King Kong Pox: A Case of Severe Mpox and Bartonella Co-infection in a Patient Living With Human Immunodeficiency Virus (HIV)
Anurag Karki, Ashirbad Acharya, Suraj Shrestha, Puja Thapa, Yogesh Pandey, Ricardo Conti, Lindsay Lim

TL;DR
A patient with HIV and a very low immune system had severe Mpox and co-infections, showing the importance of timely treatment and managing all infections.
Contribution
This case highlights the complex interplay between Mpox, HIV, and co-infections in immunocompromised individuals.
Findings
The patient had severe Mpox with widespread necrotic lesions despite treatment.
Co-infections with Bartonella and Cytomegalovirus were identified.
The case emphasizes the need for managing both Mpox and underlying HIV along with co-infections.
Abstract
Mpox, formerly monkeypox (MPXV), is a zoonotic virus that has emerged globally in recent times, disproportionately affecting immunocompromised individuals, particularly people living with human immunodeficiency virus (HIV) (PWH). PWH with advanced HIV and low CD4 counts are at higher risk for severe, prolonged courses and sometimes fatal Mpox infections, which may often be complicated by bacterial superinfections and opportunistic co-infections. We present a case of Mpox in a PWH with an initial CD4 count of 2 cells/μL and a high HIV viral load, who had worsening disease despite treatment with tecovirimat, raising the question of persistent/resistant Mpox. Further investigations revealed co-infections with Bartonella and Cytomegalovirus (CMV), adding to the case's complexity. He initially presented with high-grade fever, and multiple, large necrotic lesions were noted on his face,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
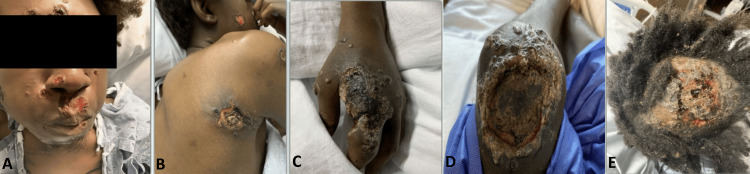 Figure 1
Figure 1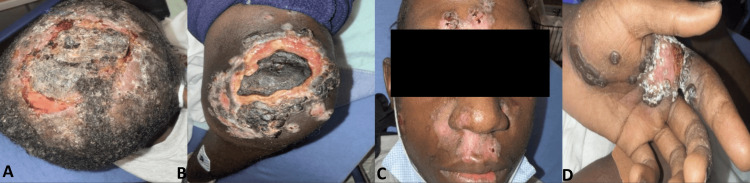 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPoxvirus research and outbreaks · Bartonella species infections research · Bacillus and Francisella bacterial research
Introduction
Mpox (formerly monkeypox) virus (MPXV) is a zoonotic disease historically confined to regions of Africa, with limited human-to-human transmission before 2022 [1,2]. The 2022-2023 global outbreaks marked a shift, with over 90% of confirmed MPXV cases occurring among gay, bisexual, and other men who have sex with men (MSM), a population at high risk for both MPXV and human immunodeficiency virus (HIV) [3]. People living with HIV (PWH), specifically those with CD4 T-cell counts less than 100 cells/μL and untreated advanced HIV, are disproportionately affected, which includes around 40-50% of Mpox cases, and they experience more prolonged and potentially lethal disease [4-6]. They also often present with bigger skin lesions, bacterial superinfections, and protracted illness [7,8]. Co-infections with opportunistic pathogens, such as *Bartonella *and *Cytomegalovirus *(CMV), further complicate the clinical course, especially in severely immunocompromised patients not on anti-retroviral therapy (ART) [5,6].
The following case of PWH with worsening Mpox despite treatment highlights a few challenges, such as persistent/resistant MPXV, opportunistic co-infections with Bartonella and CMV, and possible immune reconstitution inflammatory syndrome (IRIS).
Case presentation
A 24-year-old African American MSM, living with HIV but not adherent to ART, presented to the emergency department (ED) of our hospital with worsening Mpox lesions. He was initially diagnosed with Mpox via polymerase chain reaction (PCR) two months prior at another facility where he had presented with small necrotic lesions on his hands and face and had completed a two 14-day course of tecovirimat. Despite his initial therapies, his condition had deteriorated with new lesions and high-grade fevers with occasional anal bleeding, prompting presentation to our hospital. On examination, he had multiple large, necrotic lesions on his face, scalp, left hand, knee, back, rectum, and genitalia, some of which are shown in Figure 1.
