Adverse health outcomes among migrant workers and transnational families in the Asia–Pacific: a systematic review and meta-analysis
Rosita Chia-Yin Lin, Karen Lau, Kathryn Mackey, Natasha Roya Matthews, Maushmi Selvamani, Morais Beatriz, Bouaddi Oumnia, Chaelin Kim, Azusa Iwamoto, Masami Fujita, Ursula Trummer, Tran Ngoc Dang, Alena Kamenshchikova, Cathy Zimmerman, Sally Hargreaves

TL;DR
Migrant workers in the Asia-Pacific face high rates of work-related injuries and health issues, with their families also experiencing mental health and nutrition problems.
Contribution
This study provides the first systematic review and meta-analysis of health outcomes among migrant workers and their families in the Asia–Pacific region.
Findings
Migrant workers in the Asia-Pacific region experience high rates of occupational injuries and illnesses, with 37% reporting at least one work-related morbidity.
Transnational families left behind show significant mental health issues (50.1%) and undernutrition (31.4%).
Migrant workers face higher health risks compared to local workers, with a pooled relative risk of 1.29 for work-related morbidities.
Abstract
Labour migration is a growing global phenomenon, with migrant workers known to be more likely to experience exploitative and precarious work, impacting their health. Despite hosting over 27 million international migrant workers, the Asia–Pacific region remains underrepresented in global health evidence, limiting the development of targeted, region-specific health interventions. This study aims to investigate the health status of migrant workers and their transnational families in the Asia–Pacific region. We conducted a systematic review and meta-analysis (PROSPERO: CRD42024528561) of primary studies published between Jan 1, 2013, and April 1, 2024. We searched MEDLINE, Embase, PsycINFO, and Ovid Global Health for studies reporting work-related morbidity and mortality among international migrant workers and their transnational families in the Asia–Pacific region. A narrative synthesis…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
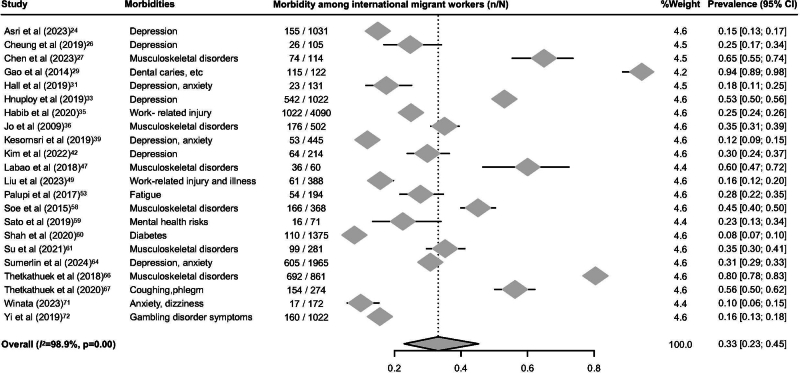 Figure 1
Figure 1 Figure 2
Figure 2 Figure 3
Figure 3 Figure 4
Figure 4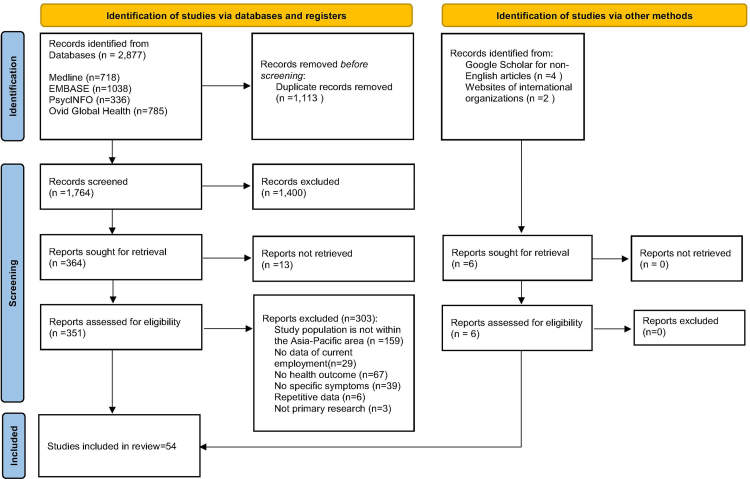 Figure 5
Figure 5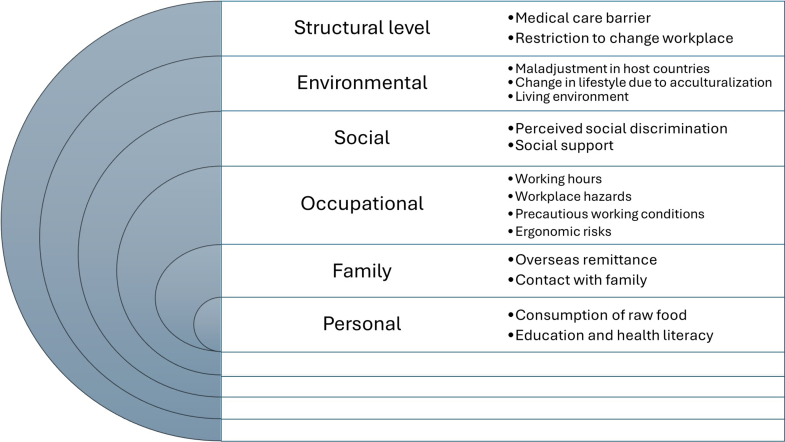 Figure 6
Figure 6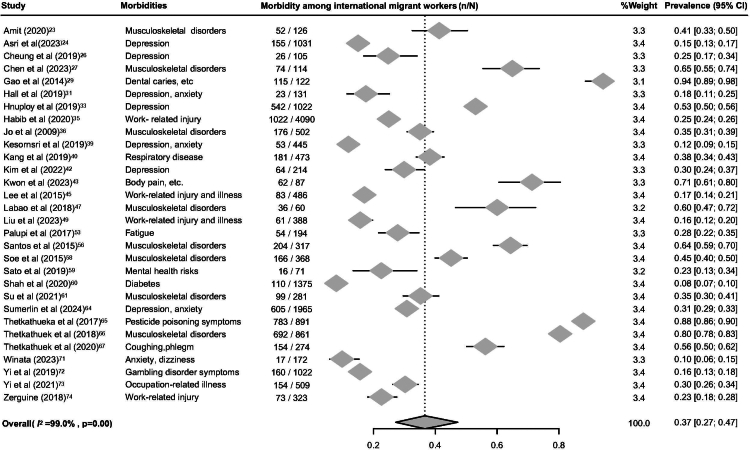 Figure 7
Figure 7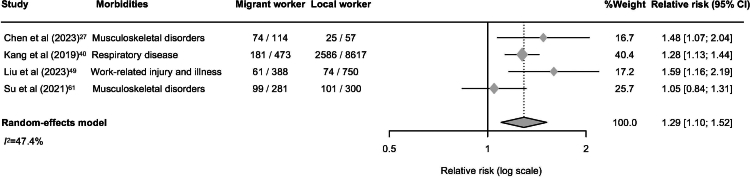 Figure 8
Figure 8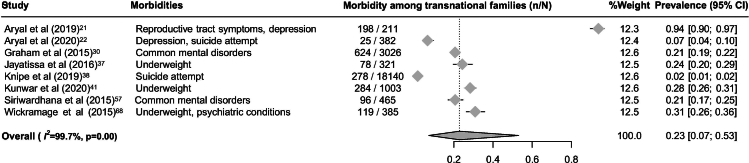 Figure 9
Figure 9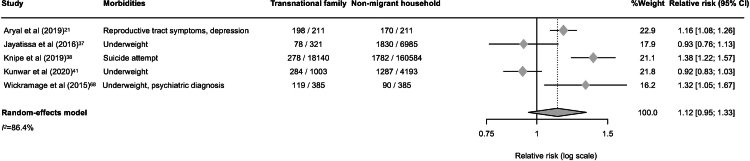 Figure 10
Figure 10- —Ministry of Education
- —10.13039/100010269Wellcome Trust
- —10.13039/501100000265UK Medical Research Council
- —UK National Health Institute for Health and Care Research
- —10.13039/100010434‘la Caixa' Foundation
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMigration, Health and Trauma · Global Health Workforce Issues · Sex work and related issues
