Sleep Architecture Alterations Following High‐Dose Steroid Pulse Therapy: A Pilot Study Using a Portable Electroencephalogram‐Based Device
Hiroki Endo, Yuki Shigetsura, Misaki Chahara, Keisuke Kido, Etsuro Nakanishi, Sakiho Ueda, Kimitoshi Kimura, Akira Kuzuya, Hirotsugu Kawashima, Riki Matsumoto, Masahiro Tsuda, Shunsaku Nakagawa, Tomohiro Terada

TL;DR
This study shows that high-dose steroid treatment significantly disrupts sleep patterns, particularly REM sleep, using a portable EEG device for the first time.
Contribution
The first objective study using a portable EEG device to demonstrate sleep architecture changes caused by high-dose steroid pulse therapy.
Findings
High-dose steroid pulse therapy significantly reduces REM sleep duration within the first day of treatment.
Portable EEG devices effectively monitor steroid-induced sleep alterations in hospitalized patients.
Total sleep time decreases while non-REM sleep remains relatively stable during high-dose steroid therapy.
Abstract
Sleep disturbance is a common side effect of high‐dose steroid pulse therapy (SPT). However, in clinical settings, the impact of this therapy on sleep architecture has not been objectively studied. This study aimed to investigate changes in sleep architecture associated with high‐dose SPT administration in patients with neuroimmunological disorders. A prospective cohort study was conducted involving six hospitalized patients with neuroimmunological disorders who were administered intravenous methylprednisolone (1000 mg/day for 3 days). Objective sleep parameters were assessed on days 0, 1, and 3 using a SleepGraph, a validated portable electroencephalography (EEG) device. Subjective sleep was evaluated using the Insomnia Severity Index (ISI), Pittsburgh Sleep Quality Index (PSQI), sleep diary, and Likert scale. Rapid eye movement (REM) sleep significantly decreased from 71.2 ± 36.6…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
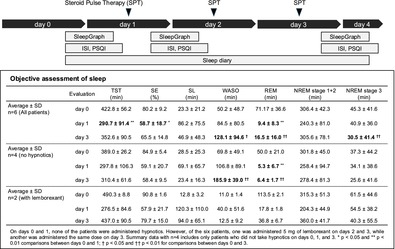 Figure 1
Figure 1| Patient | Sex | Age | BMI (kg/m2) | Underlying disease | Pre‐pulse hospitalization period (days) | ALT (IU/L) | Serum creatinine (mg/dL) | CRP (mg/dL) | ODI‐3 | Regular medications at admission (per day) |
|---|---|---|---|---|---|---|---|---|---|---|
| No. 1 | Male | 50s | 29.12 | Suspected autoimmune disorder with anti‐NAE antibody positivity | 5 | 25 | 1.11 | < 0.10 | 19.53 | Amezinium 10 mg, Droxidopa 400 mg, Fludrocortisone 0.05 mg, Goreisan 7.5 g, Levothyroxine 75 μg, Magnesium oxide 990 mg, Midodrine 4 mg, Vibegron 50 mg |
| No. 2 | Female | 50s | 25.85 | Suspected autoimmune myelitis | 3 | 24 | 0.59 | 0.14 | 8.14 | None |
| No. 3 | Male | 50s | 24.82 | Suspected post‐COVID‐19 myelitis | 10 | 41 | 0.72 | 0.13 | 14.41 | Amlodipine 5 mg, Febuxostat 20 mg, Mecobalamin 1500 μg, Limaprost alfadex 15 μg |
