When a Freckle May Not Be a Freckle: A Case of Lentigo Maligna
Madeline Tchack, Kiran Javaid, Bassem Rafiq, Noah Musolff, Babar Rao

TL;DR
A case study shows how a seemingly benign freckle was actually a type of melanoma, emphasizing the need for dermoscopy in skin lesion evaluation.
Contribution
Highlights the diagnostic value of dermoscopy in identifying lentigo maligna that appears clinically benign.
Findings
A 51-year-old male's lesion appeared benign but was diagnosed as lentigo maligna via biopsy.
Dermoscopy revealed asymmetric pigmentation, indicating malignancy not visible in clinical inspection.
The case underscores the importance of dermoscopy in accurate skin cancer diagnosis.
Abstract
Lentigo maligna (LM) is a subtype of melanoma that typically arises in chronically sun-exposed skin. A case of LM arising on the right malar cheek of a 51-year-old male patient is presented herein. Clinically, the patient’s lesion appeared benign and lacked overt features of malignancy. Dermoscopic evaluation, however, revealed asymmetric pigmentation concerning for malignancy. A biopsy was subsequently performed, confirming the diagnosis of LM. This case highlights the importance of incorporating dermoscopy into the routine evaluation of pigmented lesions, as reliance on clinical inspection alone may result in misclassification and inappropriate management.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1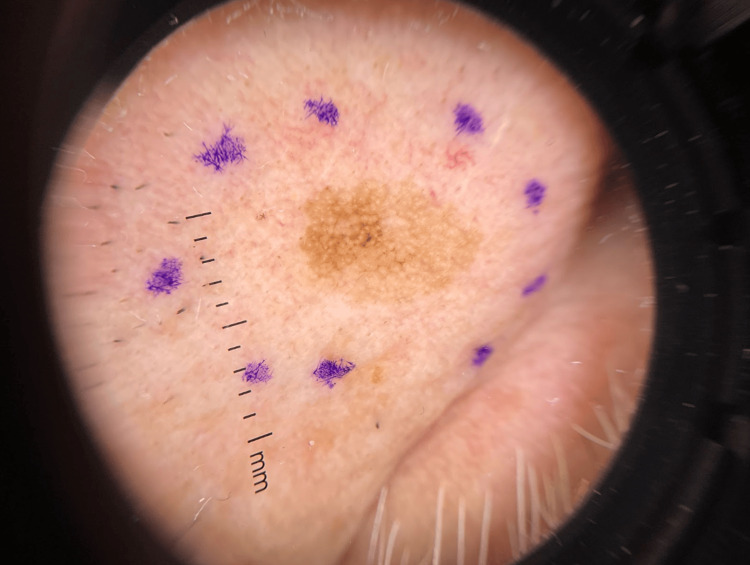 Figure 2
Figure 2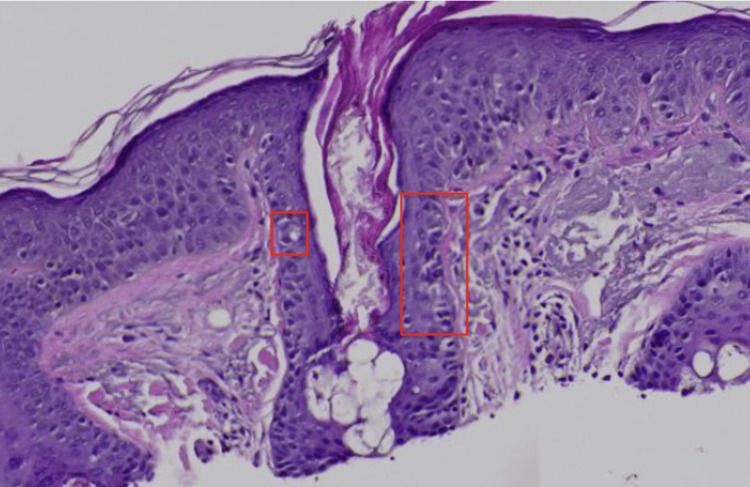 Figure 3
Figure 3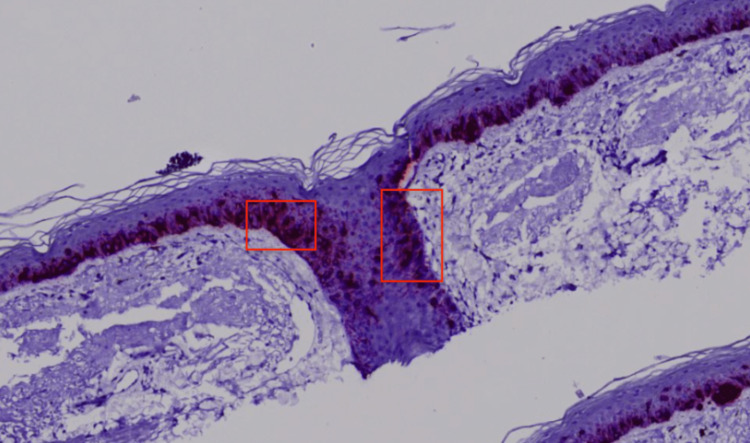 Figure 4
Figure 4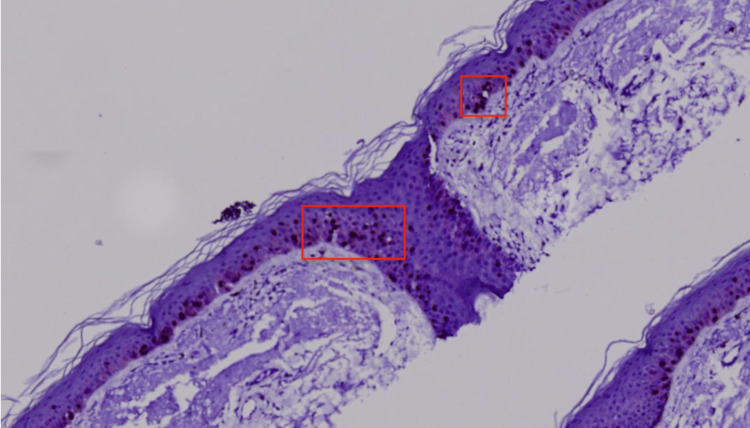 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsArchitecture and Art History Studies · Italian Fascism and Post-war Society
