser desorption/ionization‐time of flight (MALDI‐TOF) mass spectrometry, an automated microbial identification system, and the API system. Antimicrobial susceptibility testing (AST) was performed by disk diffusion method or automatic instrument method according to the unified scheme. The criteria for interpreting AST results adhered to the Clinical and Laboratory Standards Institute M100‐ED33 [5].
Definitions of the COVID‐19 Pandemic Periods
2.5
The periods from January 2017 to December 2019, January 2020 to December 2022, and January 2023 to December 2023 are designated as before, during and after the COVID‐19 pandemic, respectively.
Age Stratification Criteria
2.6
Children ≤ 14 years old, adults > 14 years old [6].
Data Analysis
2.7
Data analysis was performed using WHONET 5.6 software, while GraphPad Prism 8.0 software was employed for statistical analysis. The χ² test was used to compare drug resistance rates and strain compositions of bacteria. The p < 0.05 was considered statistically significant.
Results
3
Isolates
3.1
From 2017 to 2023, a total of 39,043 strains H. influenzae strains (from the same part of the same patient were excluded) were isolated from the member units of SPARSS network, Figure 1A is the map of the 59 member units of the SPARSS network. Before COVID‐19, the detection rate of H. influenzae was high, with an average of 4.03%. There was a decrease in the epidemic situation, with the largest decrease in 2020, which was the lowest in the past 7 years. In 2021, there was an increase, and in 2022, there was a decrease, with an average of 2.28%. It started to rise again after the COVID‐19 pandemic (Figure 1B). Among which 25,795 strains were in children and 13,248 strains were in adults, accounting for 66.1% and 33.9%, respectively, and most of them were children (Figure 1C). Male patients accounted for 63.4% (24,752/39,039) and female patients accounted for 36.6% (14,287/39,039), and the proportion of males was higher than that of females (Figure 1D).
Seasonal Distribution of H. influenzae
3.2
From 2017 to 2023, the seasonal distribution of H. influenzae is illustrated in Figure 2. Before the COVID‐19 pandemic, isolates were relatively few between August and October. The highest number of isolates was observed in January, February, May, and December, with peaks in December or January. Infections caused by H. influenzae exhibit certain seasonality, with higher incidence in winter and spring, and lower incidence in summer and autumn.
Monthly distribution of strains.
During the COVID‐19 pandemic, the number of isolates in 2020 was higher only in January, and remained low and steady for the following 10 months, with a resurgence beginning in December. The total number of H. influenzae cases detected in 2020 (354 cases) dropped to the lowest level in 4 years, which is consistent with the findings of Qing Meng [7]. In 2022, the number of isolates peaked in January, then steadily decreased until April, and remained at a low level until December.
After the COVID‐19 pandemic, in 2023, the number of isolates was low in January, began to rise gradually from April, and reached its first peak in August, which was delayed by 3 months compared to previous years. In December 2023, it reached the highest point (1401 strains) in the history of monitoring for 7 years.
Strain Source Distribution
3.3
A total of 96.9% (37,832 out of 39,043) of isolates were obtained from respiratory specimens, including 36,133 strains from sputum, 921 strains from throat swabs, and 778 strains from bronchoalveolar lavage fluid (BALF). Among them, there was a noticeable upward trajectory in the proportion of H. influenzae isolated from alveolar lavage fluid, which was observed in both children (χ ^2^ = 35.71, p < 0.001) and adults (χ ^2^ = 20.80, p < 0.001) (Table 1).
In contrast, the proportion of isolates from non‐respiratory specimens was 3.1% (1211 out of 39,043), with vulvar secretions accounting for 28.0% (404 out of 1441). Other non‐respiratory specimens included ear secretions (146), blood (114). nasal secretions (102), and pus (66). Additionally, 15 strains were identified from cerebrospinal fluid (CSF) and 364 from other specimen types (Table 1).
Examining the proportion of H. influenzae isolated from sputum samples of children from 2017 to 2023, we found rates of 91.1% before COVID‐19, 91.8% during the epidemic, and 93.0% after, indicating a rising trend (χ ^2^ = 15.41, p < 0.001). Conversely, the proportion of isolates from throat swabs decreased year by year, with rates of 4.1%, 2.9%, and 1.9%, respectively (χ ^2^ = 56.81, p < 0.001). On the other hand, the proportion from alveolar lavage fluid demonstrated an increasing trend, with rates of 1.4%, 2.4%, and 2.6% over the same period (χ ^2^ = 35.71, p < 0.001) (Table 1).
