Overlap of Bickerstaff Encephalitis and Pharyngeal-Cervical-Brachial Variant of Guillain-Barré Syndrome Following COVID-19 Infection
Kosuke Okuma, Kentaro Hori, Shingo Kawakami, Yoko Suzuki

TL;DR
A woman developed neurological complications resembling two rare conditions after a COVID-19 infection and improved with immunotherapy.
Contribution
This case highlights the overlap of Bickerstaff brainstem encephalitis and a variant of Guillain-Barré syndrome following COVID-19.
Findings
The patient showed symptoms of Bickerstaff brainstem encephalitis and pharyngeal-cervical-brachial variant of Guillain-Barré syndrome.
Anti-GQ1b and anti-GT1a antibodies were detected, aiding in diagnosis.
Immunotherapy led to rapid improvement in neurological symptoms.
Abstract
A 36-year-old woman developed numbness in both fingers and unsteadiness around 10 days after COVID-19 infection. She was admitted to our hospital after experiencing drowsiness, dysarthria, and gait disturbance within three days. On admission, her vital signs were stable, with no signs of infection. Neurological examination revealed disturbances in consciousness, ophthalmoplegia, ataxia, pharyngeal and cervical muscle weakness, and sensory abnormalities predominantly affecting the upper extremities. Brain MRI and CSF examination revealed no abnormalities, whereas the median nerve somatosensory evoked potential indicated an intracranial conduction abnormality. Based on these findings, brainstem encephalitis of non-infectious origin was suspected, and IVIg and high-dose IV methylprednisolone therapies were initiated. Subsequent serological testing revealed the presence of serum anti-GQ1b…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
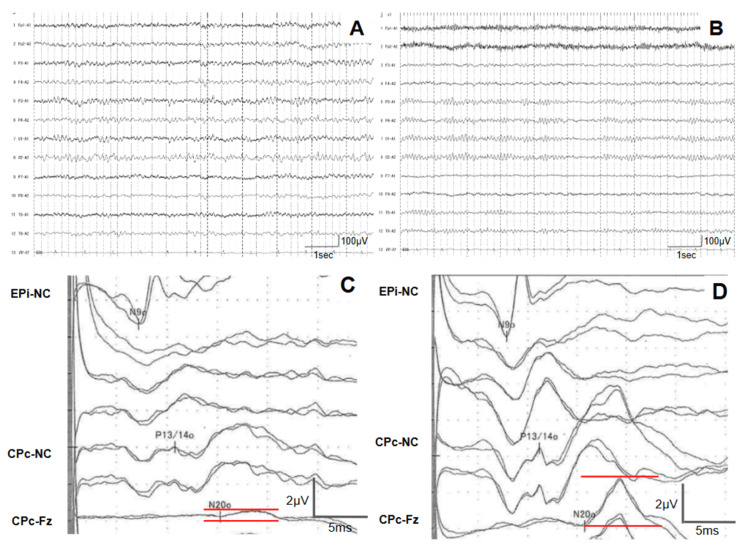 Figure 1
Figure 1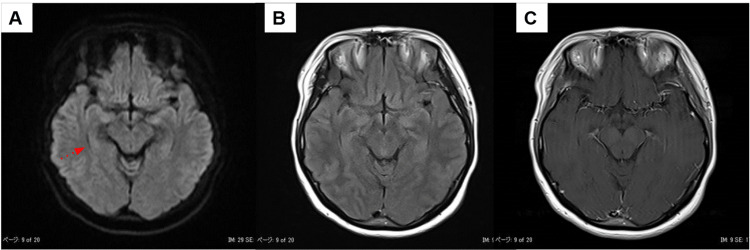 Figure 2
Figure 2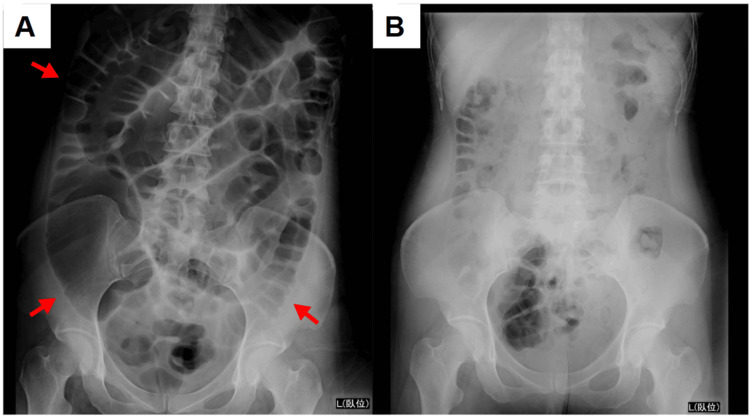 Figure 3
Figure 3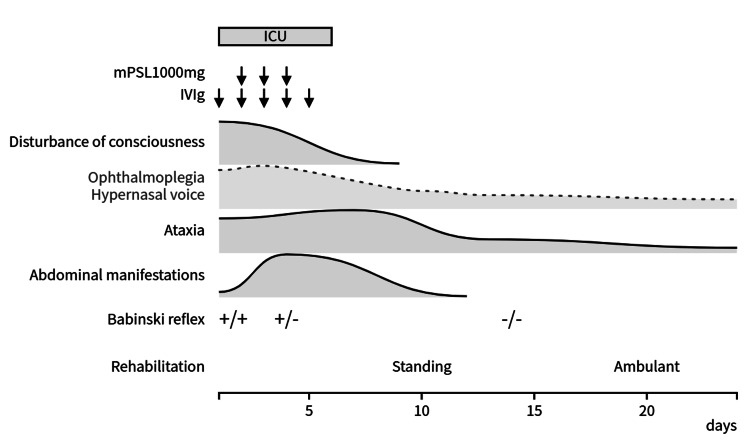 Figure 4
Figure 4| Laboratory test | Patient value | Normal range | Units |
| Complete blood count | |||
| White blood cell | 7,500 | 3,300-8,600 | /µL |
| Red blood cell | 539 | 386-492 | x10⁴/µL |
| Hemoglobin | 15.9 | 11.6-14.8 | g/dL |