| No. 4 | Male | 20s | 18.60 | Guillain–Barré syndrome | 57 | 22 | 0.65 | < 0.10 | 2.56 | Bilastine 20 mg |
| No. 5 | Female | 30s | 21.64 | Anti‐SRP antibody‐positive myopathy | 4 | 25 | 0.63 | < 0.10 | 6.59 | None |
| No. 6 | Female | 50s | 19.54 | Atypical multiple sclerosis | 3 | 8 | 0.48 | < 0.10 | 1.70 | None |
| Evaluation | TST (min) | SE (%) | SL (min) | WASO (min) | REM (min) | NREM stage 1 + 2 (min) | NREM stage 3 (min) | SO | Final awakening | |
|---|---|---|---|---|---|---|---|---|---|---|
|
Average ± SD
| Day 0 | 422.8 ± 56.2 | 80.2 ± 9.2 | 23.3 ± 21.2 | 50.2 ± 48.7 | 71.17 ± 36.6 | 306.4 ± 42.3 | 45.3 ± 41.6 | 21:46 | 5:41 |
| Day 1 | 290.7 ± 91.4** | 58.7 ± 18.7* | 86.2 ± 75.5 | 84.5 ± 80.5 | 9.4 ± 8.3** | 240.3 ± 81.0 | 40.9 ± 36.0 | 23:08 | 5:23 | |
| Day 3 | 352.6 ± 90.5 | 65.5 ± 14.8 | 46.9 ± 48.3 | 128.1 ± 94.6† | 16.5 ± 16.0†† | 305.6 ± 78.1 | 30.5 ± 41.4†† | 22:19 | 6:20 | |
|
Average ± SD
| Day 0 | 389.0 ± 26.2 | 84.9 ± 5.4 | 28.5 ± 25.3 | 69.8 ± 49.1 | 50.0 ± 21.0 | 301.8 ± 45.0 | 37.3 ± 44.2 | 21:26 | 5:06 |
| Day 1 | 297.8 ± 106.3 | 59.1 ± 20.7 | 69.1 ± 65.7 | 106.8 ± 89.1 | 5.3 ± 6.7** | 258.4 ± 94.7 | 34.1 ± 38.6 | 22:13 | 4:58 | |
| Day 3 | 310.4 ± 61.6 | 58.4 ± 9.5 | 23.4 ± 16.3 | 185.9 ± 39.0†† | 6.4 ± 1.7†† | 278.4 ± 81.3 | 25.6 ± 41.6 | 21:31 | 5:48 | |
|
Average ± SD
| Day 0 | 490.3 ± 8.8 | 90.8 ± 1.6 | 12.8 ± 3.2 | 11.0 ± 1.4 | 113.5 ± 2.1 | 315.3 ± 51.3 | 61.5 ± 44.6 | 22:28 | 6:49 |
| Day 1 | 276.5 ± 84.6 | 57.9 ± 21.7 | 120.3 ± 110.0 | 40.0 ± 51.6 | 17.8 ± 1.8 | 204.3 ± 44.9 | 54.5 ± 38.2 | 1:00 | 6:17 | |
| Day 3 | 437.0 ± 90.5 | 79.7 ± 15.0 | 94.0 ± 65.1 | 12.5 ± 9.2 | 36.8 ± 6.7 | 360.0 ± 41.7 | 40.3 ± 55.5 | 23:56 | 7:26 |
| Evaluation | ISI | PSQI | Sleep diary TST (min) | Sleep diary | Sleep quality Likert scale | Impairment Likert scale | |||
|---|---|---|---|---|---|---|---|---|---|
| SL (min) | WASO (min) | WASO (times) | |||||||
|
Average ± SD
| Day 0 | 8.0 ± 4.9 | 5.3 ± 3.4 | 448.3 ± 30.8 | 33.3 ± 28.6 | 40.8 ± 30.7 | 1.8 ± 1.2 | 6.0 ± 2.3 | 1.7 ± 0.8 |
| Day 1 | 11.2 ± 5.3 | 5.8 ± 2.6 | 276.2 ± 114.7 | 95.0 ± 95.2 | 71.3 ± 104.5 | 1.5 ± 1.4 | 6.0 ± 3.1 | 1.8 ± 1.2 | |
| Day 3 | 11.3 ± 7.2 | 6.5 ± 3.7 | 332.5 ± 125.6 | 54.2 ± 36.1 | 91.7 ± 114.4 | 1.0 ± 0.6 | 5.5 ± 2.7 | 2.3 ± 1.5 | |
|
Average ± SD
| Day 0 | 9.3 ± 5.1 | 4.8 ± 3.2 | 441.3 ± 29.6 | 41.3 ± 33.3 | 53.8 ± 27.5 | 2.3 ± 1.0 | 5.5 ± 2.6 | 2.0 ± 0.8 |
| Day 1 | 10.3 ± 5.7 | 5.5 ± 2.5 | 273.0 ± 142.8 | 93.8 ± 102.7 | 80.8 ± 126.5 | 1.8 ± 1.5 | 5.0 ± 3.5 | 2.3 ± 1.3 | |
| Day 3 | 12.0 ± 6.5 | 5.5 ± 2.4 | 292.5 ± 129.9 | 47.5 ± 12.6 | 118.8 ± 136.2 | 1.0 ± 0.8 | 5.3 ± 3.1 | 3.0 ± 1.4 | |
|
Average ± SD