Changes in Drug Resistance Rate of H. influenzae
3.4
β‐Lactamase Detection
3.4.1
According to β‐lactamase test results from 2017 to 2023, the detection rate of β‐lactamase in H. influenzae increased consistently each year, with rates of 63%, 72.1%, 76.6%, 77.1%, 84.1%, 85%, and 88% (χ ^2^ = 768.8, p < 0.001). The detection rates of β‐lactamase‐negative ampicillin‐resistant H. influenzae (BLNAR) were 9.7%, 7.9%, 7.3%, 6.9%, 4.8%, 4.1%, and 3.7%, respectively (χ ^2^ = 153.8, p < 0.001) (Table 2).
The average percentage of β‐lactamase‐producing H. influenzae was 70.6% (average of 63%, 72.1%, and 76.6%) before the epidemic, 82% (average of 77.1%, 84.1%, and 85%) during the epidemic, and 88% after the epidemic, showing a progressive increase from before to during and after the epidemic (Table 2).
In terms of BLNAR detection rates, the average before the epidemic was 8.3% (average of 9.7%, 7.9%, and 7.3%), during the epidemic was 5.3% (average of 6.9%, 4.8%, and 4.1%), and 3.7% after the epidemic. This indicates a decreasing trend in BLNAR detection from before to during and after the epidemic (Table 2).
Changes in Drug Resistance Rate of H. Influenzae
3.4.2
H. influenzae had high rates of resistance to ampicillin, cefuroxime and trimethoprim‐sulfamethoxazole and low rates of resistance to cefotaxime, meropenem, levofloxacin, and chloramphenicol (Table 3). Furthermore, the resistance rates of H. influenzae to ampicillin, ampicillin sulbactam and cefuroxime exhibited higher levels after the epidemic compared to those observed prior.
To compare the difference in drug resistance between β‐‐lactamase positive and negative strains, we performed a comparative analysis of drug sensitivity of the collected strains (22,379; 57.3%) with β‐lactamase test results. We find the rates of resistance to ampicillin, ampicillin‐sulbactam, azithromycin, and cefuroxime were significantly higher in beta‐lactamase‐producing H. influenzae than in non‐beta‐lactamase‐producing H. influenzae (Table 4).
Changes in Drug Resistance of H. Influenzae in Vulvar Secretions
3.4.3
The amount of H. influenzae isolated from children's vaginal secretions is much higher than that in adults. Additionally, the drug resistance rates of H. influenzae in children's secretions to ampicillin, ampicillin‐sulbactam, cefuroxime and chloramphenicol exhibited a gradual increase before, during, and subsequent to the epidemic (Table 5).
Discussion
4
Since the onset of pandemic, the incidence patterns and frequencies of infectious diseases such as influenza, mycoplasma, chlamydia, and respiratory syncytial virus previously following distinct epidemic rules have experienced significant alterations [8, 9, 10, 11]. H. influenzae is particularly susceptible to infections secondary to influenza and mycoplasma, leading to notable shifts in its detection rates and epidemic patterns before and after the COVID‐19 outbreak. This abrupt change has not only placed immense strain on healthcare systems but has also exacerbated the issue of antimicrobial resistance due to the widespread and excessive use of antibiotics, raising global concerns. Consequently, considerable efforts have been made to identify the risk factors for acquired drug resistance and to implement appropriate management, control, and preventive measures while researching the underlying mechanisms [12].
This study aims to thoroughly analyze the variations in strain sources, seasonal distribution, and antibiotic resistance of H. influenzae isolated from Shandong Province before and after the COVID‐19 pandemic. The goal is to elucidate the impact of COVID‐19 on the intrinsic epidemic patterns and trends of H. influenzae, thereby providing a robust foundation for developing more scientific and effective strategies to combat antibiotic‐resistant infections.