| Hematocrit | 48.0 | 35.1-44.4 | % |
| Platelets | 33.4 | 15.8-34.8 | x10⁴/µL |
| Biochemistry test | |||
| C-reactive protein | 0.55 | <0.3 | mg/dL |
| Total protein | 8.5 | 6.6-8.1 | g/dL |
| Albumin | 4.3 | 4.1-5.1 | g/dL |
| Blood urea nitrogen | 14.5 | 8.0-20.0 | mg/dL |
| Creatinine | 0.47 | 0.46-0.79 | mg/dL |
| Total bilirubin | 0.8 | 0.4-1.5 | mg/dL |
| Aspartate aminotransferase | 16 | 13-30 | U/L |
| Alanine aminotransferase | 10 | 7-23 | U/L |
| Creatine kinase | 78 | 41-153 | U/L |
| Lactate dehydrogenase | 167 | 124-222 | U/L |
| Sodium | 138 | 138-145 | mEq/L |
| Potassium | 4.3 | 3.6-4.8 | mEq/L |
| Chloride | 99 | 101-108 | mmol/L |
| Glucose | 101 | 73-109 | mg/dL |
| Procalcitonin | 0.0 | <0.05 | ng/mL |
| Free T3 | 2.52 | 2.30-4.00 | pg/mL |
| Free T4 | 1.02 | 0.93-1.70 | ng/dL |
| Thyroid-stimulating hormone | 0.619 | 0.500-5.00 | µU/mL |
| Ammonia | 23 | 12-66 | µg/dL |
| Vitamin B1 | 40 | 23.1-81.9 | ng/mL |
| Coagulation test | |||
| PT-INR | 1.04 | ||
| APTT | 25.9 | 24.0-39.0 | s |
| D-dimer | 1.2 | <1.0 | µg/mL |
| Immunologic test | |||
| Antinuclear antibody (IFA) | <40 | <40 | |
| Rheumatic factor | 1.25 | <2.0 | |
| Anti-SS-A antibody | <1.0 | <10 | U/mL |
| Anti-SS-B antibody | 1.0 | <10 | U/mL |
| Anti-thyroglobulin antibody | <10.0 | <19.3 | U/mL |
| MPO-ANCA | <1.0 | <3.5 | U/mL |
| PR3-ANCA | 1.4 | <3.5 | U/mL |
| Serum anti-ganglioside antibody test (ELISA) | Interpretation (OD, blank subtracted) | ||
| IgG class anti-GM1 antibody | - (0.011) | ||
| IgG class anti-GQ1b antibody | ++ (0.889) | ||
| IgG class anti-GT1a antibody | ++ (0.940) | ||
| IgG class anti-GT1b antibody | - (0.018) | ||
| IgG class anti-GD1a antibody | - (0.016) | ||
| CSF test | |||
| Appearance:Clear, opening pressure:10 cm H₂O | |||
| Cell count | 2 | 0-5 | /µL |
| Protein | 44 | 10-40 | mg/dL |
| Glucose | 67 | 50-75 | mg/dL |
| HSV-DNA | <2x10² | <2x10² | copies/mL |
| VZV-DNA | <2x10² | <2x10² | copies/mL |
| Myelin basic protein | 127 | 0-102 | pg/mL |
| IgG index | 0.5 | <0.7 | |
| OCBs | - | - | |
| Literature | Age/sex | Onset interval | Initial symptoms | Complications | Serum antibodies | Treatment | Outcome |