| Day 0 | 5.5 ± 5.0 | 6.5 ± 5.0 | 462.5 ± 38.9 | 17.5 ± 3.5 | 15.0 ± 21.2 | 1.0 ± 1.4 | 7.0 ± 1.4 | 1.0 ± 0.0 |
| Day 1 | 13.0 ± 5.7 | 6.5 ± 3.5 | 282.5 ± 67.2 | 97.5 ± 116.7 | 52.5 ± 74.3 | 1.0 ± 1.4 | 8.0 ± 0.0 | 1.0 ± 0.0 | |
| Day 3 | 10.0 ± 11.3 | 8.5 ± 6.4 | 412.5 ± 95.5 | 67.5 ± 74.3 | 37.5 ± 31.8 | 1.0 ± 0.0 | 6.0 ± 2.8 | 1.0 ± 0.0 | |
| Patient | Pre‐steroid pulse blood sampling day | Serum cortisol (μg/dL) | Serum ACTH (pg/mL) | Serum allopregnanolone (pg/mL) | Post‐steroid pulse blood sampling day | Serum cortisol (μg/dL) | Serum ACTH (pg/mL) | Serum allopregnanolone (pg/mL) |
|---|---|---|---|---|---|---|---|---|
| No. 1 | Day −2 | 9.3 | 64.8 | 55.2 | Day 12 | 0.5 | < 1.5 | 58.6 |
| No. 2 | Day 0 | 7.3 | 9.0 | 75.5 | N/A | N/A | N/A | N/A |
| No. 3 | Day 0 | 13.4 | 74.0 | 118.5 | Day 5 | 2.6 | 26.0 | 60.7 |
| No. 4 | Day 0 | 10.4 | 38.2 | 109.1 | Day 6 | 3.7 | 43.6 | 132.3 |
| No. 5 | Day 0 | 11.4 | 31.2 | 115.2 | Day 12 | 0.2 | 1.6 | 165.0 |
| No. 6 | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A |
- —JSPS KAKENHI
- —Research Foundation for Pharmaceutical Sciences
- —Japanese Society for Pharmaceutical Palliative Care and Sciences
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSleep and Wakefulness Research · Sleep and related disorders · Epilepsy research and treatment
Introduction
1
High‐dose steroid pulse therapy (SPT) is a standard treatment for neuroimmunological disorders [1, 2], with 1000 mg/day of methylprednisolone for 3 days commonly used globally [3, 4, 5]. Sleep disturbance is a frequent adverse effect of this treatment, occurring in ~70% of patients [6, 7]. However, in clinical practice, no standard treatment has been established for steroid‐induced sleep disturbance. Hypnotics are often administered empirically, but the most effective agent remains unclear. Furthermore, while the effects of corticosteroids on sleep architecture have been demonstrated in rodent models [8], their impact on human sleep architecture in real‐world clinical settings using electroencephalography (EEG)‐based devices has yet to be elucidated. A better understanding of sleep architecture may offer clinically relevant insights into symptoms, comorbidities, and appropriate hypnotics.
Recently, some portable EEG‐based devices have offered a low‐burden alternative with high accuracy and reliability [9, 10, 11, 12, 13]. The present study aimed to investigate changes in sleep architecture following SPT in patients with neuroimmunological disorders using a portable EEG‐based device. Clarifying the alterations in sleep parameters during SPT may help guide the appropriate use of hypnotics to improve patients' quality of life, while also providing insights into the neuropsychopharmacological mechanisms of steroid‐induced sleep disturbance.