Research in contextEvidence before this studyLiterature on the health of migrant workers and their transnational families—including left-behind children—has consistently reported adverse outcomes globally. Three systematic reviews have examined occupational health among migrant workers. Hargreaves et al. reported a 47% pooled prevalence of at least one occupational morbidity among 7260 migrant workers (95% CI: 29–64). Lau et al. found a significantly higher risk of fatal injuries among migrants when compared with local workers (relative risk = 1.71; 95% CI: 1.22–2.38), while Pega et al. reported higher occupational injury rates (relative risk = 1.27; 95% CI: 1.11–1.45). Regarding transnational families, a global review by Fellmeth et al. showed left-behind children were at increased risk of depression (relative risk = 1.52; 95% CI: 1.27–1.82), anxiety (relative risk = 1.85; 95% CI: 1.36–2.53), wasting (relative risk = 1.13; 95% CI: 1.03–1.24), and stunting (relative risk = 1.12; 95% CI: 1.00–1.26) compared to non-migrant households. Antia et al. similarly reported higher levels of depression and loneliness in left-behind children.According to updated estimates by the International Labour Organization (ILO) in 2022, the Asia–Pacific region hosts approximately 27.2 million migrant workers, accounting for 16% of the global migrant workforce. Despite growing interest in the health impacts of labour migration and the potential to leverage work as a platform for health improvement, the Asia-Pacific—one of the world's major hubs for labour migration—has not been the focus of a comprehensive analysis. Evidence on the health effects of labour migration in the region remains limited, particularly regarding the health outcomes of both migrant workers and their transnational families.Added value of this studyThis systematic review and meta-analysis provide the first comprehensive synthesis of health outcomes among migrant workers and their transnational families, including children, spouses and adult relatives left-behind in the countries of origin, in the Asia–Pacific region. Based on data from 86,620 individuals, we found that over 75% of migrant workers worked in high-risk sectors such as manufacturing, construction, and services. Among migrant workers, 88.4% reported occupational injuries and illnesses (n = 45,661), 3.8% experienced symptoms of mental health disorders (n = 1975), and another 3.8% reported musculoskeletal disorders (n = 1973), largely associated with precarious working conditions and limited access to healthcare. Health impacts of labour migration also extended to transnational families. Mental health issues—including suicide attempts and psychiatric diagnoses among children—were reported in 50.1% of cases (n = 1520), and 31.4% experienced undernutrition (n = 954).Implications of all the available evidenceThe health needs of migrant workers in the Asia–Pacific remain insufficiently addressed in both research and policy, despite their vital economic contributions. Global frameworks such as Sustainable Development Goal (SDG) 8.8 call for stronger health protections through coordinated efforts between labour-sending and -receiving countries—efforts that require robust, context-specific evidence. This gap underscores the urgent need for evidence-based strategies to improve occupational safety, regulate working hours, and ensure healthcare access. Given the cross-border impacts on transnational families, stronger coordination and integration of global frameworks into national policies are essential to protect migrant health and well-being.