| Llorente Ayuso L, et al. [ | 72 F | 28 days | Dizziness | – | GD1a | IVMP, followed by PO-PSL | Ambulatory |
| Kimura M, et al. [ | 68 F | 2 weeks | Dysarthria, gait disturbance | Takotsubo cardiomyopathy | GQ1b, GT1a, GM1/GT1a | IVIg, IVMP, PE | Ambulatory |
| Mori D, et al. [ | 51 M | 4 days | Disturbance of consciousness | – | GQ1b | IVIg, IVMP | Ambulatory |
| Mori D, et al. [ | 28 F | Unknown | Disturbance of consciousness | Septic shock | Negative | IVIg, IVMP, PE | Death |
| Naoki I, et al. [ | 28 F | 5 days | Paresthesia, limb weakness, unsteadiness | – | GQ1b | IVIg, IVMP, PE | Ambulatory |
| Present case | 36 F | 10 days | Paresthesia in both hands | Paralytic ileus | GQ1b, GT1a | IVIg, IVMP | Ambulatory |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPeripheral Neuropathies and Disorders · Long-Term Effects of COVID-19 · Peripheral Nerve Disorders
Introduction
Bickerstaff brainstem encephalitis (BBE) is a rare variant of Guillain-Barré syndrome (GBS), characterized by the triad of altered consciousness, ataxia, and external ophthalmoplegia [1,2]. Another atypical subtype is the pharyngeal-cervical-brachial (PCB) variant, which presents with predominant weakness in the pharyngeal, neck, and upper limb muscles [3]. Both subtypes are often preceded by upper respiratory tract infections. Clinical and immunological studies have suggested overlapping features between BBE and PCB, and antiganglioside antibodies such as anti-GQ1b are frequently detected, indicating a shared autoimmune basis [1-3]. COVID-19, caused by SARS-CoV-2, is associated with various neurological complications, and its relationship with GBS is well recognized. It has been pointed out that antiganglioside antibodies are less often detected [4]. Reports of BBE following COVID-19 are limited [5-8], and to date, no cases of co-occurrence of these two variants have been documented, and their pathophysiology is unclear. This study reports a rare case of overlap of BBE and PCB variants following COVID-19 infection. Notably, prompt immunotherapy led to favorable outcomes, despite the development of paralytic ileus during the clinical course.