Methods
2
Study Participants and Outcome Measurements
2.1
Six hospitalized patients (≥ 18 years) receiving high‐dose SPT (methylprednisolone 1000 mg/body/day for 3 days) for neuroimmunological disorders at Kyoto University Hospital were enrolled between June 2024 and May 2025. Written informed consent was obtained from all participants by the attending physicians or pharmacists. Exclusion criteria included contraindications to portable EEG (e.g., pacemaker use), inability to perform pretreatment evaluation or complete self‐assessments, history of epilepsy, pregnancy or lactation, history of severe drug allergies, high risk of suicide, and regular hypnotic use (unless started after therapy). High‐dose SPT was administered in the morning at a fixed dose of 1000 mg/day, which corresponded to 10–21 mg/kg/day when adjusted for the patients' body weights.
Demographic, clinical, and sleep‐related data were collected, along with residual serum samples during the course of SPT, specifically on days 0, 1, and 3. Serum allopregnanolone, a neurosteroid implicated in steroid‐induced sleep disturbance [14, 15], was measured using a commercial enzyme‐linked immunosorbent assay (ELISA) kit (Abcam, Cambridge, UK). Cortisol and adrenocorticotropic hormone (ACTH) levels were also measured. Serum cortisol was quantified using the AIA‐Pack CL Cortisol assay on the AIA‐CL2400 analyzer (Tosoh Bioscience, Tokyo, Japan) with the chemiluminescent enzyme immunoassay (CLEIA) method. ACTH was measured using the Elecsys ACTH assay (Roche Diagnostics K.K., Tokyo, Japan) on the cobas 8000 e801 analyzer (Roche Diagnostics K.K., Tokyo, Japan) based on the electrochemiluminescence immunoassay (ECLIA) method.
Objective or Subjective Assessment of Sleep
2.2
Objective sleep was assessed using the SleepGraph (Proassist, Osaka, Japan) before (day 0) and on days 1 and 3 of SPT. The SleepGraph is a portable, EEG‐based device that employs four surface electrodes placed at the following sites: the right frontal scalp (Fp2), the infra‐orbital area beneath the left eye, the right mandibular angle, and the left mastoid (M1). The Fp2‐to‐M1 derivation simultaneously captures EEG activity and the right electro‐oculogram (EOG), whereas the infra‐orbital‐to‐M1 derivation records the left EOG. Chin muscle tone is measured via an electromyogram channel obtained between the right mandibular electrode and M1.
To minimize patient burden and avoid disturbing natural sleep, we employed the telemetry EEG‐based device SleepGraph. Furthermore, SleepGraph provides a sufficient number of channels to enable manual scoring. The SleepGraph is an approved medical device in Japan (approval number: 231AHBZX00001000). Sleep data were scored manually according to the standard criteria in 30‐s epochs as Stage W, Stage N1 + N2 (NREM N1–2), Stage N3 (NREM N3), or Stage R (REM). Subjective sleep was evaluated using a sleep diary [16], 10‐point Likert scales for sleep quality and daytime impairment, and validated Japanese versions of the Insomnia Severity Index (ISI‐J) [17] and Pittsburgh Sleep Quality Index (PSQI‐J) [18]. The sleep diary tracked bedtimes, sleep latency (SL), number and duration of awakenings, and final wake‐up times throughout the study.
Statistical Analysis
2.3
Statistical analyses were conducted using R software (v4.2.1; R Foundation for Statistical Computing, Vienna, Austria) with the nlme and emmeans packages. A linear mixed‐effects model, specifying day as a fixed effect and subject as a random effect, was used to compare days 0, 1, and 3 using Tukey's test. Significance was set at 5%. A post hoc power analysis using the pwr package was performed based on a two‐sided paired t‐test (α = 0.05), estimating power from the observed effect size (Cohen's d) and sample size (n = 6).
Results
3
Patient Characteristics
3.1
The characteristics of the six patients included in this study are summarized in Table 1. The mean age of the six patients was 46 years, with an equal distribution of males and females. No hypnotics were used on days 0 and 1; however, 5 mg of lemborexant was administered to Patient 4 on days 2 and 3, and to Patient 5 on day 3. One patient exhibited a 3% oxygen desaturation index (ODI‐3) > 15. No psychiatric symptoms such as steroid‐induced depression were clinically observed during steroid treatment, although standardized assessment tools were not applied.