In this study, the proportion of H. influenzae isolated from children was 66.1%, which can be attributed to the immature development of the children's immune system, the limitations and abuse of antibacterial drugs [13, 14, 15]. The majority of H. influenzae isolates were from males (63.4%), suggesting that male is more susceptible to infection with this strain. This discrepancy may be linked to various factors, including genetic differences, immune responses variations, hormonal influences, and potentially a higher prevalence of smoking among males in Shandong Province [16, 17]. Significant differences in the isolation rates of H. influenzae between male and female reveal infections inequality between the sexes again.
Monitoring data revealed significant seasonal fluctuations in H. influenzae infections, with higher incidence rates observed in winter and spring and lower rates in summer and autumn. This pattern aligns with findings reported by Hongjiao Wang [18]. These seasonal changes may be attributed to substantial temperature fluctuations during winter and spring, which can weaken the local immune response of the airway mucosa, facilitating pathogen spread and colonization [19]. These observations indicate that the decline in H. influenzae isolates is closely related to the timing and stringency of COVID‐19 control measures. The subsequent increase from December 2020 to March the following year correlates with the traditional Chinese practice of celebrating the Spring Festival, during which increased population mobility and social interactions lead to a higher incidence of respiratory diseases. The peak period of H. influenzae in 2023 showed a backward shift of about 3 months. Therefore, it is reasonable to suppose that H. influenzae infections will eventually return to pre‐epidemic regularity with society returns to normal interactions [11]. Additionally, compared to previous years, the end of 2023 reached the peak of H. influenzae infections in December in the past 7 years. This may be because H. influenzae is more prone to co‐infection with mycoplasma and influenza viruses during winter and spring seasons. Thus, susceptible children should be encouraged to maintain good respiratory hygiene, wear masks, enhance their nutrient intake, improve physical fitness, and take measures to reduce the risk of H. influenzae infections.
The number of H. influenzae isolates from sputum specimens showed an increasing trend in both demographics. Following throat swabs and bronchoalveolar lavage fluid were the next most common sources. Notably, the number of H. influenzae isolated from bronchoalveolar lavage fluid of both children and adults before the epidemic was less than that during the epidemic. This may be attributed to the fact that COVID‐19 primarily targets the lungs, leading to lower respiratory tract infections, severe pneumonia, and acute respiratory distress syndrome in severe cases [20, 21], and bronchoscopy is one of the important means of clinical evaluation and treatment of pneumonia. The epidemic of COVID‐19 has greatly increased the frequency of bronchoscopy, thereby improving the detection rate of H. influenzae in bronchoalveolar lavage fluid. In non‐respiratory specimens, vulvar secretions represented the highest proportion. Among reproductive health issues in girls, vulvar vaginitis is the most common condition, with Streptococcus pyogenes and H. influenzae identified as prevalent pathogens [22, 23]. This could be related to hygiene practices among children. Previous studies have confirmed that pathogens associated with upper respiratory tract infections can be transmitted to the genital area through oral, nasal, and hand contact [24, 25]. Additionally, Gardnerella vaginalis is frequently found in adult vulvovaginitis cases. Given the differing pathogen compositions in childhood and adult vaginitis, accurate diagnosis of vulvovaginitis caused by H. influenzae in children and the judicious use of antibiotics warrant the attention of clinicians. This study suggests that H. influenzae causes fewer bloodstream and central nervous system infections in children and adults.
Resistance mechanisms to beta‐lactams in H. influenzae are including enzymatic and nonenzymatic mechanism, the most common resistant mechanism to beta‐lactams in H. influenzae is production of beta‐lactamases [26]. Nonenzymatic mechanism to beta‐lactams in H. influenzae can be mediated by modifications in cell permeability, defects in the autolytic system and in overall peptidoglycan synthesis and metabolism, or amino acid substitutions in penicillin‐binding protein 3 (PBP3) encoded by the ftsI gene, and alterations of the target PBPs is the most common nonenzymatic mechanism involved in beta‐lactamase resistance [26]. Historically, ampicillin has been the go‐to medication for treating H. influenzae infections. However, in recent years, the widespread use of antibiotics has led to a significant increase in H. influenzae drug resistance to ampicillin, with resistance levels becoming progressively more concerning [27]. This study observed a consistent yearly rise in the resistance rate of H. influenzae to ampicillin from 2017 to 2023. The primary mechanisms driving ampicillin resistance include the production of β‐lactamase and mutations in penicillin‐binding protein 3 (PBP3) [28]. The detection rate of positive β‐lactamase in H. influenzae exhibited an upward trajectory annually during the study period, aligning with international reports pre‐epidemic, during the epidemic, and post‐epidemic [2]. Clinical bacterial isolates collected from 11 tertiary care children's hospitals in China in 2016 to 2020 indicates that more than 60% of H. influenzae strains produced b‐lactamases [29]. H. influenzae from a tertiary hospital in southwest China indicates that 83.5% of the H. influenzae isolates were positive for β‐lactamase [28]. This trend could be attributed to the common practice of doctors prescribing antibiotics for acute upper respiratory tract infections, with H. influenzae being a major respiratory pathogen in both children and adults [30].