Introduction
Labour migration is a global phenomenon, with 167.7 million migrant workers worldwide in 2022–4.7% of the global labour force—reflecting a 30 million increase since 2013 (ILO).1 Nearly 70% reside in high-income countries, mainly in agricultural, industrial, and service sectors.1 Evidence shows substantial health risks among migrant workers. Hargreaves et al. reported high rates of musculoskeletal disorders (MSDs), dermatological infections, depression, and occupational injuries, largely due to precarious conditions (low wages, long hours, undocumented status).2 Pega et al. found higher occupational injury morbidity in migrant versus local workers (relative risk = 1.27; 95% CI: 1.11–1.45),3 and Lau et al. reported a higher risk of fatal workplace injuries (relative risk = 1.71; 95% CI: 1.22–2.38), despite migrants often being healthier at baseline.4 Labour migration also affects transnational families, with studies by Fellmeth et al. and Antia et al. showing that left-behind children face greater risks of mental health conditions and undernutrition, including being underweight, compared to peers in non-migrant households.5^,^6
Despite these known challenges, research specifically examining the health of migrant workers and their transnational families in the Asia–Pacific region remains limited, even though the region hosts approximately 27.2 million migrant workers.1 In the Asia–Pacific, this reality is exemplified by the Philippines, where large numbers of overseas Filipino workers leave behind children who often experience reduced parental involvement and face heightened risks of adverse health outcomes.7
Several international frameworks have been established to protect the health and rights of migrant workers. The World Health Organization Global Plan of Action on Workers’ Health 2008–2017 (WHO GPA) called for reducing health disparities between migrant and local workers.8 Within the United Nations Sustainable Development Goals (SDGs), Goal 8.8 promotes safe and secure working environments for all workers, including migrants.9 The Global Compact for Safe, Orderly and Regular Migration (Objective 6) and The IOM emphasise fair and ethical recruitment to ensure decent work.10^,^11 Moreover, a recent commentary has highlighted the critical need to address labour exploitation in the global workforce.12
Although the Asia–Pacific region accounts for 16.2% of the global migrant workforce,1 most research on migrant workers' health has focused on the USA and Europe. This evidence gap limits the development of effective, region-specific health policies for migrant workers. Studies from parts of Asia have reported mental health risks and limited healthcare access among migrant workers, but these findings remain fragmented, without comprehensive regional synthesis.13^,^14 Similarly, research from the Greater Mekong Subregion has highlighted substantial health risks linked to limited access to healthcare services.15 Despite the region's scale of labour migration, systematic reviews that consolidate evidence across Asia–Pacific countries are lacking, in contrast to those available for Europe and the USA. Evidence on the health of their transnational families left behind in countries of origin, is also sparse and has largely focused on left-behind children in China, primarily within the context of internal rather than international labour migration.5
To address this gap, we conducted a systematic review and meta-analysis on the health of migrant workers and their transnational families in the Asia–Pacific. We examined work-related health outcomes and quantified morbidity prevalence and relative risks to inform policies on occupational safety and healthcare access.
Methods
Search strategy and inclusion criteria
We systematically searched Embase, MEDLINE, Ovid Global Health, and PsychINFO for primary studies published between Jan 1, 2013, and April 1, 2024. The starting year was chosen because the International Labour Organization (ILO) provides Asia–Pacific regional estimates of international migrant workers only from 2013 onwards, allowing our review to align with the most recent period of comparable labour migration data. Studies were eligible if they reported health outcomes among international migrant workers or their transnational families within the Asia–Pacific region. No language restrictions were applied. A Boolean search strategy was developed by RCL based on previous literature,2^,^4^,^5 and subsequently refined by SH. The full search strategy is provided in Appendix pp 1–2. In addition, grey literature and non-English studies were manually searched using key terms in Google Scholar, Google Search, and websites of relevant international and regional organisations, including WHO, IOM and ILO.
International migrant workers were defined according to the UN Convention on the Protection of the Rights of All Migrant Workers and Members of Their Families,16 as individuals engaged in remunerated work in a country where they are not nationals, regardless of documentation status. Eligible studies included those reporting on international migrant workers who originated from and were employed within the Asia–Pacific region, as defined by the United Nations regional classification,17 with the addition of Taiwan, encompassing a total of 56 countries and territories (Appendix p 3). Transnational families were defined as households in which at least one member was employed overseas (with no geographical restriction on the country of employment), while the remaining family members resided in their country of origin within the Asia–Pacific region. This group included left-behind children, stay-behind spouses, older adults, and caregivers. We included all types of primary research designs as long as they reported empirical data. However, studies that combined migrant and local workers, or international and internal migrant households, were excluded unless data were disaggregated and reported separately. Health outcomes for international migrant workers were defined as morbidity and mortality linked to their occupation, work environment, or workplace exposures. For transnational families, health outcomes referred to morbidity and mortality associated with the migration of family members employed abroad.
Titles and abstracts of English-language primary studies were screened by four reviewers (RCL, KL, KM, NR). Grey literature and non-English studies were manually searched and screened by five reviewers (RCL, KL, MS, CK, AI). All records were independently screened by two reviewers using the web-based application Rayyan,18 with discrepancies resolved by consensus.
The review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.19 This study is registered with PROSPERO, number CRD42024528561.
Data analysis
Full-text articles were screened and data extracted by one reviewer (RCL), with cross-verification by another (KL, KM). Discrepancies were resolved through discussion. We extracted data on study design, population, location, employment sector, working conditions, and health outcomes. To avoid duplication, when multiple publications reported on the same outcomes in the same population, only the most comprehensive study was included in the meta-analysis.
Studies were categorised based on their health focus through a narrative synthesis of health outcomes, accompanied by a descriptive analysis of these outcomes and associated factors. Comparisons between migrant and local workers, and between transnational and non-migrant families, were made where data permitted. Health risks among migrant workers and their transnational families were integrated into a multi-layered conceptual framework.