Introduction
Lentigo maligna (LM) is a subtype of malignant melanoma that most commonly presents as an irregularly pigmented brown macule on chronically sun-exposed areas, such as the head and neck [1]. In contrast, solar lentigines and freckles (sunspots) are common benign lesions that frequently arise in the same locations, making early recognition of LM particularly challenging. This diagnostic overlap underscores the clinical relevance of distinguishing a simple “freckle” from an early LM.
Clinically, LM often presents as a slowly enlarging, irregular, tan-brown patch with variegated pigmentation and indistinct borders, most frequently occurring on sun-damaged facial skin such as the cheek and nose [1,2]. Histologically, LM is characterized by atypical melanocytes along the basal layer, often extending down adnexal structures, without dermal invasion [2].
The primary risk factor for developing LM is cumulative ultraviolet radiation [3]. If left undiagnosed, LM may progress to invasive melanoma, most often of the aggressive desmoplastic subtype, in approximately 5-20% of patients [4]. Epidemiologically, LM and LM melanoma (LMM), a more invasive type of LM, account for over 15% of all melanoma cases in the United States, with incidence rates rising steadily in recent decades [5]. Given this potential for progression, accurate and timely diagnosis is critical.
Dermoscopy has been shown to increase diagnostic accuracy nearly ninefold compared to unaided clinical examination [6]; however, LM may still masquerade as a benign lesion on first inspection. Our case is distinctive because the patient’s LM closely resembled a benign freckle and was initially reassured as such by a primary care physician (PCP).
