OKAIN: A comprehensive oncology knowledge base for the interpretation of clinically actionable alterations
Zhenhua Yang, Chunwei Xu, Mingmin Wang, Xinxiu Meng, Kai Wang, Aodi Wang

TL;DR
OKAIN is a precision oncology tool that helps identify clinically actionable genetic mutations in cancer patients.
Contribution
OKAIN introduces a weighted evidence analysis system for assessing actionable cancer mutations with over 100,000 variants.
Findings
OKAIN contains over 100,000 variants in 1,239 cancer-associated genes.
It includes 12,409 therapeutic evidence entries, with 2,600 classified as Level A.
The database integrates 864 entries from Chinese guidelines or NMPA labels.
Abstract
The increased use of next-generation sequencing in clinical genetic testing has resulted in the identification of several genetic variations with possible therapeutic implications. We developed OKAIN (https://szcube.origimed.com), an algorithm tool that assesses clinically actionable mutations using a precision oncology knowledge database. OKAIN employs a weighted evidence analysis system to deliver final clinical annotation outcomes for intricate variations. As of now, OKAIN has amassed over 100,000 variants in 1,239 cancer-associated genes, encompassing 12,409 entries of therapeutic evidence in 471 genes. This collection highlights 2,600 Level A evidence entries in 66 genes, with 864 entries derived from the National Medical Products Administration labels or Chinese guidelines. OKAIN acts as a precision oncology knowledge base for the assessment of clinically actionable alterations,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
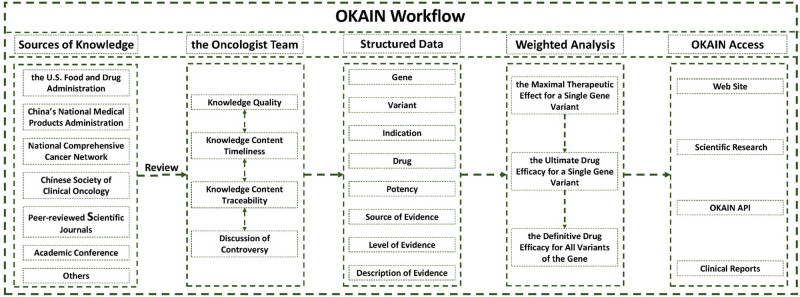 Figure 1
Figure 1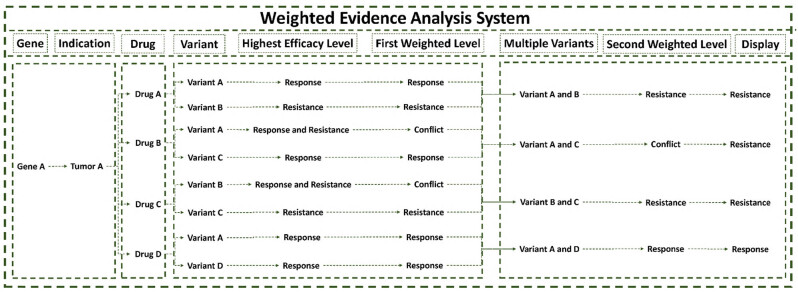 Figure 2
Figure 2 Figure 3
Figure 3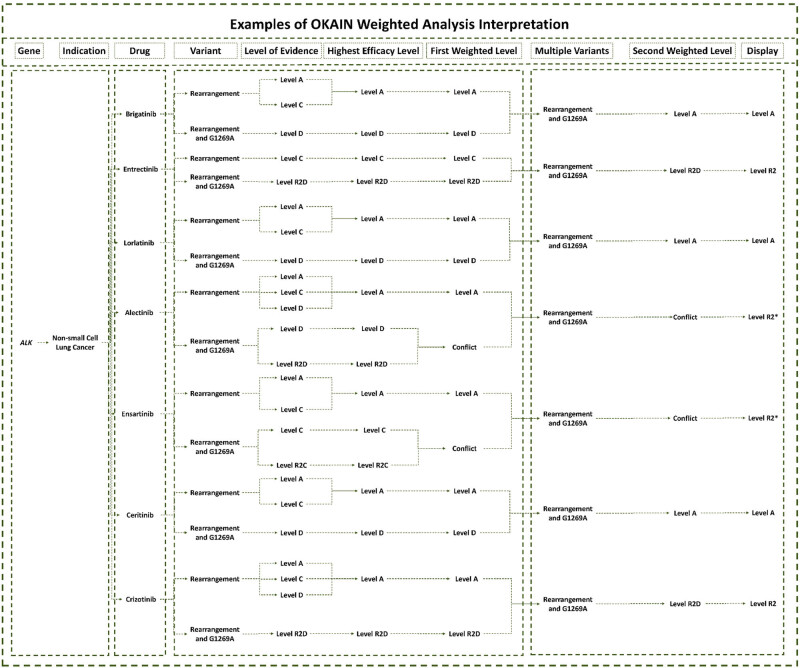 Figure 4
Figure 4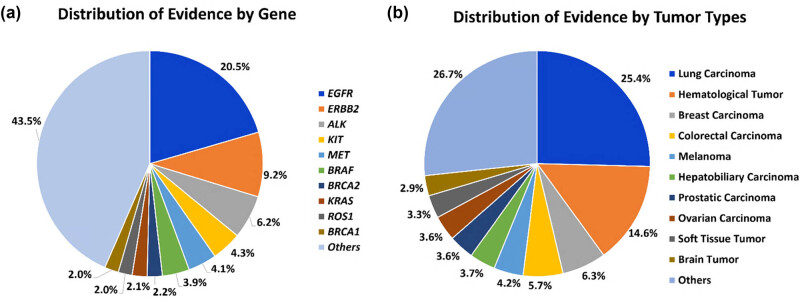 Figure 5
Figure 5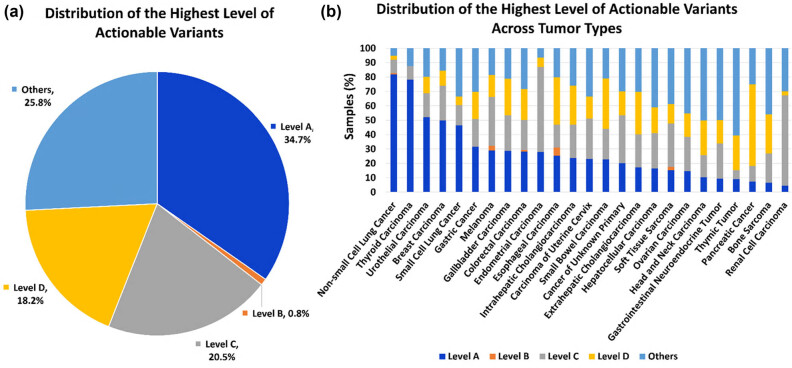 Figure 6
Figure 6| Potency | Category | Therapeutic |
|---|---|---|
| Response | Level A | A biomarker predictive of response to FDA/NMPA-approved therapies or those recommended by clinical guidelines in this indication |
| Level B | A biomarker predictive of response to therapies, demonstrated by extensive retrospective studies or prospective investigations (Phase III clinical studies), in this indication | |
| Level C | C1. A biomarker predictive of response to FDA/NMPA-approved therapies or those recommended by clinical guidelines in another indication | |
| C2. A biomarker predictive of response to therapies, demonstrated by small-scale retrospective studies or early-stage prospective studies (Phase I or II clinical studies) in this indication | ||
| Level D | D1. A biomarker predictive of response to therapies, demonstrated by a limited number of case reports in this indication | |
