Grade V AAST Intestinal Vascular Injury Secondary to Blunt Abdominal Trauma: A Case Report From a University Hospital in Saltillo, Mexico
Alejandra Y Proa-Arriaga, Adrian A Santos-Vega, Oscar A Romero, Gloria Isela Mendoza-Frías, Fernando Martínez-Cuspinera

TL;DR
A 65-year-old man with blunt abdominal trauma from a bicycle accident was found to have a severe intestinal injury requiring surgery, highlighting the importance of thorough evaluation in such cases.
Contribution
This case report presents a rare Grade V AAST intestinal vascular injury caused by blunt trauma and emphasizes the need for careful clinical re-evaluation.
Findings
The patient had a Grade V AAST intestinal injury with a devascularized ileal segment and mesenteric hematoma.
The injury was initially suspected via the 'string of pearls' sign on imaging and confirmed during surgery.
The patient recovered well post-surgery and was discharged with no complications.
Abstract
A 65-year-old male with no relevant medical history presented to the emergency department with generalized abdominal pain following blunt trauma caused by a bicycle handlebar impact to the mesogastrium 48 hours prior. The patient initially self-medicated with analgesics without improvement. Upon evaluation, he had stable vital signs, epigastric ecchymosis, decreased peristalsis, and signs of generalized peritonism. Laboratory results showed leukocytosis (17.6 x 109/L). Plain abdominal radiographs showed intestinal loops with diameters within normal limits and a few short air-fluid levels in the left hypochondrium. Notably, the distribution of intraluminal gas in that region revealed a “string of pearls” sign, raising suspicion for an obstructive process. An abdominal CT scan revealed inflammatory pelvic changes, mesenteric fat stranding, dilated ileal loops, and free fluid in the pelvic…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
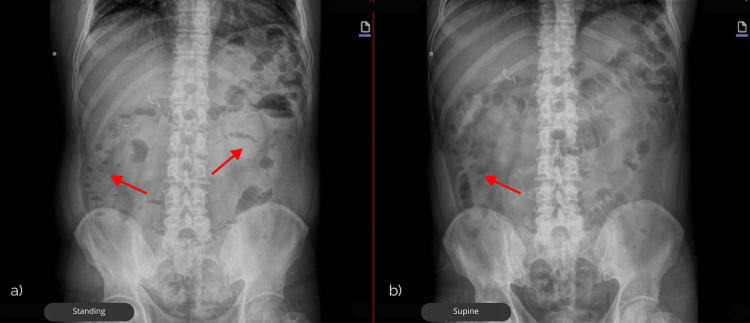 Figure 1
Figure 1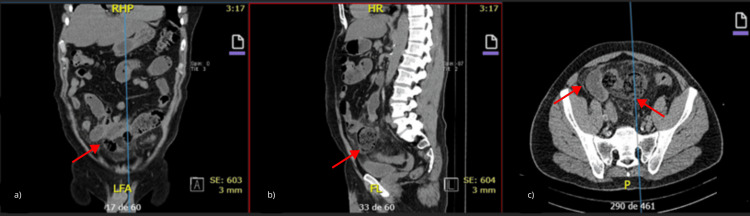 Figure 2
Figure 2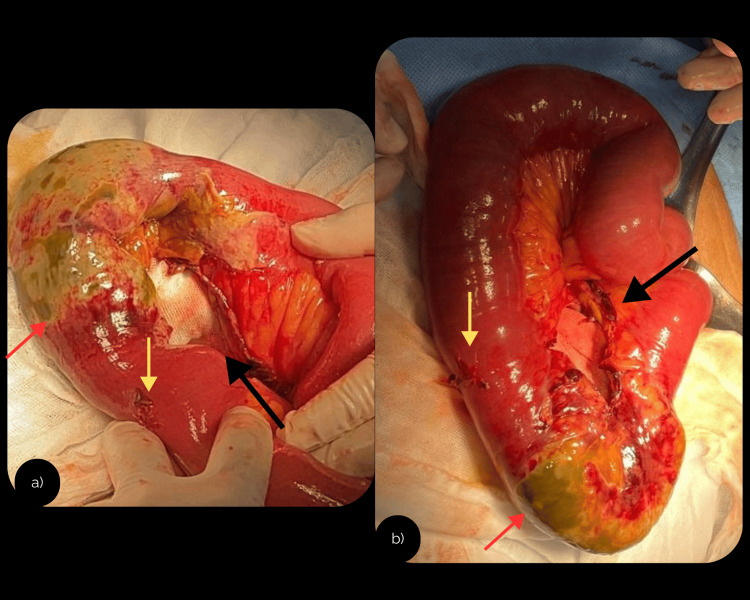 Figure 3
Figure 3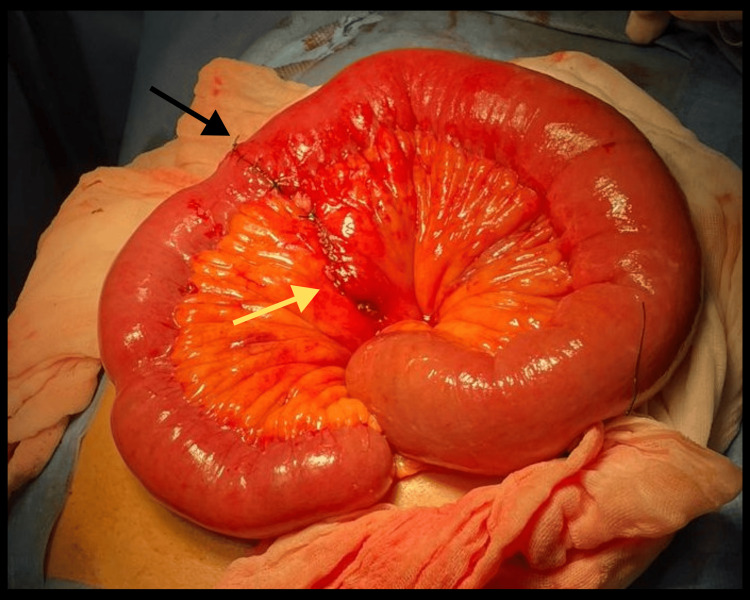 Figure 4
Figure 4| Parameter | Patient Value | Reference Range |
| Hemoglobin (g/dL) | 15 | 12–16 g/dL |
| Platelets (x103/µL) | 242 | 150–400 x 103/µL |
| Leukocytes (x103/µL) | 17.6 | 4.5–11 x 103/µL |
| Neutrophils (%) | 87.2 | 40–70% |
| Glucose (mg/dL) | 130 | 70–110 mg/dL |
| Blood Urea Nitrogen (BUN) (mg/dL) | 16.5 | 7–20 mg/dL |