We present this case to highlight how LM can mimic innocuous-appearing pigmented lesions and emphasize the value of dermoscopy in identifying subtle malignant features that may not be apparent on gross clinical examination, underscoring the need for diagnostic vigilance in both dermatologic and primary care settings.
Case presentation
A 51-year-old male patient presented to the dermatology clinic with a light brown macule on the right cheek (Figure 1) that had been present for several months. On review of systems, the patient revealed no pain, itching, fever, chills, night sweats, or unintended weight loss. He had no personal or family history of melanoma or nonmelanoma skin cancer. His past medical history was significant only for an aortic aneurysm. Of note, the patient had been to his PCP approximately one month prior to this appointment, where he was told the lesion was not a cause for concern.
Clinical examination showed a 0.5 x 0.8 cm light brown regular macule on the right cheek.
On clinical examination, the lesion did not exhibit features overtly suspicious for malignancy. As part of routine diagnostic practice, dermoscopy was used and showed an asymmetrical pigmented pseudonetwork with regular borders (Figure 2). Given the lesion’s asymmetric pigmentation observed under a dermatoscope, biopsy versus interval monitoring was discussed as part of his management. Ultimately, the patient opted to proceed with a biopsy.
Dermoscopy demonstrated variegated colors, asymmetrical pigmented follicular openings, and angulated lines creating a pseudonetwork with regular borders.
Histopathological examination revealed melanocytes throughout the epidermis in a pagetoid distribution and atypical melanocytes with large hyperchromatic pleomorphic nuclei and abundant cytoplasm along the basal layer of the epidermis extending down appendages with variably sized and shaped melanocytic nests unevenly distributed in the dermal-epidermal junction (DEJ) (Figure 3). Additional staining was performed, demonstrating positive SOX-10 & MART-1 (Figures 4, 5), confirming the diagnosis of melanoma in situ, LM type. Wide local excision was recommended for further management.
Microphotograph at 400x magnification, stained with H&E. Histopathology showed an increased presence of single and nested pleomorphic cells (red squares) along the dermoepithelial junction including along the hair follicles.
Microphotograph at 400x magnification, immunohistochemically stained with MART-1. The staining revealed an increased uptake of the atypical cells (red squares) at the dermoepithelial junction confirming them to be melanocytes.
Microphotograph at 400x magnification, immunohistochemically stained with SOX-10. The staining revealed an increased uptake of the atypical cells (red squares) at the dermoepithelial junction confirming them to be melanocytes.
Discussion
Sun-exposed areas are particularly susceptible to ultraviolet radiation, and the cumulative effects of sun damage lead to the development of lentigines, freckles, actinic sun damage, and cutaneous malignancies [7]. While these lesions are most often benign, malignant lesions may mimic those that appear benign, both clinically and on dermoscopy [8]. Important differential diagnoses to consider when evaluating freckles include melanoma, LM, and porokeratosis [9].
Lentigines and freckles are common benign lesions, yet rare cases of progression to melanoma in situ have been reported [10]. In our patient, the lesion lacked the classic ABCDE (asymmetry, border, color, diameter, and evolving) criteria [11] used to clinically identify melanoma, thus appearing clinically benign. Inspection with dermoscopy, however, revealed subtle atypical features, including variegated pigmentation, asymmetrical pigmented follicular openings, and angulated lines creating a pseudonetwork. Dermoscopy of a benign solar lentigo often demonstrates a delicate, light brown typical pseudonetwork with uniform pigmentation, whereas an LM is characterized by atypical pseudonetworks with irregular, asymmetric pigmentation surrounding obliterated or distorted follicular openings [12].
This case underscores the importance of incorporating dermoscopy into routine evaluations of new or evolving cutaneous lesions, not only for dermatologists but also for general practitioners. Beyond diagnostic accuracy, dermoscopy can help identify the most diagnostically informative area for biopsy in large or heterogeneous LM lesions, thereby reducing sampling error and improving diagnostic yield [13]. Nevertheless, widespread dermoscopy use in primary care remains limited by barriers such as insufficient training, lack of prioritization for many PCPs, perceived complexity of dermoscopy, and high equipment costs [14]. Despite these challenges, Williams et al. found that most PCPs view dermoscopy as a valuable tool, citing lack of access and training as the primary obstacles, and strongly support its inclusion in residency curricula [15]. Further, a three-month e-learning dermoscopy course for family physicians led to significant diagnostic score improvements in 87.3-92.1% of participants [16], demonstrating that training interventions can be highly effective.