| D2. A biomarker predictive of response to therapies, supported by preclinical study results | ||
| Resistance | Level R1 | A biomarker predictive of resistance to therapies, authorized by the FDA/NMPA or advised in professional clinical guidelines in this indication |
| Level R2 | R2B. A biomarker predictive of resistance to therapies, demonstrated by extensive retrospective studies or prospective investigations (Phase III clinical studies), in this indication | |
| R2C. A biomarker predictive of resistance to therapies, demonstrated by small-scale retrospective studies or early-stage prospective studies (Phase I or II clinical studies) in this indication | ||
| R2D1. A biomarker predictive of resistance to therapies, demonstrated by a limited number of case reports in this indication | ||
| R2D2. A biomarker predictive of resistance to therapies, supported by preclinical study results |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGenomics and Rare Diseases · Cancer Genomics and Diagnostics · Colorectal Cancer Treatments and Studies
Introduction
1
Precision oncology is a rapidly emerging field that involves the molecular profiling of tumors to discern diagnostic, prognostic, and therapeutic implications [1–3]. Patients are increasingly undergoing multigene sequencing of individual tumors to identify potential tumor biomarkers that could be effectively targeted with corresponding drugs. Both the Food and Drug Administration (FDA) and the National Medical Products Administration (NMPA) have approved numerous drugs based on these biomarkers, such as larotrectinib. For example, larotrectinib can be successfully used as a treatment when an NTRK fusion is identified in a solid tumor patient without a known acquired resistance mutation.
While there is a broad consensus on the interpretation of certain genomic alterations, such as epidermal growth factor receptor (EGFR) T790M and EGFR L858R, a large number of genetic variants that lack consensus for interpretation pose a significant challenge [4–6], including co-mutations and acquired drug-resistance variants. The use of precision medical technology in oncology has led to the widespread adoption of next-generation sequencing (NGS) large panel detection as the primary clinical approach. This method allows for comprehensive coverage of rare mutation targets, systematic identification of co-occurring mutations in tumors, and significant improvements in clinical detection efficiency. However, accurately interpreting rare mutations remains a major clinical challenge. Therefore, it is necessary to create a precision oncology knowledge base that offers centralized, freely accessible, and accurately interpreted clinical information on genomic data. This tool would assist clinicians in interpreting genomic alterations detected in patient tumor samples, enabling them to make optimal treatment decisions.