| Creatinine (mg/dL) | 1.1 | 0.6–1.2 mg/dL |
| Total Protein (g/dL) | 7 | 6–8.3 g/dL |
| Albumin (g/dL) | 4 | 3.5–5.0 g/dL |
| Amylase (U/L) | 46 | 30–110 U/L |
| Lipase (U/L) | 11 | 0–60 U/L |
| Sodium (mmol/L) | 136 | 135–145 mmol/L |
| Chloride (mmol/L) | 99 | 98–106 mmol/L |
| Potassium (mmol/L) | 4.7 | 3.5–5.1 mmol/L |
| Prothrombin Time (s) | 11.2 | 11–13.5 s |
| International Normalized Ratio (INR) | 1 | 0.8–1.2 |
| Partial Thromboplastin Time (s) | 25.3 | 25–35 s |
| Grade | Type of injury | Description of injury |
| I | Hematoma | Contusion or hematoma without devascularization |
| I | Laceration | Partial thickness, no perforation |
| II | Laceration | Laceration <50% of circumference |
| III | Laceration | Laceration ≥50% of circumference without transection |
| IV | Laceration | Transection of the small bowel |
| V | Laceration | Transection of the small bowel with segmental tissue loss |
| V | Vascular | Devascularized segment |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAbdominal Trauma and Injuries · Trauma Management and Diagnosis · Case Reports on Hematomas
Introduction
American Association for the Surgery of Trauma (AAST) Grade V intestinal injuries represent the most severe form of bowel trauma, involving complete transection or devascularization. Although they account for less than 1% of abdominal trauma cases, they carry a high risk of ischemia, sepsis, and mortality exceeding 40%, underscoring the need for early recognition and prompt surgical management. Abdominal blunt trauma (ABT) in adults can result in injuries ranging from solid organ lacerations to more elusive lesions involving the mesentery and small bowel [1,2]. The abdomen ranks as the third most commonly injured anatomical region [3]. The presence of hemodynamic instability or peritonitis in blunt abdominal trauma constitutes an absolute indication for immediate exploratory laparotomy. This approach aims to prevent progression to sepsis and other severe complications, including dehiscence, fistula, or hemorrhage, with a mortality rate reported in the literature of up to 30% [4-6]. While rare, mesenteric vascular injuries carry significant morbidity due to their often-subtle clinical presentation and potential for delayed diagnosis [1,2]. This case report describes a high-grade intestinal vascular injury (AAST Grade V) secondary to blunt abdominal trauma, as well as the surgical approach required for its management.