Alterations in Sleep Architecture Assessed Using a Portable EEG‐Based Device
3.2
The data measurement status was stable over each recording night, with only minimal artifacts. The objective sleep parameters are summarized in Table 2. The individual patient‐level objective sleep parameters are provided in Table S1, and a representative recording is shown in Figure S1. In all patients (n = 6), total sleep time (TST) significantly decreased from day 0 (422.8 ± 56.2 min) to day 1 (290.7 ± 91.4 min; p < 0.01) and remained reduced on day 3 (352.6 ± 90.5 min). REM sleep also decreased significantly on day 1 (9.4 ± 8.3 min; p < 0.01) and remained lower on day 3 (16.5 ± 16.0 min) compared with day 0 (71.2 ± 36.6 min). SL and wake after sleep onset (WASO) showed increasing trends after day 0, although the differences were not statistically significant. Stage N3 duration was significantly reduced on day 3 compared to that on day 0 (p < 0.01). In patients who did not receive hypnotics (n = 4), REM sleep was significantly reduced on both day 1 (5.3 ± 6.7 min; p < 0.01) and day 3 (6.4 ± 1.7 min; p < 0.01) compared to day 0 (50.0 ± 21.0 min). WASO was also significantly prolonged on day 3 (185.9 ± 39.0 min) versus day 0 (69.8 ± 49.1 min; p < 0.01). Two patients who received lemborexant (5 mg) on day 3 showed improved TST (276.5 ± 84.6 min on day 1 to 437.0 ± 90.5 min on day 3) and REM sleep (17.8 ± 1.8 min to 36.8 ± 6.7 min), though these did not return to baseline levels.
Changes in Subjective Sleep Measures
3.3
Table 3 shows changes in subjective sleep parameters across days 0, 1, and 3. The individual patient‐level subjective sleep parameters are provided in Table S2. TST significantly decreased from day 0 (448.3 ± 30.8 min) to day 1 (276.2 ± 114.7 min; p < 0.01). ISI and PSQI scores showed no significant changes over time. SL and WASO tended to increase on day 1, but without statistical significance. Likert‐scale ratings for sleep quality and daytime impairment also remained stable, though a slight increase in impairment was reported on day 3.
In patients not receiving hypnotics (n = 4), TST decreased similarly on day 1 (273.0 ± 142.8 min) compared with day 0 (441.3 ± 29.6 min), while other parameters remained stable. The two patients who received lemborexant showed increased TST on day 3 (412.5 ± 95.5 min vs. 282.5 ± 67.2 min on day 1). Apart from the administration of lemborexant, no changes in concomitant medications, physical conditions, or sleep environments that could have affected sleep were observed in these patients.
Serum Hormone and Neurosteroid Levels
3.4
Serum hormone and neurosteroid levels assessed in five patients with baseline data showed serum cortisol levels of 7.3–13.4 μg/dL, ACTH of 9.0–74.0 pg/mL, and allopregnanolone of 55.2–118.5 pg/mL. Post‐treatment samples (n = 4) showed marked suppression of cortisol (0.2–3.7 μg/dL) and ACTH (< 1.5–43.6 pg/mL), while allopregnanolone levels varied (58.6–165.0 pg/mL) without a consistent pattern. Individual data are presented in Table 4.
Discussion
4
To our knowledge, this study is the first clinical report to evaluate steroid‐induced sleep disturbance using a portable EEG‐based device. As expected, reduced TST was objectively confirmed by the sleep study. High‐dose SPT markedly reduced REM sleep in this study. Short‐term REM reduction is linked to negative mood states, amygdala hyperactivity, impaired anterior cingulate connectivity, memory deficits, anxiety, irritability, impaired concentration, and stress‐related prefrontal dysfunction [19, 20, 21, 22]. Furthermore, long‐term REM loss is associated with increased mortality and dementia risk [23, 24], highlighting the importance of REM preservation during treatment. As SPT is often followed by longer oral regimens, strategies to preserve REM sleep may be clinically important. Notably, in two patients, lemborexant improved almost all sleep parameters. This observation is consistent with prior evidence from rodent models and clinical trials in humans demonstrating that lemborexant increases both REM and NREM sleep. These findings suggest favorable effects of lemborexant on sleep parameters [25, 26]. Apart from the administration of lemborexant, no changes in concomitant medications, physical conditions, or sleep environments that could have affected sleep were observed, suggesting that the improvements in sleep parameters were attributable to lemborexant. However, the varying effects of hypnotics underscore the need for further research on optimal agents [27, 28]. These findings provide important insights toward elucidating the clinical picture of SPT‐induced sleep disturbance, and understanding changes in sleep parameters alongside patients' clinical symptoms. As such knowledge may facilitate evidence‐based strategies, such as the early detection of REM sleep, NREM sleep, and TST reduction during SPT and the rational selection of hypnotics like orexin receptor antagonists, to mitigate sleep disruption and improve patient outcomes. Furthermore, they contribute to the neuropsychopharmacological field by demonstrating a clear association between corticosteroid exposure and objectively measured changes in sleep parameters.