Case presentation
A 36-year-old woman with a history of depression and ulcerative colitis, for which she had been treated with mesalazine suppository, developed upper respiratory symptoms around 10 days before admission. She was diagnosed with COVID-19 based on a positive SARS-CoV-2 antigen test seven days before admission. Three days before admission, she experienced numbness and unsteadiness in her hands, followed by slurred speech and gait disturbance the following day. Because of dysphagia and altered consciousness, she was admitted to a local hospital the day before and was transferred to our hospital the following day for further evaluation and treatment.
On admission, her vital signs were as follows: heart rate, 72 bpm; blood pressure, 104/74 mmHg; temperature, 36.5°C; SpO₂, 98% (on room air). Cardiac and respiratory sounds were normal, and no rashes were observed. Neurological examination revealed decreased consciousness (Glasgow Coma Scale score of E3V4M6). The patient was responsive to verbal stimuli but exhibited a marked nasal voice. Bilateral ptosis was observed, with pupils measuring 6 mm, sluggish light reflexes, restricted ocular movements, and a fixed central gaze. Facial muscle strength was preserved, but she tended to show involuntary crying-like expressions. Manual muscle testing revealed weakness in the neck and upper limbs (grade 4) and mild weakness in the lower limbs (grade 4-5). Sensory examination revealed dysesthesia in the bilateral upper limbs, upper trunk, and distal lower limbs and impaired vibratory sensation. Severe limb and truncal ataxia prevented sitting without support. Deep tendon reflexes were reduced or absent in all extremities, and bilateral Babinski and Chaddock signs were positive. Laboratory findings were as follows: WBC count, 7,500/μL; RBC count, 539 × 10^4^/μL; Hb, 15.9 g/dL; C-reactive protein, 0.55 mg/dL; ammonia, 23 μg/dL; procalcitonin, 0.0 ng/mL. Vitamin B1 was within normal range. Autoantibodies against collagen vascular diseases were absent. CSF analysis showed a clear appearance, an opening pressure of 10 cm H₂O, a normal cell count of 2/μL, and a protein level of 44 mg/dL (Table 1). Nerve conduction studies revealed no significant abnormalities. Electroencephalography (EEG) showed a posterior dominant alpha rhythm of 8-9 Hz, which was mildly slower than expected for her age and was poorly organized (Figure 1A). Median nerve somatosensory evoked potential (SEP) revealed the reduction of N20 amplitude, although the P13/14 onset latency was within normal limits (Figure 1C). Brain MRI revealed no intracranial hyperintense lesions or contrast enhancement (Figure 2). Based on these findings, BBE was the primary diagnostic consideration as a disorder presenting with polyneuropathy and brainstem dysfunction, and the patient was admitted for treatment.
Neurophysiological examinationEEG on days 2 (A) and 16 (B); SEP of the median nerve on days 2 (C) and 23 (D)(A) EEG on admission showed background activity of 8-9 Hz with a poorly organized posterior dominant rhythm, considered slow for age. (B) EEG normalized following improvement in arousal after treatment. (C) The initial SEP showed a reduction in N20 amplitude (red line). (D) Follow-up SEP after treatment demonstrated recovery of the N20 amplitude.EEG filter settings: high-cut filter, 60 Hz; time constant, 0.3 s; AC filter, onCPc, Centroparietal electrode contralateral to the stimulation; EEG, Electroencephalography; EPi, Erb’s point electrode ipsilateral to the stimulation; Fz, Midline frontal electrode; NC, Non-cephalic reference; SEP, Somatosensory evoked potential
Brain MRI on admission(A) Axial DWI of the midbrain level. (B) Axial FLAIR image. (C) Axial T1-weighted image with gadolinium contrast. No intracranial hyperintense lesions or abnormal contrast enhancement were observed, including within the limbic system.DWI, Diffusion-weighted imaging; FLAIR, Fluid-attenuated inversion recovery; MRI, Magnetic resonance imaging