Disseminated ulcerative and necrotic skin lesions.(A) Facial involvement with multiple ulcerative nodules, especially around the nose and mouth, with presence of hemorrhagic crusts. (B) Well-defined ulcers, core necrosis, and surrounding erythema on the posterior shoulder. (C) A large ulcer with black eschar and surrounding pustules on the dorsum of the hand. (D) Lesion on the left knee with central necrosis and a thick hyperkeratotic border. (E) Scalp ulcer with hemorrhagic crusts and necrotic tissue on top.
Repeated MPXV PCR tests confirmed persistent infection. His initial CD4 count was 2 cells/μL (normal range: 500-1600 cells/μL), with an HIV viral load of 687,000 copies/mL. Due to the severity of his condition, the case was discussed with the Centers for Disease Control and Prevention (CDC). After completing a two-week course of IV tecovirimat, three doses of brincidofovir, and a single dose of vaccinia immunoglobulin (VIGIV), the patient showed gradual improvement with no new lesions. ART was initiated during his prior admission, but he was unable to continue it as an outpatient. ART was reintroduced. His initial CD4+ T-cell count of only 2 cells/μL and a significantly high HIV-1 viral load of 687,000 copies/mL indicated the patient's severe immunosuppression. Considering the severity of immunocompromised status, a thorough assessment for opportunistic infections was done. He had Bartonella henselae serology positive for IgG with a titer of 1:256 (normal range: less than 1:128) and IgM with a titer of 1:64 (normal range: less than 1:16), suggesting either a recent or chronic infection. The patient had also reported exposure to stray cats in the past. CMV DNA was also found in the blood with a viral load of 5,280 copies/mL (normally undetectable), which is also a prevalent opportunistic infection in individuals with advanced acquired immunodeficiency syndrome (AIDS). Treatment for both infections was initiated with appropriate antibiotics that included doxycycline and valganciclovir. His hospital course was further complicated by an extended-spectrum beta-lactamase (ESBL) Escherichia coli abscess underlying a necrotic knee lesion. After completing a two-week course of IV tecovirimat 200 mg twice daily, three doses of oral brincidofovir 200 mg, and a single dose of VIGIV 6000 units, the patient showed gradual improvement with no new lesions as demonstrated in Figure 2. He was discharged with a four-week course of oral tecovirimat 600 mg twice daily and outpatient follow-up.
Improvements of Mpox lesions in various anatomical regions throughout time.(A) Scalp lesions exhibiting central crusting and resolving erythema at the periphery with partial re-epithelialization. (B) Desquamation and granulation tissue showing signs of healing in this ulcerated necrotic lesion on the left knee. (C) Facial lesions showing resolving erythematous plaques and crusting over the forehead and nasal bridge. (D) Left hand palmar aspect showing a healing ulcer with dry crusts and granulating base.
Discussion
The Mpox outbreak in 2022 found sexual contact as the primary route of transmission, with frequent anogenital lesions and co-occurring sexually transmitted infections (STIs) such as gonorrhea, syphilis, and chlamydia [4,5]. MPXV infects humans through mucosal or skin contact, leading to primary infections in the eyes, respiratory system, skin, or genital sites [9]. The virus can disseminate via lymphatic and vascular routes, causing lymphadenopathy and affecting organs such as the lungs, liver, and kidneys [9,10]. Bacterial superinfections, co-infections with HIV or STIs, worsen disease severity, prolong recovery, and increase morbidity and mortality [11].
While initial prodromal symptoms of Mpox are similar in PWH and those without HIV, PWH with advanced HIV and uncontrolled viremia experience more severe and prolonged cutaneous manifestations, often with mucosal involvement [5,12]. Compared to HIV-negative individuals, PWH are more likely to develop ano-rectal pain, bleeding, proctitis, peri-rectal abscesses, and phimosis, with advanced HIV increasing the risk of multi-organ involvement, including myopericarditis, encephalitis, colitis, pneumonitis, blepharoconjunctivitis, and keratitis [9,10,13]. In PWH with CD4 counts below 350 cells/μL, Mpox severity increases with declining immune function, particularly in those newly diagnosed with advanced HIV or not on ART [6,13,14]. A study in Atlanta found that PWH with uncontrolled HIV viral loads (>200 copies/mL) had 2.1 times higher odds of severe Mpox compared to those with suppressed viral loads [15]. Our patient had an exceptionally low CD4 count with a high viral load that had placed him at the highest risk for a prolonged and severe Mpox disease course. Bartonella henselae can also have widespread skin manifestations in advanced cases of HIV, most notably bacillary angiomatosis [16]. Our patient had positive serologies for Bartonella that were consistent with acute/recent infection; however, biopsy and Bartonella PCR from select lesions were negative. Workup was limited due to the sheer number of lesions, making it more difficult to definitively rule out bacillary angiomatosis. This co-infection had likely contributed to the initial treatment failure and prolonged course, which emphasizes the necessity of a comprehensive diagnostic workup for co-pathogens in severely immunocompromised Mpox patients.