In this study, some patients exhibited near‐complete loss of REM sleep. Given the high inter‐scorer reliability of SleepGraph, these changes likely reflect true alterations rather than scoring artifacts [29]. Obstructive sleep apnea syndrome (OSAS) may cause sleep fragmentation and reduced REM sleep [30]. One patient had an ODI‐3 ≥ 15, indicating possible OSAS influence, while others did not, suggesting limited impact.
The mechanism underlying the reduction of REM sleep associated with steroid‐induced insomnia remains unclear; however, several hypotheses can be considered. The occurrence of REM sleep is regulated by a flip‐flop switch between the ventrolateral preoptic nucleus and brainstem arousal centers that include orexin‐producing neurons. Orexin neurons have been reported to express glucocorticoid receptors [31], suggesting that steroids may influence orexin activity. Furthermore, chemogenetic activation of orexin neurons has been shown to shorten total REM sleep time [32], raising the possibility that steroid exposure may have contributed to the reduction of REM sleep observed in the present study. In fact, the finding that an orexin receptor antagonist improved the REM sleep shortening induced by SPT provides additional support for this hypothesis.
Moreover, steroids are known to suppress nocturnal melatonin synthesis [33], and insufficient nocturnal melatonin secretion has been reported to shorten REM sleep [34]. Thus, it is also conceivable that steroids reduce REM sleep via suppression of melatonin secretion. In any case, these remain hypotheses, and further studies are warranted to elucidate the underlying mechanisms.
Subjective tools such as the ISI and PSQI exhibited limited sensitivity to short‐term changes, which may explain the discrepancy with sleep studies. However, as these tools were originally designed to assess sleep for 2 weeks or more [17, 18], simpler tools such as portable EEG‐based devices or sleep diaries may be more suitable for short‐term clinical monitoring.
Although the mechanisms of steroid‐induced sleep disturbance remain unclear, they may involve hypothalamic–pituitary–adrenal axis hyperactivity or reduced levels of neurosteroids, such as allopregnanolone [6]. The lack of a consistent trend in allopregnanolone levels suggests that peripheral measures may not fully capture central neurosteroid dynamics, or there may be limitations in sample timing and consistency. Further mechanistic studies are warranted.
The first limitation of this report includes the small sample size, single‐center design, background heterogeneity, and the absence of a non‐steroid control group, as this was a single‐arm study. Consequently, the disease‐related alternation in sleep could not be specifically evaluated. For example, Guillain‐Barré syndrome has been reported to be associated with sleep disturbances, particularly due to sleep‐disordered breathing and fragmented sleep parameters [35].
However, a post hoc power analysis confirmed the large effects observed (e.g., REM sleep; Cohen's d = 1.90, power = 0.96). The second limitation is the use of a portable EEG‐based device instead of standard polysomnography. However, the SleepGraph system has demonstrated high consistency with polysomnography [36, 37] and high inter‐scorer reliability in diverse sleep research [29], supporting its validity. Further studies should investigate underlying mechanisms and evaluate long‐term interventions to mitigate steroid‐induced sleep disturbance.
Conclusion
5
Our findings provide novel clinical evidence that high‐dose SPT objectively and markedly reduces TST, REM sleep, and NREM sleep. These results highlight a previously underrecognized impact of corticosteroid therapy on patient sleep. The portable EEG‐based device offers a feasible approach for detecting steroid‐induced sleep alterations. Further studies are required to clarify the underlying mechanisms and to identify effective interventions to preserve sleep architecture during corticosteroid therapy.