In cases of beta‐lactamase‐negative ampicillin‐resistant H. influenzae (BLNAR), resistance to beta‐lactams results from mutations in penicillin‐binding protein 3 (PBP3) encoded by the ftsI gene [31]. Interestingly, BLNAR exhibited a declining trend throughout the years surveyed, pre‐, during, and post‐epidemic, the decline in BLNAR can be attributed to the following factors. First, during the COVID‐19 pandemic, preventive measures such as mask‐wearing, social distancing, and frequent hand hygiene significantly reduced the transmission of H. influenzae [32]. Additionally, decreased international travel and exchanges with Japan and South Korea may have further contributed to this decline, after all, Japan and Korea have high detection rates of BLNAR [33]. Second, changes in antibiotic prescription patterns, particularly the overall reduction in antibiotic use during the pandemic, may have influenced the prevalence of drug‐resistant strains [34]. Finally, potential detection bias could have played a role, as many hospitals prioritized SARS‐CoV‐2 testing, leading to reduced surveillance of other respiratory pathogens, at the same time, some patients with mild respiratory infections were isolated at home and did not undergo bacterial culture, which may have resulted in an artificial decrease in the reported incidence of BLNAR [35]. In this study, the rate of beta‐lactamase detection in H. influenzae was 57.3%, which is still at a relatively low level. Failure to detect beta‐lactamase may result in underreporting of BLNAR, affecting the results of certain drugs' sensitivity, and therefore, it is necessary to strengthen the detection of beta‐lactamase in H. influenzae. The study also highlighted a high resistance rate of H. influenzae to ampicillin‐sulbactam, with a consistent upward trend observed across the years. In particular, the resistance to ampicillin‐sulbactam increased significantly (48.5% to 70.2%) in β‐lactamase‐positive strains of H. influenzae, which may be associated with a relatively rare BLPACR strain (β‐lactamase‐positive, amoxicillin‐clavulanate‐resistant H. influenzae). Due to the deletion of the breakpoint for amoxicillin‐clavulanate in the CLSI M100 32nd edition (2022), routine testing of ampicillin and sulbactam for amoxicillin‐clavulanate is no longer conducted in this region. BLPACR isolates tend to accumulate mutations in the ftsI gene following exposure to ampicillin. These mutations reduce the affinity of PBP3 for β‐lactam antibiotics, leading to increased resistance to cephalosporins. Therefore, it is crucial to enhance monitoring efforts for these strains. Following the Expert Recommendations on Diagnosis and Treatment of H. influenzae Infection in Children, it is advised to consider third‐generation cephalosporins as the primary empirical treatment, with carbapenem antibiotics like meropenem reserved for severe cases and patients allergic to cephalosporins.
The study noted a relatively high resistance rate of H. influenzae to azithromycin, potentially linked to its common co‐infection with mycoplasma, with azithromycin often being the preferred treatment for mycoplasma and chlamydia infections in children. Conversely, the resistance rate of H. influenzae to levofloxacin was low, likely due to infrequent use of fluoroquinolones in children and newborns, as well as stringent regulations on quinolone antibiotic usage enforced by various departments in China. Over the period of 2017 to 2023, the resistance rate of H. influenzae to SXT ranged from 68.5% to 74.7%, SXT resistance in H. influenzae is usually caused by changes in the folp gene and the sul2 gene [36], aligning with previous reports, suggesting that sulfonamides may no longer be suitable as empirical therapeutics for H. influenzae bloodstream infections. While the resistance rate to chloramphenicol (5.6%) was relatively low in this study, caution is advised in its clinical use due to significant adverse reactions in children.