Dermoscopy has consistently been shown to improve skin cancer diagnostic accuracy for dermatologists and PCPs alike [17]. Reliance on clinical examination alone risks misclassifying malignant lesions as benign and improperly managing them with clinical observation. In our case, dermoscopy provided the critical diagnostic cues that prompted biopsy and ultimately revealed LM. This presentation is notable because the lesion was initially misdiagnosed as a benign freckle by a PCP, reflecting the challenge of distinguishing LM from benign pigmented lesions in non-specialist settings.
A limitation of this case is the absence of postoperative follow-up data, including the healing process, aesthetic results, and patient satisfaction. Additionally, detailed information regarding lesion evolution prior to presentation and a formal histologic grading of atypia was not available, which limits further clinicopathologic correlation.
Conclusions
Overall, our case emphasizes the importance of clinical correlation with dermoscopy, not only in dermatology clinics but also in primary care settings. In the absence of dermoscopy, lesions that appear clinically benign may be misclassified as simple “freckles,” potentially delaying diagnosis and treatment of dangerous lesions. Dermoscopy is necessary for physicians to make informed management decisions, and general practitioners who familiarize themselves with dermoscopic patterns can provide more comprehensive dermatologic care. This message is underscored by our patient, who was initially reassured by his PCP that the lesion was benign; without dermoscopy, his diagnosis of LM would have likely been missed. This case highlights how access to dermoscopy in primary care can be particularly valuable in regions where dermatologists are less accessible and where populations rely on general practitioners for holistic care.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lentigo maligna: a review Clin Exp Dermatol Karponis D Stratigos IA Joshy J 2182254920243796671810.1093/ced/llad 394 · doi ↗ · pubmed ↗
- 2Lentigo maligna: clinical presentation and appropriate management Clin Cosmet Investig Dermatol Iznardo H Garcia-Melendo C Yélamos O 83785513202010.2147/CCID.S 224738 PMC 767147333223843 · doi ↗ · pubmed ↗
- 3Lifetime ultraviolet radiation exposure and lentigo maligna melanoma Br J Dermatol Linos E Li WQ Han J Li T Cho E Qureshi AA 1666166817620172792515010.1111/bjd.15218 PMC 5459624 · doi ↗ · pubmed ↗
- 4Reviewing challenges in the diagnosis and treatment of lentigo maligna and lentigo-maligna melanoma Rare Cancers Ther Juhász ML Marmur ES 133145320152718248210.1007/s 40487-015-0012-9PMC 4837936 · doi ↗ · pubmed ↗
- 5Incidence trends of lentigo maligna and lentigo maligna melanoma in the United States from 2000 to 2019 Int J Dermatol Chen Q Zheng M Ling C 6476546320243817336110.1111/ijd.16982 · doi ↗ · pubmed ↗
- 6Dermoscopy compared with naked eye examination for the diagnosis of primary melanoma: a meta-analysis of studies performed in a clinical setting Br J Dermatol Vestergaard ME Macaskill P Holt PE Menzies SW 66967615920081861676910.1111/j.1365-2133.2008.08713.x · doi ↗ · pubmed ↗
- 7Risk factors of lentigo maligna as compared to other melanoma subtypes Int J Dermatol Mitsaki KS Apalla Z Lazaridou E Lallas K Lallas A 06263202410.1111/ijd.1711238419346 · doi ↗ · pubmed ↗
- 8Sunscreens and photoaging: a review of current literature Am J Clin Dermatol Guan LL Lim HW Mohammad TF 8198282220213438782410.1007/s 40257-021-00632-5PMC 8361399 · doi ↗ · pubmed ↗