Because of the impaired consciousness and bulbar palsy, the patient was admitted to the ICU for close monitoring. IVIg therapy (400 mg/kg/day) was administered for five days starting on the day of admission, followed by three days of methylprednisolone pulse therapy (1,000 mg/day). Her level of consciousness rapidly improved. By hospital day 8, the patient was fully alert and did not require mechanical ventilation. Subsequently, she was transferred to the general ward on day 10. Neurological symptoms improved significantly within the first week; however, ataxia became more apparent as the muscle strength recovered. Numbness in the upper limbs persisted for approximately two weeks. On hospital day 3, the patient developed abdominal distention, pain, and nausea. Abdominal radiography and CT revealed diffuse intestinal dilation without signs of obstruction, leading to the diagnosis of paralytic ileus. Fasting and central venous nutrition were initiated, and the symptoms resolved within approximately 10 days (Figure 3). A follow-up EEG demonstrated normalized background activity (Figure 1B), and SEP showed recovery of the N20 potential amplitude (Figure 1D). Serological testing was positive for serum IgG anti-GQ1b and anti-GT1a antibodies, confirming the diagnosis of BBE with features of the PCB variant. The patient regained the ability to stand by day 10 and walked unassisted by day 20. Ultimately, the patient was transferred for rehabilitation on day 24, with mild bilateral abduction limitation and lower limb-dominant ataxia at discharge (Figure 4).
Abdominal X-rays showing paralytic ileusRadiography performed on day 4 (A) shows diffuse intestinal dilation without evidence of mechanical obstruction, which improved with conservative treatment by day 14 (B).
Post-admission clinical course ICU, Intensive care unit; IVIg, Intravenous immunoglobulin; mPSL, Methylprednisolone
Discussion
BBE and its PCB variant are rare subtypes of GBS. Disease-specific antibodies are presumed to be anti-GQ1b antibodies against BBE and anti-GT1a antibodies against PCB variant [1-3]. Clinically, approximately 60% of BBE cases present with pharyngeal palsy, suggesting that these two conditions may lie on the clinical spectrum. This is further supported by serological findings, which show that 90% of anti-GT1a antibody-positive cases are also positive for anti-GQ1b antibodies due to cross-reactivity [3,5].
In the present case, the patient developed BBE approximately 10 days after COVID-19 infection, initially presenting with the classical triad of BBE and bilateral upper limb paresthesia. She exhibited marked nasal speech, sensory disturbances predominantly in the upper limbs and trunk, and muscle weakness. Based on these clinical features, a coexisting PCB variant was suspected, supported by the presence of serum IgG anti-GQ1b and anti-GT1a antibodies. Abnormal median nerve SEP findings, such as reduced N20 amplitude or disappearance of the N20 component with preserved P13/14 onset latency, are frequently observed in BBE and are considered useful for early diagnosis [9]. In the present case, such findings were detected by SEP two days after admission, despite the absence of any brain MRI abnormalities.
COVID-19 has been recognized as a potential trigger for GBS. A systematic review of 436 patients reported a mean age of 61 years with a male predominance, with GBS symptoms typically emerging at an average of 19 days following the onset of COVID-19. The most common clinical subtype is acute inflammatory demyelinating polyneuropathy. Among the reviewed cases, four were classified as PCB variants, whereas none were identified as BBE. A notable feature of COVID-19-associated GBS is the low detection rate of antiganglioside antibodies. Among 16 reported cases of Miller-Fisher syndrome (MFS), anti-GQ1b antibodies were detected in only two cases, a significantly lower rate than the general detection frequency of approximately 90%. This suggests that the pathogenesis of MFS differs between patients with and without COVID-19 infection [4]. Given the shared pathophysiological features between BBE and MFS [10], BBE cases occurring in the context of COVID-19 may also exhibit a lower frequency of anti-GQ1b antibody positivity.
