Letter to the Editor regarding “Brachial plexus compression following a laterjet procedure”
Olivier Camuzard, Tanguy Perraudin, Lucas Lo Cunsolo, Elise Lupon

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
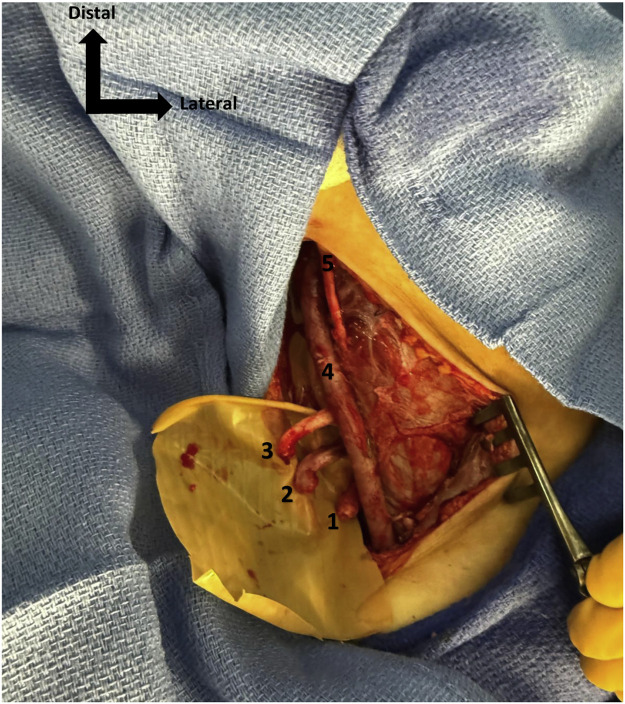 Figure 1
Figure 1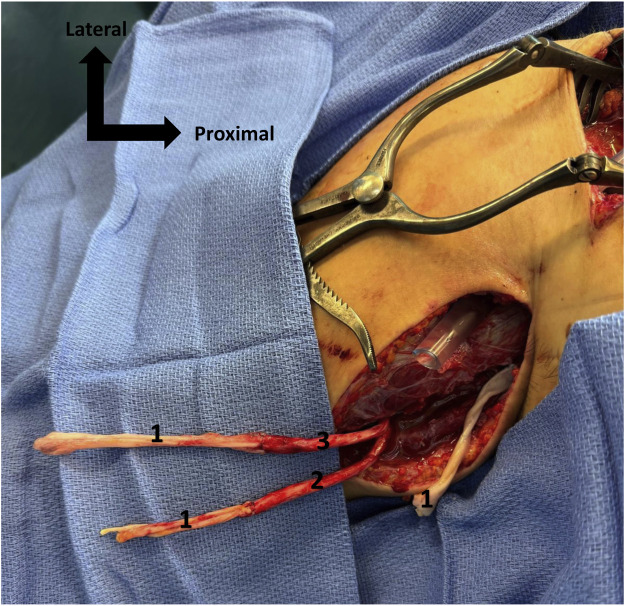 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsShoulder Injury and Treatment · Shoulder and Clavicle Injuries · Spine and Intervertebral Disc Pathology
Dear Sir,
With great interest, we read the manuscript written by Dounas et al.1 The authors reported an interesting case of brachial plexus compression caused by a residual pectoralis minor band that remained attached to the coracoid and was transposed to the anterior glenoid during a Latarjet procedure, leading to compression of the underlying cords. We would like to contribute additional insight by sharing our own experience with brachial plexus injury in the context of this procedure.