Existing knowledge bases designed to aid in the clinical interpretation of alterations include resources such as Clinical Interpretation of Variants in Cancer (CIViC) [4] and OncoKB [5]. However, most of these databases provide either the final clinical annotation results or multiple pieces of clinical interpretation evidence for the alterations. Additionally, thorough annotations of gene variations of Chinese drugs are not considered in most of those databases.
To address this issue, we present OKAIN, a knowledge base for precision oncology that assesses clinically actionable alterations. OKAIN includes a wide range of information related to genomic variants associated with cancer and their effectiveness in treatment. Its purpose is to offer physicians precise and structured interpretations of cancer mutations found in patients’ tumors, thereby facilitating clinical decision making.
OKAIN provides comprehensive insights into the therapeutic efficacy of co-mutations, acquired drug-resistant variants, and rare mutations, assisting physicians in precisely treating patients with complex variants. The knowledge base includes a weighted evidence analysis system that conducts a thorough analysis of the evidence related to the therapeutic efficacy of a tumor patient’s cancer-associated genomic variants. This system enables the acquisition of robust evidence of therapeutic efficacy in tumor patients.
Methods
2
OKAIN (Version 1.0, 2024) accommodates clinically relevant cancer variants, including single nucleotide variants, frameshifts, insertions, deletions, gene rearrangements, copy number variations, and changes in expression levels. These variants are described unambiguously using the HGVS nomenclature [7,8]. OKAIN contains information about the biological effects and treatment implications of specific cancer genes and their variations. As shown in Figure 1, the data are sourced from a variety of authoritative entities, encompassing the FDA, NMPA, clinical guidelines, peer-reviewed scientific journals, and major conference proceedings, among others. Biological and clinical implications are meticulously reviewed by oncologist teams. To ensure a clear and precise representation of data, we will structure the information systematically. The structured data will include genes, variants, indication, drug, potency, source of evidence, level of evidence, and description of evidence. The weighted evidence analysis system to deliver final clinical annotation outcomes for intricate variations. The OKAIN dataset is mainly used for clinical research and to enhance OrigiMed’s clinical reporting. Users can access this dataset through an intuitive and interactive web interface at https://szcube.origimed.com.