We used a random-effects model in R (version 4.4.2) to calculate pooled morbidity prevalence and 95% confidence intervals among migrant workers and transnational families. Forest plots were generated for both prevalence and relative risk estimates, the latter based on studies with comparator groups (local workers or non-migrant households). Heterogeneity was assessed using the I^2^ statistic. The use of a random-effects model was guided by narrative synthesis indicating substantial heterogeneity across study characteristics. Sensitivity analyses excluded studies rated as low or average quality to assess robustness of pooled estimates.
The quality of included studies was assessed using the Joanna Briggs Institute Checklist for Prevalence Studies,20 which evaluates risk of bias, methodological rigour, and reporting transparency. Studies scoring less than 50% were classified as low quality, 50–70% as average quality, and above 70% as high quality. For mixed-methods studies, quality was assessed using an integrated approach combining criteria for cross-sectional and qualitative studies. No studies were excluded based on quality; however, quality ratings informed the interpretation of study findings. All studies were independently assessed by one reviewer (RCL) and cross-checked by another (KL, KM, MS, MB, BO, CK, AI), with discrepancies resolved by consensus.
Role of funding source
The funder of the study had no role in study design, data collection, data analysis, data interpretation, writing of the report, or the decision to submit for publication. All authors had full access to all study data and were responsible for the decision to submit for publication.
Results
Characteristics of included studies
A total of 2877 publications were identified, of which 1113 were duplicates. After removal, 1764 articles were screened by title and abstract. Of these, 351 were selected for full-text review, and 54 studies were included in the final analysis (Fig. 1). These studies collectively included data from 86,620 individuals, comprising 64,172 migrant workers and 22,448 transnational family members. The characteristics of the included studies are summarised in Table 1. Of these, 48 were peer-reviewed articles published in English,21, 22, 23, 24^,^26, 27, 28, 29, 30, 31, 32, 33, 34, 35^,^37, 38, 39, 40, 41, 42, 43^,^45, 46, 47, 48^,^50, 51, 52, 53, 54, 55, 56, 57, 58, 59, 60^,^62, 63, 64, 65, 66, 67, 68^,^70, 71, 72, 73, 74 while four were published in Japanese,25 Korean,36 traditional Chinese,49 and simplified Chinese.61 Two reports—one from ILO44 and one from the IOM69—were also included.Fig. 1. Study selection.Table 1. Characteristics of included studies on migrant workers and transnational families in the Asia–Pacific region.StudyYearCountry of origin (migrant worker)Sex ratio (%) (male/female)Employment sectorHealth outcomeStudy designQuality scorea (%)Aryal et al.212019Nepal0/100Not applicableGynaecological diseases, depressionCross-sectional63Aryal et al.222020Nepal0/100Not applicableDepressionCross-sectional75Amit et al.232020Philippines70/30ManufacturingMusculoskeletal disordersCross-sectional63Asri and Chuang242023Indonesia47/53UnknownDepressionCross-sectional88Aida et al.252023Indonesia, Vietnam, Philippines, etc.56/44Nursing, manufacturing, processing, constructionMixed health outcomesCase series90Cheung et al.262019Philippines0/100Domestic workerDepressionCross-sectional75Chen and Luo272023Thailand93/7ManufacturingMusculoskeletal disordersCross-sectional88Dutta282017BangladeshNot availableConstructionOccupational injuries and illnessesQualitative study80Gao et al.292014Indonesia0/100DomesticDental cariesCross-sectional100Graham et al.302015Indonesia, Vietnam, Philippines32/68Not applicableCommon Mental DisordersMixed methods72Hall et al.312019Philippines0/100Domestic workerDepression and anxietyCross-sectional88Hall et al.322019Philippines0/100Domestic workerMixed health outcomesQualitative study70Hnuploy et al.332019Myanmar58/42Manufacturing, agriculture, fishing, construction, service, domestic workerDepressionCross-sectional88Habib et al.342020Syria52/48Agriculture, construction, manufacturingMusculoskeletal disordersCross-sectional100Habib et al.352021Syria52/48Agriculture, construction, manufacturingOccupational injuries and illnessesCross-sectional100Jo et al.362009China, Sri Lanka, Bangladesh, Myanmar, etc.78/22Manufacturing, construction, service, care workerMusculoskeletal disordersCross-sectional100Jayatissa and Wickramage372016Sri Lanka53/47Not applicableStunting, wasting and underweightCross-sectional88Knipe et al.382019Sri LankaNot availableNot applicableSuicide attemptCohort study64Kesornsri et al.392019Myanmar56/44Manufacturing, fishing and processingDepression and anxietyCross-sectional88Kang et al.402019China, Indonesia, Vietnam, Philippines87/13FishingMixed health outcomesCase series60Kunwar et al.412020Nepal53/47Not applicableStunting, wasting and underweightCross-sectional100Kim et al.422022Vietnam, Cambodia44/56General worker, service, agricultureDepressionCross-sectional100Kwon et al.432023Vietnam100/0Agriculture, construction, fishing, manufacturingMixed health outcomesCross-sectional50Lee et al.442011China, Vietnam, Sri Lanka, Indonesia, etc.30/70Construction, manufacturingOccupational injuriesNarrative text100Lee et al.452015China64/36Domestic, service, manufacturing, constructionOccupational injuries and illnessesCross-sectional63Lee et al.462016China0/100Not availableCardiovascular diseasesCross-sectional65Labao et al.472018Philippines10/90Domestic worker, service, manufacturingMusculoskeletal disordersCross-sectional75Lee and Cho482019China81/19Manufacturing, construction, agriculture, serviceOccupational injuries and deathCase series90Liu et al.492023Taiwan69/31Agriculture, manufacturing, construction, serviceMixed health outcomesCross-sectional100Meyer et al.502016Myanmar33/66Agriculture, manufacturing, sex