Conclusion
5
The COVID‐19 pandemic has markedly influenced the epidemiological patterns of H. influenzae in Shandong. This impact not only underscores the profound repercussions of the pandemic on microbial ecology but also offers valuable insights and strategic preparations for a potential “X‐disease” pandemic on a global scale. By conducting precise data analysis, we aim to furnish clinicians with enhanced scientific and expert medication recommendations, refining anti‐infection treatment protocols to better address present and future health challenges. These efforts are geared towards making meaningful contributions to global public health security.
Author Contributions
Yanmeng Sun: data curation, formal analysis, investigation, methodology, project administration, supervision, visualization, writing – original draft. Mengyuan Wang: data curation, formal analysis, investigation, methodology, methodology. Zheng Li: data curation, formal analysis, investigation, resources, supervision. Sijin Man: conceptualization, data curation, formal analysis, investigation. Shifu Wang: conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, project administration, resources, software, supervision, validation, visualization, writing – review and editing.
Conflicts of Interest
1
The authors declare no conflicts of interest.
Transparency Statement
The lead author Shifu Wang affirms that this manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1F. Shooraj , B. Mirzaei , S. F. Mousavi , and F. Hosseini , “Clonal Diversity of Haemophilus influenzae Carriage Isolated From Under the Age of 6 Years Children,” BMC Research Notes 12, no. 1 (2019): 565.31506105 10.1186/s 13104-019-4603-7PMC 6737650 · doi ↗ · pubmed ↗
- 2R. S. W. Tsang and M. Ulanova , “The Changing Epidemiology of Invasive Haemophilus influenzae Disease: Emergence and Global Presence of Serotype a Strains That May Require a New Vaccine for Control,” Vaccine 35, no. 33 (2017): 4270–4275.28666758 10.1016/j.vaccine.2017.06.001 · doi ↗ · pubmed ↗
- 3I. Ayouni , J. Maatoug , W. Dhouib , et al., “Effective Public Health Measures to Mitigate the Spread of COVID‐19: A Systematic Review,” BMC Public Health 21, no. 1 (2021): 1015.34051769 10.1186/s 12889-021-11111-1PMC 8164261 · doi ↗ · pubmed ↗
- 4O. Gasch , L. Badia‐Cebada , J. Carmezim , et al., “Effects of the COVID‐19 Pandemic on Incidence and Epidemiology of Catheter‐Related Bacteremia, Spain,” Emerging Infectious Diseases 28, no. 11 (2022): 2181–2189.36191608 10.3201/eid 2811.220547 PMC 9622263 · doi ↗ · pubmed ↗
- 5CLSI , Performance Standards for Antimicrobial Susceptibility Testing, 33rd ed. CLSI supplement M 100. Clinical and Laboratory Standards Institute. 2023.
- 6I. Fadhil , R. Soliman , S. Jaffar , et al., “Estimated Incidence, Prevalence, Mortality, and Registration of Childhood Cancer (Ages 0–14 Years) in the WHO Eastern Mediterranean Region: An Analysis of GLOBOCAN 2020 Data,” Lancet Child & Adolescent Health 6, no. 7 (2022): 466–473.35605628 10.1016/S 2352-4642(22)00122-5 · doi ↗ · pubmed ↗
- 7Q. Meng , W. Li , H. Jiang , et al., “Comparison of the Distribution and Changes in the Antibiotic Resistance of Clinical Bacterial Isolates From the Lower Respiratory Tract of Children in Shenzhen Before the Epidemic, During the Epidemic, and During the Period of Normalized Prevention and Control of COVID‐19,” Infectious Diseases and Therapy 12, no. 2 (2023): 563–575.36598677 10.1007/s 40121-022-00751-4PMC 9812007 · doi ↗ · pubmed ↗
- 8R. E. Baker , S. W. Park , W. Yang , G. A. Vecchi , C. J. E. Metcalf , and B. T. Grenfell , “The Impact of COVID‐19 Nonpharmaceutical Interventions on the Future Dynamics of Endemic Infections,” Proceedings of the National Academy of Sciences 117, no. 48 (2020): 30547–30553.10.1073/pnas.2013182117 PMC 772020333168723 · doi ↗ · pubmed ↗