Case presentation
A 65-year-old male with no significant past medical history presented to the emergency department 48 hours after falling from a bicycle and striking his mesogastrium against the handlebar. The patient reported progressive abdominal pain, unrelieved by self-administered analgesics, and associated fever. On arrival, he was hemodynamically stable. Physical examination revealed epigastric ecchymosis, decreased peristalsis, generalized abdominal dullness, and positive McBurney and Rovsing signs.
Laboratory tests revealed leukocytosis, neutrophilia and hyperglycemia (Table 1).
Plain abdominal radiographs in two positions showed intestinal loops with diameters within normal limits and a few short air-fluid levels in the left hypochondrium. Notably, the distribution of intraluminal gas in that region revealed a “string of pearls” sign, raising suspicion for an obstructive process (Figure 1).
Plain abdominal X-rays in two projections showing short air–fluid levels and the “string of pearls” sign, as indicated by the red arrows in (a) standing and (b) supine positions, suggestive of intestinal obstruction.
Abdominal non-contrast computed tomography (CT) imaging showed pelvic inflammation, increased mesenteric fat density, dilated ileal loops with fecaloid content, proximal jejunal dilation with intraluminal fluid, and free fluid in the pelvic cavity (Figure 2).
Abdominal CT demonstrating transition point and proximal dilatationAbdominal computed tomography (CT) in (a) coronal, (b) sagittal, and (c) axial sections demonstrating a pelvic inflammatory process with mesenteric fat stranding, a dilated ileal loop with fecaloid content at the transition point, dilated proximal jejunal loops with fluid, and free fluid in the pelvis (red arrows).
After a non-contrast CT showed a transition point with proximal dilatation, mesenteric fat stranding, and free fluid, the patient’s persistent acute surgical abdomen prompted an exploratory laparotomy.
Intraoperative findings included approximately 150 mL of serosanguineous fluid, a 1 cm hematoma on the mesenteric border of the ileum 100 cm proximal to the ileocecal valve, and an inflammatory phlegmon with dense adhesions between ileal loops, the abdominal wall, and the omentum. A 12.5 cm segment of devascularized ileum with necrosis (bucket-handle sign) was identified 120 cm from the ileocecal valve (Figure 3) consistent with AAST Grade V injury, and involving ischemic changes to the distal third of the cecal appendix (edematous, erythematous, and covered with fibrinous coating).
Exploratory laparotomy: intraoperative images.Intraoperative photographs taken during exploratory laparotomy showing different angles of the same lesion. (a, b) Bucket-handle injury of the ileum (black arrow), associated with loss of viability of an ileal segment (red arrow) and serosal disruption of the ileum (yellow arrow).
Resection of the devascularized segment (approximately 15 cm) was performed, followed by a single-layer anastomosis using Connell-Mayo sutures with 2-0 Vicryl, and a second seromuscular layer with Lembert sutures using 2-0 silk (Figure 4).
Intraoperative outcome of the procedure: anastomosis with closure of the mesenteric defect.A first-layer anastomosis (black arrow) was performed using Connell-Mayo sutures with 2-0 Vicryl, reinforced with a second seromuscular layer using Lembert sutures with 2-0 silk. The mesenteric defect (yellow arrow) was closed with a continuous 2-0 silk suture.
The patient had an uncomplicated postoperative course, tolerated oral feeding by postoperative day 2, and was discharged with scheduled outpatient follow-up. Final histopathological analysis confirmed necrotic ileum with regional peritonitis and periappendicitis.
Discussion
Intestinal vascular lesions following blunt trauma pose diagnostic challenges due to their often-subtle onset [3]. This case illustrates the importance of maintaining a high index of suspicion in patients with blunt abdominal trauma and highlights the role of early imaging and surgical intervention in preventing complications.
Blunt abdominal trauma with intestinal or mesenteric injury is uncommon but potentially life-threatening. Duodenal injury is often diagnosed late due to the retroperitoneal location of the duodenum and is associated with high rates of complications and mortality [2]. The main mechanism of injury is crushing (blunt trauma), caused, for example, by the handlebar of a bicycle or the steering wheel of a car [7]. A less common cause is deceleration, which more frequently results in damage to the third and fourth portions of the duodenum [7].
In hemodynamically stable patients with suspected intra-abdominal injury, CT serves as an adjunct to clinical assessment [8]. In this case, a non-contrast CT showed indirect signs (transition point, mesenteric fat stranding, and free pelvic fluid) that supported - rather than determined - the decision for exploratory laparotomy prompted by persistent peritoneal signs.