workerDepression, anxietyCross-sectional100Mohammed and Kosalram512022India100/0Construction, skilled worker, serviceDiabetes, Cardiovascular diseasesCross-sectional50Nakagawa et al.522021Cambodia22/78Food processingParasite infectionCase report100Palupi et al.532017Indonesia0/100Domestic workerFatigue, depressionCross-sectional100Pradhan et al.542019NepalNot availableConstructionCardiovascular diseasesCase series30Paudya et al.552020NepalNot availableNot availableMixed health outcomesSystematic review64Santos et al.562015Sri Lanka, Indonesia, India, Napal, etc.48/52ManufacturingMusculoskeletal disordersCross-sectional63Siriwardhana et al.572015Sri Lanka27/73Not applicableCommon Mental DisordersCross-sectional100Soe et al.582015Myanmar32/68ManufacturingMusculoskeletal disordersCross-sectional100Sato et al.592019Indonesia20/80NursingMental health problemCross-sectional75Shah et al.602020India, Pakistan, Bangladesh100/0Manual labour, driver, office workDiabetesCross-sectional88Su et al.612021China96/4Construction, office workMusculoskeletal disordersCross-sectional88Spitzer et al.622023Indonesia, Philippines0/100Domestic workerMixed health outcomesQualitative90Sucipto et al.632023IndonesiaNot availableNot applicableStunting, malnutrition, mental health problemsCross-sectional40Sumerlin et al.642024Indonesia, Philippines0/100Domestic workerDepression and anxietyCross-sectional100Thetkathuek and Jaide652017Cambodia58/42AgricultureOccupational injuries and illnessesCross-sectional63Thetkathuek et al.662018Cambodia58/42AgricultureMusculoskeletal disordersCross-sectional88Thetkathuek et al.672020Cambodia61/39AgricultureOccupational injuries and illnessesCross-sectional100Wickramage et al.682015Sri-Lanka40/60Not applicableUnderweight, mental health problemsCross-sectional88Wickramage et al.692015Bangladesh, India, Indonesia, Nepal, etc.Not availableNot applicableUnderweight, psychiatric diagnosis, Common Mental DisordersNarrative text100Wongsanuphat et al.702019MyanmarNot availableManufacturingMeaslesCross-sectional63Winata and McLafferty712023Indonesia0/100Domestic workerMixed health outcomesMixed methods78Yi et al.722019Philippines0/100Domestic workerGambling disorderCross-sectional100Yi et al.732021Bangladesh, India, China, MyanmarNot availableConstruction, manufacturing, skilled workerOccupation-related illnesses, body pains, cold-like symptomsCross-sectional50Zerguine et al.742018Indonesia, Bangladesh, Pakistan, etc.100/0ConstructionWork-related injuriesCross-sectional63aStudy quality was evaluated utilising a 100 percent scale: <50% were defined low quality, 50–70% were average, and <70 as high quality.
Of the 54 included studies, 39 (72%)21, 22, 23, 24^,^26^,^27^,^29, 30, 31^,^33, 34, 35^,^37^,^39^,^41^,^43^,^45^,^47^,^49^,^51^,^53^,^56, 57, 58, 59^,^61^,^64, 65, 66, 67^,^70^,^72, 73, 74 were cross-sectional. Most were high quality, with a median quality score of 88%, with 37 (69%) rated as high, and only two rated low. One case series received a score of 30%, due to unclear reporting of the participants' health conditions.54 Another qualitative study scored 40%, largely because of unclear linkages between the research methodology, study population, and analytical approach.63 Detailed quality assessment scores are presented in Table 1.
Of the 54 included studies, 44 articles23, 24, 25, 26, 27, 28, 29^,^31, 32, 33, 34, 35, 36^,^39^,^40^,^42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55, 56^,^58, 59, 60, 61, 62^,^64, 65, 66, 67^,^70, 71, 72, 73, 74 focused on labour migration, while 10 articles21^,^22^,^30^,^37^,^38^,^41^,^57^,^63^,^68^,^69 examined transnational families. Data were collected across 17 countries and territories. Among the 54 included studies, 51 reported study locations, with nearly equal distribution between high-income countries (24 studies; 47%) and middle-income countries (27 studies; 53%). The study locations included: Thailand (n = 8),33^,^39^,^50^,^58^,^65, 66, 67^,^70 Korea (n = 7),23^,^36^,^42^,^43^,^45^,^46^,^48 Sri Lanka (n = 5),37^,^38^,^57^,^61^,^68 Hong Kong (n = 4),26^,^30^,^64^,^65 Malaysia (n = 4),47^,^56^,^62^,^74 Taiwan (n = 4),24^,^27^,^40^,^53 Nepal (n = 4),21^,^22^,^41^,^55 Japan (n = 3),25^,^52^,^59 Macao (n = 3),31^,^32^,^72 Lebanon (n = 2),34^,^35 India (n = 1),51 Indonesia (n = 1),63 Qatar (n = 1),54 Singapore (n = 1),73 United Arab Emirates (n = 1),60 and Vietnam (n = 1).49 One additional study30 reported multiple locations across Indonesia, the Philippines, and Vietnam. The classification of income groups was based on World Bank standards.75
The included studies indicated that migration primarily flowed from middle-income to high-income countries. Among the 18 labour-sending countries, 16 were classified as middle-income, while 12 of the 17 labour-receiving countries were high-income. Notably, five countries—Taiwan, Thailand, Malaysia, Vietnam, and Sri Lanka—functioned as both labour-sending and -receiving countries, reflecting the dynamic and bidirectional nature of labour mobility in the region. Details of these classifications are summarised in Table 2.Table 2. Labour migration flow in the Asia–Pacific region, classified by country role and World Bank income group.Labour-sending countries (n = 18) High income (n = 1)Taiwan Middle income (n = 16)Bangladesh, Cambodia, China, India, Indonesia, Kazakhstan, Malaysia, Mongolia, Myanmar, Nepal, Pakistan, Philippines, Sri Lanka, Thailand, Uzbekistan, Vietnam Low income (n = 1)SyriaLabour-receiving countries (n = 17) High income (n = 12)Oman, Bahrain, Hong Kong, Japan, Korea, Kwait, Macao, Saudi Arabia, Singapore, Taiwan, United Arab Emirates, Qatar Middle income (n = 5)Lebanon, Malaysia, Sri Lanka, Thailand, VietnamLabour-sending and receiving countries (n = 5) High income (n = 1)Taiwan Middle income (n = 4)Thailand, Malaysia, Sri Lanka, VietnamCountries included in the search strategy but not listed here (e.g. Tonga, Yemen) had no eligible studies identified.