We compared the present case with five previously reported cases of BBE following COVID-19 infection [5-8] (Table 2). The average interval between infection and onset was 12.2 days (range: 4-28 days), and most patients were positive for the anti-GQ1b antibody. All patients received IVIg therapy and steroid pulse therapy. In our case, the patient developed paralytic ileus during hospitalization. One previously reported case was complicated by takotsubo cardiomyopathy, indicating that careful monitoring for autonomic dysfunction is necessary. Although neurological assessment in the acute phase may be limited by intubation, none of the previously reported cases were considered to involve a coexisting PCB variant. Most patients recovered to a level of independent ambulation. However, one fatal case involved negative serum autoantibody results and MRI findings showing bilateral midbrain abnormalities.
In general, patients who are negative for anti-GQ1b antibodies tend to exhibit abnormal brain MRI findings, increased CSF cell counts and protein levels, and prolonged disturbances of consciousness [11]. In the present case, although BBE developed following COVID-19 infection, brain MRI and CSF findings were both normal. Consciousness and cranial nerve symptoms improved significantly within approximately 1 week. The subsequent detection of anti-GQ1b antibodies was consistent with the typical features of antibody-positive cases. These findings suggest that even when BBE is triggered by COVID-19, testing for anti-ganglioside antibodies remains important for diagnosis.
Conclusions
This study presents a case of overlap of BBE and PCB variants following COVID-19, with a favorable outcome obtained through prompt immunotherapy. In patients presenting with an acute onset of impaired consciousness and brainstem symptoms after COVID-19, BBE should be considered in the differential diagnosis. When symptoms extend beyond the classical triad, the possibility of a coexisting variant, such as the PCB variant, warrants consideration. Assessment of anti-ganglioside antibodies remains essential for diagnosis, even in cases triggered by COVID-19.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bickerstaff brainstem encephalitis and Fisher syndrome: anti-GQ 1b antibody syndrome J Neurol Neurosurg Psychiatry Shahrizaila N Yuki N 5765838420132298420310.1136/jnnp-2012-302824 · doi ↗ · pubmed ↗
- 2Nationwide survey of patients in Japan with Bickerstaff brainstem encephalitis: epidemiological and clinical characteristics J Neurol Neurosurg Psychiatry Koga M Kusunoki S Kaida K Uehara R Nakamura Y Kohriyama T Kanda T 121012158320122285160810.1136/jnnp-2012-303060 · doi ↗ · pubmed ↗
- 3Continuous spectrum of pharyngeal-cervical-brachial variant of Guillain-Barré syndrome Arch Neurol Nagashima T Koga M Odaka M Hirata K Yuki N 151915236420071792363610.1001/archneur.64.10.1519 · doi ↗ · pubmed ↗
- 4Guillain-Barré syndrome associated with COVID-19: a systematic review Brain Behav Immun Health Pimentel V Luchsinger VW Carvalho GL 1005782820233668662410.1016/j.bbih.2022.100578 PMC 9842533 · doi ↗ · pubmed ↗
- 5Bickerstaff encephalitis after COVID-19J Neurol Llorente Ayuso L Torres Rubio P Beijinho do Rosário RF Giganto Arroyo ML Sierra-Hidalgo F 2035203726820213288072310.1007/s 00415-020-10201-1PMC 7471525 · doi ↗ · pubmed ↗
- 6Case report: takotsubo cardiomyopathy in Bickerstaff brainstem encephalitis triggered by COVID-19Front Neurol Kimura M Hashiguchi S Tanaka K 8222471220213500294710.3389/fneur.2021.822247 PMC 8741194 · doi ↗ · pubmed ↗
- 7Bickerstaff brainstem encephalitis developed quickly after COVID-19 infection Acute Med Surg Mori D Yamada T Fukuma H Nakao S Matsuoka T 012202510.1002/ams 2.70071 PMC 1221446940606543 · doi ↗ · pubmed ↗
- 8Successful treatment with plasmapheresis of severe Bickerstaff brainstem encephalitis with high cerebrospinal fluid CXCL-10 levels after COVID-19 infection: a case report Clin Exp Neuroimmunol Naoki I Kenzo S Riyoko K Kenji I Yoshihisa Y 3034162025