A 2019 meta-analysis evaluated over 1,000 patients with blunt abdominal trauma and found conservative management successful in 60%, with 40% requiring surgical intervention [3], and highlighted the importance of early diagnosis and multidisciplinary collaboration in optimizing outcomes.
The classification of small bowel injuries proposed by Moore et al. provides a standardized grading system to assess trauma severity, ranging from Grade I (hematoma without devascularization) to Grade V (bowel transection with segmental tissue loss or complete devascularization) [9]. In this system, an additional category includes isolated vascular injuries, which are also classified as Grade V. This grading scale is particularly useful for correlating radiological findings with intraoperative damage and for guiding surgical decision-making [9]. In cases involving multiple intestinal injuries, the authors recommend increasing the grade by one level, up to a maximum of Grade III, as shown in Table 2.
This case underscores a low threshold for exploration when indirect CT signs persist alongside peritoneal findings, even with non-contrast CT. Once segmental devascularization is confirmed, limited resection with primary anastomosis is appropriate and was associated with an uncomplicated recovery in our patient [1,4,6]. An appendectomy was performed due to an inflamed-appearing appendix; final histopathology showed periappendicitis (serosal inflammation), consistent with a reactive/incidental finding.
This case contributes to the limited literature on high-grade AAST intestinal vascular injuries and emphasizes the need for vigilance in evaluating patients with delayed presentation after blunt trauma.
Conclusions
High-grade mesenteric and small bowel vascular injuries, although rare, must be considered in blunt abdominal trauma with persistent or worsening symptoms. They can present late and with subtle imaging findings. In our patient, non-contrast CT demonstrated indirect signs (transition point, mesenteric fat stranding, free pelvic fluid) that supported - but did not replace - clinical judgment in the context of a surgical abdomen; early laparotomy with limited resection led to an uncomplicated recovery. CT should be used as an adjunct to identify additional or missed injuries and to aid surgical planning, while maintaining a low threshold for operative exploration when peritoneal signs persist despite equivocal imaging.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The impact of prior laparotomy and intra-abdominal adhesions on bowel and mesenteric injury following blunt abdominal trauma World J Surg Loftus TJ Morrow ML Lottenberg L 4574654320193022556310.1007/s 00268-018-4792-6PMC 6330127 · doi ↗ · pubmed ↗
- 2Duodenal rupture after blunt abdominal trauma by bicycle handlebar: case report and literature review Niger J Surg Mendoza-Moreno F Furtado-Lobo I Pérez-González M 2132162520193157938010.4103/njs.NJS_31_18PMC 6771178 · doi ↗ · pubmed ↗
- 3No need for surgery? Patterns and outcomes of blunt abdominal trauma Innov Surg Sci Goedecke M Kühn F Stratos I Vasan R Pertschy A Klar E 100107420193170930110.1515/iss-2018-0004 PMC 6817729 · doi ↗ · pubmed ↗
- 4Selective nonoperative management of blunt splenic injury: an Eastern Association for the Surgery of Trauma practice management guideline J Trauma Acute Care Surg Stassen NA Bhullar I Cheng JD 073201210.1097/TA.0b 013e 3182702 afc 23114484 · doi ↗ · pubmed ↗
- 5Nonoperative management of blunt hepatic injury: an Eastern Association for the Surgery of Trauma practice management guideline J Trauma Acute Care Surg Stassen NA Bhullar I Cheng JD 073201210.1097/TA.0b 013e 318270160 d 23114483 · doi ↗ · pubmed ↗
- 6Management of the complex duodenal injury Am J Surg Bolaji T Ratnasekera A Ferrada P 63964422520233658801610.1016/j.amjsurg.2022.12.016 · doi ↗ · pubmed ↗
- 7Duodenal injury in blunt abdominal trauma. Case report and literature review Cir Cir Rodríguez-García JA Ponce-Escobedo AN Pérez-Salazar DA Sepúlveda-Benavides CA Uvalle-Villagómez RA Muñoz-Maldonado GE 535787201910.24875/CIRU.1900077931501625 · doi ↗ · pubmed ↗
- 8Concordance between tomographic and surgical AAST injury grades in liver, spleen, and kidney due to blunt abdominal trauma Cir Cir Bolívar-Rodríguez MA Niebla-Moreno JM Respardo-Ramírez CA Pámanes-Lozano A Cázarez-Aguilar MA de Jesús Peraza-Garay F 3853919020223525975510.24875/CIRU.21000415 · doi ↗ · pubmed ↗