Migrant workers in this region were predominantly male (43,117 [71%]). More than 75% were employed in manufacturing (19,056 [35%]), construction (15,424 [28%]), and service sectors (7629 [14%]) including drivers, restaurant workers, car washers and sales assistants. Other sectors included agriculture (6762 [12%]) and domestic work (3834 [7%]).
Health issues of migrant workers
Among the 44 studies on migrant workers, seven key health focus areas were identified: mental health (n = 11),24^,^26^,^31^,^33^,^39^,^42^,^50^,^53^,^59^,^64^,^72 musculoskeletal disorders (MSDs) (n = 9),23^,^27^,^34^,^36^,^47^,^56^,^58^,^61^,^66 mixed health outcomes (referring to studies that concurrently examined a range of physical and psychological health issues) (n = 8),25^,^32^,^40^,^43^,^49^,^55^,^62^,^71 occupational injuries and illnesses (n = 8),28^,^35^,^44^,^45^,^48^,^65^,^67^,^74 diabetes and cardiovascular diseases (CVDs) (n = 4),46^,^51^,^54^,^60 infectious diseases (n = 3),52^,^70^,^73 and oral health (n = 1).29
Occupational injuries and illnesses exhibited the highest prevalence, affecting 45,661 migrant workers (88%) who reported at least one work-related morbidity in our review. Of note, 85% of these cases were reported in a single study of Chinese migrant workers in South Korea.48 When this study was excluded, occupational injuries and illnesses remained the most frequently reported health condition, affecting 3572 individuals. The most common type of occupational injury was cuts and wounds (n = 955). Other major reported health conditions included mental health issues (1975 [3.8%]), MSDs (1973 [3.8%]), and diabetes and CVDs (745 [1.4%]). Two studies reported migrant worker mortality, including 353 deaths caused by collisions48 and 571 deaths attributed to CVDs.54
Through thematic analysis of reported health risks, we categorised these into six interrelated levels—personal, familial, occupational, social, environmental, and structural—illustrating the complex, multi-layered determinants of health among migrant workers (Fig. 2). Among these, occupational factors were the most pervasive and consistently reported source of risk. Three key occupational factors—long working hours, workplace hazards, and precarious employment—were most frequently cited as contributing to multiple and overlapping health burdens among migrant workers.Fig. 2. Health risk factors of migrant workers and transnational families in the Asia–Pacific region. References: Medical care barrier26^,^32^,^36^,^44^,^70; Restriction to change workplace44^,^48; Maladjustment in host countries25^,^38^,^46^,^49; Change in lifestyle due to acculturation60; Living environment28^,^30^,^70^,^73; Perceived social discrimination31; Social support26^,^42^,^44^,^56^,^72; Working hours24^,^26^,^28^,^39^,^41^,^54^,^55^,^62, 63, 64^,^66, 67, 68^,^71; Workplace hazards35^,^43^,^45^,^48^,^51^,^54^,^55^,^66^,^74; Working conditions26^,^28^,^48^,^50^,^52^,^62^,^70; Ergonomic risks25^,^33^,^43^,^50^,^59^,^60^,^73; Overseas remittance22^,^30^,^41^,^57^,^68; Contact with family22^,^24^,^56; Consumption of raw food55; Education and health literacy.37^,^57^,^63
Long working hours, including overwork, lack of breaks, and no rest days—were cited in 14 studies.24^,^28^,^33^,^49^,^51^,^54^,^56^,^58^,^62^,^64, 65, 66, 67^,^71 These conditions were associated with increased risks of mental health issues,24^,^33^,^64 MSDs,56^,^58^,^66 diabetes and CVDs,51^,^54 mixed health outcomes,49^,^62^,^71 and occupational injuries and illnesses.28^,^65^,^67 Workplace hazards including exposure to heat, chemicals, dust, sharp or heavy objects, collisions, and lack of protective equipment were described in 11 studies.35^,^43, 44, 45^,^48^,^51^,^54^,^56^,^65^,^67^,^74^,^ These hazards contributed to MSDs,56 mixed health outcomes,43 diabetes and CVDs,51^,^54 and occupational injuries and illnesses.35^,^44^,^45^,^48^,^65^,^67^,^74 Precarious working conditions, including physical and verbal abuse, job stress, and lack of workplace control, were reported in seven studies.26^,^28^,^35^,^42^,^50^,^56^,^62 These factors were associated with increased risks of mental health issues,26^,^42^,^50 MSDs,56 mixed health outcomes,62 and occupational injuries and illnesses.28^,^33 Barriers to medical care were identified in five studies.26^,^32^,^36^,^44^,^70 These barriers were associated with worsen health conditions, including MSDs,36 measles infection,70 mixed health outcomes,32 and occupational injuries and illnesses.28^,^44
Together, these findings underscore the multifaceted and interlinked nature of occupational determinants, which expose migrant workers not only to direct physical and psychological harm but also to chronic health inequalities driven by excessive labour demands, hazardous environments, and systemic barriers to care.