OKAIN workflow.
In accordance with guidelines from the American Society of Clinical Oncology, the Association for Molecular Pathology, the College of American Pathologists, and the European Society for Medical Oncology [9,10], as well as information from public databases like OncoKB and consensus among oncologists, we have developed levels of evidence classification system (Table 1).
Continual research on the efficacy of genomic variants often produces conflicting evidence regarding the effectiveness of specific gene alterations. This poses a significant obstacle to the rapid interpretation of genomic alterations. To address this issue, OKAIN’s weighted evidence analysis system performs a comprehensive analysis of all therapeutic efficacy evidence for a specific genomic variant related to a particular drug, to determine the highest degree of efficacy for that drug. The highest level of efficacy is then evaluated against all variants of the gene, resulting in efficacy data for all gene variants in relation to the medication (Figure 2).
OKAIN’s weighted evidence analysis system. The Highest Efficacy Level indicates the maximal therapeutic effect for the specific genomic variant in response to a specific drug.
Within this framework, sensitivity evidence levels (A, B, C, D) exhibit direct correspondence with resistance evidence levels (R1, R2B, R2C, R2D), respectively, when weighted for a specific gene–tumor–drug–variant association. Sensitivity evidence levels follow a hierarchical order from highest to lowest (A → B → C → D), while resistance evidence levels descend correspondingly (R1 → R2B → R2C → R2D).
OKAIN prioritizes negative clinical evidence, discouraging the use of targeted therapies when the evidence suggests the therapy may be ineffective or controversial. When weighing the evidence level for multiple variants based on a specific drug, the evidence for drug resistance and conflicting evidence is prioritized over the level of evidence for sensitivity.
The Highest Efficacy Level represents the most clinically significant evidence tier for a specific gene–tumor–drug–variant, encompassing both sensitivity and resistance classifications following weighting analysis. For example, a variant may concurrently exhibit Level A, Level C, Level D, Level R2B, and Level R2D, wherein the Highest Efficacy Level would report Level A (highest sensitivity) and Level R2B (highest resistance).
The First Weighted Level denotes the definitive therapeutic efficacy prediction for a specific genomic variant in a given tumor type, derived directly from the Highest Efficacy Level. When conflicting evidence exists (e.g., concurrent sensitivity and resistance classifications), the system outputs “Conflict.”
The Second Weighted Level denotes the consensus therapeutic efficacy for all variants of a gene within a specified drug–tumor context, derived through aggregation of First Weighted Levels. This tier exclusively retains the highest efficacy level (sensitivity or resistance) observed across variants. When multiple distinct sensitivity types coexist within the definitive First Weighted Levels, prioritization follows the hierarchy: Resistance → Conflict → Response, preserving only the highest-priority classification. Should the Second Weighted Level manifest as “Conflict,” the final display will default to “Resistance” paired with the Highest Resistance Level, thereby prioritizing patient safety through avoidance of contentious therapeutic approaches.
Results
3
Levels of evidence
3.1
OKAIN categorizes the evidence for sensitivity to targeted therapies into four levels (A, B, C, and D) for each genetic alteration, based on the strength of clinical and preclinical data supporting the use of the mutation as a predictive biomarker.