The Latarjet procedure is a well-established solution for the treatment of anterior shoulder instability. The authors present a case of a patient with an uncommon, subtle presentation of brachial plexus injury that fully resolved after neurolysis, which is valuable for clinicians to recognize.1 It is important to note, however, that different approaches to the Latarjet procedure exist, including both open and arthroscopic techniques.2 The authors did not explicitly specify whether the procedure in their case was performed using an open or arthroscopic Latarjet approach, although this distinction is important as it can significantly influence the type and severity of potential complications.3
The authors reviewed the literature on the mechanisms of brachial plexus injury associated with the Latarjet procedure and briefly mentioned iatrogenic lacerations without providing further details, an aspect that we would like to emphasize.1 Indeed, the arthroscopic procedure, as first described in our academic hospital,4 and now widely used worldwide, may lead to operative lacerations—an important risk that reconstructive surgeons should be aware of. This technique includes a delicate step of shaving the anterior glenoid rim, which carries a potential for severe neurovascular injury. We recently encountered such a complication in a 21-year-old right-handed student, a non-smoker and otherwise healthy, who presented with right anterior shoulder instability in the context of high-level sports activity. She underwent an arthroscopic Latarjet procedure that was complicated by an axillary vessel injury caused by the shaver, requiring emergency repair with a saphenous vein graft. She was referred to our reconstructive department 5 days later with a right infraclavicular brachial plexus injury, presenting with complete motor and sensory deficit of the right upper limb. We approached the brachial plexus through the deltopectoral groove and identified a complete transection of the lateral, medial, and posterior cords (Figure 1). The nerve gap was measured at 10 cm for the posterior cord and 8 cm for both the lateral and medial cords, using a second approach at the level of the brachial canal, which had already been explored during the arterial repair. Three end-to-end nerve grafts were performed using autologous sural nerve cable grafts matching the size of each defect, secured with 8–0 Prolene sutures to restore continuity of the three transected cords (Figure 2). The anastomoses were protected with fibrin sealant (TISSEEL®, Baxter Healthcare Corporation, Deerfield, IL, USA) and the limb was immobilized for 21 days.Figure 1. Distal stumps of the 3 cords of brachial plexus, externalized in the brachial canal. 1. Posterior cord, 2. Medial cord, 3. Lateral cord, 4. Venous bypass, 5. Musculocutaneous nerve.Figure 1. Figure 2Sural nerve graft between distal stump of brachial plexus cords (already sutured) and proximal stumps of the 3 cords., 1. Sural nerve graft, 2. Medial cord, 3. Lateral cord.Figure 2
Postoperative recovery was marked by severe pain requiring step 3 analgesics and regional anesthetic blocks for pain control. This case highlights an acute and devastating complication that may occur following arthroscopic Latarjet procedures, potentially jeopardizing limb viability. Given the extent of the nerve injuries, the prognosis for functional recovery remains guarded.5
We thank the authors for raising awareness of nerve injuries associated with this procedure and wish to emphasize another dramatic mechanism related to the shaving step of the surgery, along with a proposed surgical management strategy.
Funding
This study has received no funding.
Release of information
The study subject has consented to clinical photographs and imaging for academic research.
Declaration of competing interest
The authors have no conflicts of interests to declare.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Dounas G.D.Ibrahim A.Pour-Ahmadi A.White J.Potter A.Brachial plexus compression following a laterjet procedure JPRAS Open 4520253583624076142710.1016/j.jpra.2025.07.005PMC 12319328 · doi ↗ · pubmed ↗
- 2VuletićF.Bøe B.Current trends and outcomes for open vs. Arthroscopic latarjet Curr Rev Musculoskelet Med 17520241361433846798710.1007/s 12178-024-09889-9PMC 11068718 · doi ↗ · pubmed ↗
- 3Horner N.S.Moroz P.A.Bhullar R.Open versus arthroscopic Latarjet procedures for the treatment of shoulder instability: a systematic review of comparative studies BMC Musculoskelet Disord 19120182553004574510.1186/s 12891-018-2188-2PMC 6060556 · doi ↗ · pubmed ↗
- 4Boileau P.Mercier N.Roussanne Y.Thélu C.Old J.Arthroscopic Bankart-Bristow-Latarjet procedure: the development and early results of a safe and reproducible technique Arthroscopy 26112010143414502103500710.1016/j.arthro.2010.07.011 · doi ↗ · pubmed ↗
- 5Suroto H.Rifqi Farizan Akbar M.Aprilya D.Pribadi F.Validity and reliability of prognosis brachial plexus injury score for traumatic brachial plexus injury Clin Orthop Surg 15120231531583677899110.4055/cios 22168 PMC 9880511 · doi ↗ · pubmed ↗