Health issues of transnational families
Ten studies on transnational families included left-behind children, stay-behind spouses, older adults, and caregivers with some examining multiple generations. Three main health focus areas were identified: mental health (n = 4),22^,^30^,^38^,^57 malnutrition (n = 2),37^,^41 and mixed health outcomes involving both mental health and nutritional status (n = 4).21^,^63^,^68^,^69 In total, 50.1% reported mental health issues—including anxiety, depression, suicide attempts, and other common disorders (n = 1520)—and 30.4% reported malnutrition, including stunting, wasting, and underweight (n = 954).
The health of transnational families was associated with the frequency of remittances from migrant workers22^,^30^,^41^,^57^,^68 and their own education levels.37^,^57^,^63 Given the interconnected health fluctuations between transnational families and migrant workers, these factors could be incorporated into the framework of multiple risk factors affecting migrant workers (Fig. 2).
Meta-analysis: work-related morbidity of migrant workers
The meta-analysis of work-related morbidity among migrant workers included data from 18,019 individuals across 30 studies.23^,^24^,^26^,^27^,^29^,^31^,^33^,^35^,^36^,^39^,^40^,^42^,^43^,^45^,^47^,^49^,^53^,^56^,^58, 59, 60, 61^,^64, 65, 66, 67^,^71, 72, 73, 74 The pooled prevalence of reporting at least one work-related morbidity was 37% (95% CI 27–47; I^2^ = 99.0%; Fig. 3), indicating that more than one in three migrant workers experience work-related health problems. Of the 30 studies, four were included in the meta-analysis of relative risk, selected based on methodological homogeneity in employment sectors and health outcomes. Based on four studies27^,^40^,^49^,^61 involving 1256 migrant workers and 9724 local workers, the pooled relative risk of work-related morbidity was 1.29 (95% CI: 1.10–1.52; I^2^ = 47.4%; Fig. 4), suggesting that migrant workers are about 30% more likely to report morbidity compared with native workers.Fig. 3. Forest plot of prevalence of having at least one reported work-related morbidity among migrant workers in the Asia–Pacific region.Fig. 4. Forest plot of relative risk of having at least one reported work-related morbidity among migrant workers compared with local workers.
Meta analysis: morbidity of transnational families
A total of 23,933 transnational family members from eight studies21^,^22^,^30^,^37^,^38^,^41^,^57^,^68 were included in the meta-analysis. The pooled prevalence of reporting at least one morbidity, including mental health conditions and malnutrition, associated with labour migration was 23% (95% CI: 7–53; I^2^ = 99.7%; Fig. 5), highlighting a substantial health burden among left-behind family members. To compare health outcomes between transnational families and non-migrant households, a separate meta-analysis was conducted using five studies,21^,^37^,^38^,^41^,^68 selected based on comparable characteristics in country of origin and health outcome focus. The pooled relative risk was 1.12 (95% CI: 0.95–1.33; I^2^ = 86.4%; Fig. 6), indicating only a modest and statistically non-significant elevation in morbidity among transnational families.Fig. 5. Forest plot of prevalence of having at least one reported morbidity associated with labour migration among transnational families in the Asia–Pacific region.Fig. 6. Forest plot of relative risk of having at least one reported morbidity associated with labour migration among transnational families compared with non-migrant households.
Sensitivity analyses assessed the impact of study quality on pooled estimates. Among migrant workers, excluding low and average quality studies yielded a prevalence of 33% (95% CI: 0.23–0.45; I^2^ = 98.9%) and a relative risk of 1.32 (95% CI: 1.01–1.74; I^2^ = 64.9%), consistent with main findings (Appendix pp 4–5). For transnational families, the pooled prevalence was 21% (95% CI: 0.13–0.30; I^2^ = 94.4%), and the relative risk compared with non-migrant households was 1.03 (95% CI: 0.83–1.27; I^2^ = 74.1%), showing no notable deviation (Appendix pp 6–7).
Discussion
This large multi-country dataset identified substantial occupational health risks among international migrant workers in the Asia–Pacific region. Long working hours, hazardous conditions, precarious employment, and limited healthcare access were consistently associated with musculoskeletal disorders, occupational injuries, depression, gambling disorders, and cardiovascular disease. Although some studies support the “healthy migrant effect,”4^,^27 this advantage diminishes over time due to cumulative exposure to occupational and structural stressors.26^,^49^,^54^,^61^,^70^,^72
Our findings align with global reviews reporting high occupational morbidity among migrant workers,2, 3, 4 though our pooled prevalence (37%) was slightly lower—likely due to underreporting and limited disclosure.4^,^5 The relative risk (1.29) was consistent with global estimates,3 but the absence of regional mortality data limited comparisons for fatal injuries. For example, during a measles outbreak in Korea, migrant workers had twice the attack rate of local workers (1.4% vs 0.7%), attributed to lower vaccination coverage (11.6% vs 36.7%).70
For transnational families, findings indicate elevated risks of mental health issues and undernutrition, in line with global reviews of left-behind children.5^,^6 However, the pooled relative risk (1.12) was only marginally elevated, possibly reflecting differences in population composition and limited disaggregated data. Many studies included not only children, but also spouses and older adults. Emotional strain and irregular remittances were key contributors to poor health outcomes.22^,^30^,^41^,^57^,^62^,^68 Some studies that combined internal and international migrant households were excluded from our analysis due to the lack of disaggregated data. For example, a cross-sectional study from Cambodia reported higher morbidity among both adult members and left-behind children in migrant families compared to non-migrant households.76 Although not eligible for inclusion in the meta-analysis, such evidence underscores the potential health vulnerabilities of transnational family members and may partly explain why the pooled relative risk in our review was only modestly elevated.