No MPXV-specific antivirals are approved, but tecovirimat and brincidofovir, developed for smallpox, are used for Mpox treatment [17]. Tecovirimat has been the first-line therapy, with observational studies showing no significant difference in outcomes by HIV status [18,19]. Brincidofovir, a prodrug of cidofovir, may act synergistically with tecovirimat in severe cases, particularly in PWH with advanced HIV [20]. VIGIV provides cross-protective antibodies and may benefit immunocompromised patients [21]. In our case, we had to use all of the above three modalities, which then potentially led to improvement in his overall clinical status. This aggressive approach was ultimately necessary and beneficial in this context of severe immunosuppression and initial treatment failure.
Initiating ART can trigger Mpox-IRIS in PWH with advanced HIV, with 25% of such patients in a global case series developing suspected IRIS and a 57% mortality rate among those affected [5]. Despite this risk, early ART initiation is critical for immune reconstitution and MPXV clearance. Combination antiviral therapy is recommended for severe, progressive disease in such patients [22]. Persistent or recurrent Mpox in immunocompromised patients may indicate tecovirimat resistance, with studies identifying resistant isolates in patients with CD4 counts below 200 cells/μL who received multiple tecovirimat courses [5]. We had initial concerns for Mpox-IRIS, but ART was continued in this patient.
Conclusions
Mpox is an opportunistic infection that can cause severe disease in PWH, particularly those with advanced HIV, along with low CD4 counts. Timely diagnosis and treatment of both Mpox and underlying HIV, alongside management of co-infections, are critical for improving outcomes. Early ART initiation, antiviral therapy, and supportive care are essential, despite risks such as IRIS or antiviral resistance. Comprehensive care and vigilant monitoring can mitigate the severe manifestations of Mpox in this vulnerable population.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Virulence differences of Mpox (monkeypox) virus clades I, I Ia, and I Ib.1 in a small animal model Proc Natl Acad Sci U S A Americo JL Earl PL Moss B 0120202310.1073/pnas.2220415120 PMC 997450136787354 · doi ↗ · pubmed ↗
- 2Human monkeypox: an emerging zoonosis Lancet Infect Dis Di Giulio DB Eckburg PB 1525420041472056410.1016/S 1473-3099(03)00856-9PMC 9628772 · doi ↗ · pubmed ↗
- 3Clinical presentation and virological assessment of confirmed human monkeypox virus cases in Spain: a prospective observational cohort study Lancet Tarín-Vicente EJ Alemany A Agud-Dios M 66166940020223595270510.1016/S 0140-6736(22)01436-2PMC 9533900 · doi ↗ · pubmed ↗
- 4Monkeypox virus infection in humans across 16 countries - April-June 2022 N Engl J Med Thornhill JP Barkati S Walmsley S 67969138720223586674610.1056/NEJ Moa 2207323 · doi ↗ · pubmed ↗
- 5Mpox in people with advanced HIV infection: a global case series Lancet MitjàO Alemany A Marks M 93994940120233682800110.1016/S 0140-6736(23)00273-8 · doi ↗ · pubmed ↗
- 6Severe Mpox infections in people with uncontrolled human immunodeficiency virus Clin Infect Dis Govind A Lazarte SM Kitchell E 184318467620233671866210.1093/cid/ciad 052 · doi ↗ · pubmed ↗
- 7Outbreak of human monkeypox in Nigeria in 2017-18: a clinical and epidemiological report Lancet Infect Dis Yinka-Ogunleye A Aruna O Dalhat M 8728791920193128514310.1016/S 1473-3099(19)30294-4PMC 9628943 · doi ↗ · pubmed ↗
- 8The effect of HIV and Mpox co-infection on clinical outcomes: systematic review and meta-analysis HIV Med Taha AM Elrosasy A Mahmoud AM 8979092520243844331910.1111/hiv.13622 · doi ↗ · pubmed ↗