Level A includes specific alterations that have been approved by the FDA/NMPA or recommended by clinical professional guidelines as predictive of response to particular therapies in specific tumors. The FDA has approved avapritinib as a treatment for adult patients with unresectable or metastatic gastrointestinal stromal tumor (GIST) that harbor a platelet-derived growth factor receptor alpha (PDGFRA) exon 18 mutation, including PDGFRA D842V mutations. Avapritinib is a tyrosine kinase inhibitor that targets PDGFRA and PDGFRA D842 mutants, as well as multiple KIT proto-oncogene (KIT) exon 11, 11/17, and 17 mutations with half-maximal inhibitory concentrations (IC_50_s) less than 25 nM. In vitro cellular assays, avapritinib inhibited the autophosphorylation of KIT D816V and PDGFRA D842V mutants, which are associated with resistance to approved kinase inhibitors. The IC_50_ for KIT D816V was 4 nM and for PDGFRA D842V was 30 nM. Therefore, the use of avapritinib to treat GIST patients with PDGFRA D842V mutations is classified as Level A (Figure 3).
Examples of the OKAIN levels of evidence. The level of evidence shows the efficacy for a specific genomic variant related to a particular drug.
Level B includes specific alterations that serve as predictive biomarkers of response to therapies. These alterations have been established through large-scale retrospective studies or prospective studies, at least Phase III, in particular types of tumors. The ZETA Trial, a Phase III study, showed that patients with medullary thyroid cancer (MTC) who had a somatic RET M918T mutation had a higher objective response rate to vandetanib (55%) than patients with sporadic MTC tumors that lacked a somatic M918T mutation (33%) [11]. In vitro studies have shown that vandetanib inhibits the tyrosine kinase activity of various receptor tyrosine kinases, including the EGFR and vascular endothelial growth factor (VEGFR) families, Ret proto-oncogene (RET), protein tyrosine kinase 6 (BRK), TEK receptor tyrosine kinase (TIE2), and members of the EPH receptor and Src kinase families. These kinases play a role in both normal cellular functions and pathological processes such as oncogenesis, metastasis, tumor angiogenesis, and maintenance of the tumor microenvironment. The RET M918T mutation in MTC is classified as Level B based on emerging Phase III clinical data (Figure 3).
Level C is divided into two sub-levels: C1 and C2. Level C1 includes alterations that have received FDA/NMPA approval or are recommended by clinical professional guidelines as predictive of response to therapies in different types of tumors. For example, anaplastic lymphoma kinase (ALK) rearrangements are found in 2–7% of non-small-cell lung cancer (NSCLC) patients [12,13]. The FDA has approved several ALK TKIs, including crizotinib, alectinib, ceritinib, brigatinib, and lorlatinib, for treating ALK-positive NSCLC. Studies have also shown that ALK TKIs produce significant clinical responses in ALK-positive non-NSCLC patients [14–21]. The available evidence indicates that targeted therapy may be beneficial for these patients. As a result, ALK rearrangement is classified as Level C1 in non-NSCLC tumors, based on evidence derived from NSCLC. Level C2 includes alterations that predict biomarkers of response to therapies, as established by small retrospective or prospective studies (Phase I or II) in specific types of tumors. Phosphatase and tensin homolog (PTEN) is often deregulated in advanced prostate cancers, leading to the activation of the PI3K-Akt-mTOR pathway and increased cell survival. A Phase II study (NCT00976755) of everolimus, an mTOR inhibitor, was conducted in patients with metastatic castration-resistant prostate cancer. The study found that PTEN deletion was associated with higher disease remission rates and improved progression-free survival (PFS) [22]. According to the emerging Phase II clinical data, PTEN deletion is classified as a Level C2 mutation in prostate cancer (Figure 3).
Level D is subdivided into Levels D1 and D2. These levels include alterations that are candidate predictive biomarkers of response to therapies based solely on a few reported cases in specific tumors (Level D1) or preclinical studies (Level D2). Futibatinib is a potent inhibitor that targets the FGFR family. It has high affinity for FGFR 1, 2, 3, and 4, with IC_50_ values below 4 nM. Futibatinib forms a covalent bond with FGFR, effectively inhibiting FGFR phosphorylation, disrupting downstream signaling pathways, and reducing the viability of cancer cells harboring FGFR alterations, including fusions/rearrangements, amplifications, and mutations. Clinical observations have shown that patients with gastric cancer featuring FGFR2 amplification respond to futibatinib treatment [23,24]. Consequently, in the context of gastric cancer, FGFR2 amplification has been classified as a Level D1 mutation (Figure 3).