Author Contributions
Study design and conceptualization were performed by H.E., Y.S., and K. Kido. Data were acquired by H.E., Y.S., and M.C. Sleep data were scored, and representative data were selected by K. Kido. Data analysis and interpretation were performed by H.E., Y.S., and K. Kido. H.E. and Y.S. drafted the manuscript. Critical revision of the manuscript for important intellectual content was performed by H.E., Y.S., M.C., K. Kido, H.K., E.N., S.U., K. Kimura, A.K., R.M., M.T., S.N., and T.T. All authors reviewed and approved the final manuscript and accept full responsibility for its content, including the investigation and resolution of any issues concerning its accuracy and integrity.
Ethics Statement
This study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the Ethics Committee of Kyoto University Graduate School of Medicine, School of Medicine, and Faculty of Medicine Hospital (Approval Number, R4438).
Consent
Written informed consent was obtained from all participants before their study inclusion.
Conflicts of Interest
The authors declare no conflicts of interest.
Supporting information
Figure S1: npr270071‐sup‐0001‐Figure S1.docx.
Table S1: npr270071‐sup‐0002‐TableS1.xlsx.
Table S2: npr270071‐sup‐0003‐TableS2.docx.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1D. B. Sanders , G. I. Wolfe , M. Benatar , et al., “International Consensus Guidance for Management of Myasthenia Gravis: Executive Summary,” Neurology 87, no. 4 (2016): 419–425.27358333 10.1212/WNL.0000000000002790 PMC 4977114 · doi ↗ · pubmed ↗
- 2S. E. Leonhard , M. R. Mandarakas , F. A. A. Gondim , et al., “Diagnosis and Management of Guillain‐Barré Syndrome in Ten Steps,” Nature Reviews Neurology 15, no. 11 (2019): 671–683.31541214 10.1038/s 41582-019-0250-9PMC 6821638 · doi ↗ · pubmed ↗
- 3T. Kümpfel , K. Giglhuber , O. Aktas , et al., “Update on the Diagnosis and Treatment of Neuromyelitis Optica Spectrum Disorders (NMOSD)—Revised Recommendations of the Neuromyelitis Optica Study Group (NEMOS). Part II: Attack Therapy and Long‐Term Management,” Journal of Neurology 271, no. 1 (2024): 141–176.37676297 10.1007/s 00415-023-11910-z PMC 10770020 · doi ↗ · pubmed ↗
- 4B. Yamout , M. Al‐Jumah , M. A. Sahraian , et al., “Consensus Recommendations for Diagnosis and Treatment of Multiple Sclerosis: 2023 Revision of the MENACTRIMS Guidelines,” Multiple Sclerosis and Related Disorders 83 (2024): 105435.38245998 10.1016/j.msard.2024.105435 · doi ↗ · pubmed ↗
- 5H. Murai , “The Japanese Clinical Guidelines 2022 for Myasthenia Gravis and Lambert‐Eaton Myasthenic Syndrome: An Overview,” Brain and Nerve 76, no. 1 (2024): 7–12.38191133 10.11477/mf.1416202551 · doi ↗ · pubmed ↗
- 6J. L. Cole , “Steroid‐Induced Sleep Disturbance and Delirium: A Focused Review for Critically Ill Patients,” Federal Practitioner 37, no. 6 (2020): 260–267.32669778 PMC 7357890 · pubmed ↗
- 7T. Fujita , Y. Fukuyama , N. Misumi , and T. Nishino , “Investigation on the Onset of Insomnia Resulting From the Introduction of Steroids in Collagenosis Internal Medicine,” Japanese Journal of Hospital Pharmacy 53, no. 10 (2017): 1257–1260.
- 8T. Kato , G. Okawa , K. F. Tanaka , and Y. Mitsukura , “Dexamethasone Induces Sleep Disturbance in a Dose‐Dependent Manner in Mice,” P Lo S One 18, no. 12 (2023): e 0296028.38117835 10.1371/journal.pone.0296028 PMC 10732373 · doi ↗ · pubmed ↗