This review provides the first region-specific morbidity estimates based on multilingual evidence. However, most included studies were cross-sectional and relied on self-reported data. Female migrant workers beyond the domestic sector were also underrepresented. This underrepresentation is evident when compared with ILO estimates, which show that male and female migrant workers contribute nearly equally to the labour force in the Asia–Pacific region,1 whereas men accounted for 71% of participants in our included studies. Publication bias cannot be excluded, and substantial heterogeneity reflects differences in study populations and outcome measures. While this limits the precision of pooled estimates, forest plots were retained to illustrate the overall distribution and direction of effects across the region. Beyond these methodological considerations, it is also important to note that while occupational factors were the most consistently reported and therefore emphasised as key contributors in the main text, our thematic analysis (Fig. 2) also highlighted other contextual risks such as living conditions. For example, limited facilities in migrant worker housing have been linked to COVID-19 exposure risks in Singapore.73
These health burdens stem not from migration itself, but from inadequate protections—affecting both workers and their families across borders. Strengthening protections in both sending and receiving countries is therefore essential. Although 80% of Asia–Pacific countries have bilateral labour migration agreements, only 44% have implemented ethical recruitment measures, and fewer than half have mechanisms to safeguard the rights of their overseas workers.77 In the 2023 report on migration and health, the Association of Southeast Asian Nations (ASEAN) Secretariat called on member states to ensure health coverage for migrant workers by 2025, while at the same time acknowledging that workers continue to face substantial barriers to accessing care, including language difficulties, financial constraints, frequent changes in employment, and exclusion from local insurance systems.78 These contrasting messages underscore the urgent need for strengthened cooperation between labour-sending and labour-receiving countries.
Regional mechanisms already exist to facilitate such cooperation. For example, bilateral agreements between labour-sending and receiving countries in the Asia–Pacific have included explicit health protections for migrant workers. The Bangladesh–Qatar Agreement (2008) stipulates that employers must cover medical treatment free of charge for workers, while the Nepal–Jordan General Agreement (2017) requires employers to provide all necessary medical care.79 In addition, two active consultative processes in the region involve governments at different ends of the migration corridor: the Colombo Process, a forum of labour-sending countries in South and South-East Asia,80 and the Abu Dhabi Dialogue, which brings together Colombo Process countries of origin with Gulf Cooperation Council destination countries.81 These mechanisms provide platforms for dialogue and cooperation to promote the welfare and well-being of migrant workers. Our findings may contribute to evidence-based policy development within these regional frameworks to reduce the health risks associated with labour migration.
By 2023, the outflow of migrant workers from Asia–Pacific countries had risen by 33% from 2022, while inflows and migrant stocks in major destinations surpassed pre-pandemic levels.77 This trend underscores the region's growing dependence on migrant labour and the urgent need to protect worker health to sustain economic stability. Despite its central role in global labour migration, the Asia–Pacific remains underrepresented in global policy frameworks. Aligning national policies with WHO's Global Plan of Action, SDG 8.8, and the Global Compact for Safe, Orderly and Regular Migration can support regional action to improve safety, promote ethical recruitment, and expand healthcare access.
Ultimately, this review provides the first region-wide synthesis of migrant worker health in the Asia–Pacific, addressing a major evidence gap and highlighting substantial but preventable adverse health outcomes. Strengthening protections and closing policy gaps through coordinated regional action, involving governments, health services, and employers, is essential to safeguard the health of both migrant workers and their families, with direct implications for sustainable economic development.
Contributors
SH and RCL conceived the study. RCL developed the protocol with input from KL, KM, UT, AK, CZ, and SH. RCYL conducted the database search, abstract screening, data extraction, and quality appraisal, which were cross-verified by KL, KM, NRM, MS, MB, BO, CK, and AI. RCL performed the data analysis and drafted the manuscript, with contributions from all authors.
Data sharing statement
No additional data are available.
Declaration of interests
We declare no competing interests.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1International Labour Organization ILO global estimates on international migrant workers: international migrants in the labour forcehttps://www.ilo.org/publications/major-publications/ilo-global-estimates-international-migrants-labour-force 2024
- 2Hargreaves S.Rustage K.Nellums L.B.Occupational health outcomes among international migrant workers: a systematic review and meta-analysis Lancet Global Health 72019 e 872e 8823112290510.1016/S 2214-109X(19)30204-9PMC 6565984 · doi ↗ · pubmed ↗
- 3Pega F.Govindaraj S.Tran N.T.Health service use and health outcomes among international migrant workers compared with non-migrant workers: a systematic review and meta-analysis P Lo S One 1662021 e 025265110.1371/journal.pone.0252651 PMC 818951234106987 · doi ↗ · pubmed ↗
- 4Lau K.Aldridge R.Norredam M.Workplace mortality risk and social determinants among migrant workers: a systematic review and meta-analysis Lancet Public Health 9112024 e 935e 9493948690810.1016/S 2468-2667(24)00226-3PMC 11868777 · doi ↗ · pubmed ↗
- 5Fellmeth G.Rose-Clarke K.Zhao C.Health impacts of parental migration on left-behind children and adolescents: a systematic review and meta-analysis Lancet 392101642018256725823052847110.1016/S 0140-6736(18)32558-3PMC 6294734 · doi ↗ · pubmed ↗
- 6Antia K.Boucsein J.Deckert A.Effects of international labour migration on the mental health and well-being of left-behind children: a systematic literature review Int J Environ Res Public Health 1712202043353256044310.3390/ijerph 17124335 PMC 7345580 · doi ↗ · pubmed ↗
- 7Dominguez G.B.Hall B.J.The health status and related interventions for children left behind due to parental migration in the Philippines: a scoping review Lancet Reg Health West Pac 28202210056610.1016/j.lanwpc.2022.100566 PMC 939157335996696 · doi ↗ · pubmed ↗
- 8WHOWHA A 60/26 workers' health: global plan of actionhttps://apps.who.int/gb/ebwha/pdf_files/WHA 60/A 60_R 26-en.pdf