OKAIN classifies evidence for resistance into two main levels: R1 and R2. Level R1 includes alterations that have been approved by the FDA/NMPA or recommended by clinical professional guidelines as predictive of resistance to therapies in specific tumors. An example of this is the PDGFRA D842V mutation, which has been shown to cause resistance to imatinib in patients with GISTs (Figure 3). Resistance evidence Level R2 is subdivided into R2B, R2C, and R2D, which correspond to sensitivity evidence levels B, C, and D, respectively. This stratification facilitates the precise weighting of clinical evidence.
Examples of weighted analysis interpretation
3.2
OKAIN logs all clinical data for each genomic alteration, enabling physicians to comprehensively review the therapeutic implications. A single genetic variant may correspond to multiple efficacy levels for a given therapeutic strategy (Figure 4). The evidence analysis system is designed to help physicians obtain conclusive evidence of therapeutic efficacy for cancer patients quickly and succinctly.
Examples of OKAIN weighted analysis interpretation. The level of evidence shows the efficacy for the specific genomic variant related to a particular drug. The Highest Efficacy Level indicates the maximal therapeutic effect for the specific genomic variant in response to a specific drug. The First Weighted Level indicates the ultimate drug efficacy for the specific genomic variant, as determined after applying a weighting analysis. If the Highest Efficacy Level presents conflicting evidence, the system will output “Conflict.” The Second Weighted Level specifies the definitive efficacy for all variants of the gene. If the highest level presents conflicting evidence, the system outputs “Conflict.” The display shows the ultimate efficacy for all variants of the gene related to the drug. “” prompting that the sensitivity of ALK rearrangement and ALK G1269A co-mutation is controversial.*
The FDA/NMPA has approved several ALK TKIs for treating NSCLC patients with ALK rearrangement. Crizotinib, ceritinib, ensartinib, alectinib, brigatinib, and lorlatinib are all designated as Level A for this rearrangement. Additionally, numerous preclinical studies have classified this rearrangement as Level D, predicting sensitivity to ALK TKIs [25–27]. The weighting system prioritizes the highest efficacy level for genomic alterations with multiple levels. Therefore, ALK rearrangement is categorized as Level A for crizotinib, ceritinib, ensartinib, alectinib, brigatinib, and lorlatinib. If conflicting evidence is present for the highest level, the system outputs “Conflict.” As shown in Figure 4, the ALK rearrangement and ALK G1269A co-mutation are classified as Level D and R2D for alectinib, according to various literature sources [28–31]. In this case, the system would output “Conflict” when weighted. OKAIN highlights resistant clinical evidence to ensure patients do not lose valuable treatment time due to potentially ineffective targeted drugs, even if the ALK rearrangement is classified as Level A for alectinib. The co-occurrence of ALK rearrangement and ALK G1269A mutation is ultimately categorized as “Level R2*”, with “” indicating that the sensitivity of this co-mutation to alectinib is controversial. Similarly, ALK rearrangement and ALK G1269A co-mutations are ultimately classified as “Level R2” [32,33]. When the highest level of evidence indicates resistance, the ALK rearrangement and ALK G1269A co-mutations are ultimately classified as Level R2 for crizotinib and entrectinib [25,30,31].
Quantity of evidence in the OKAIN knowledge base
3.3
To date, OKAIN has amassed over 100,000 variants in 1,239 cancer-associated genes, encompassing 12,409 entries of therapeutic evidence in 471 genes. This collection highlights 2,600 Level A evidence entries in 66 genes, with 864 entries derived from either the NMPA label or Chinese guidelines (Table S1). The EGFR, erb-B2 receptor tyrosine kinase 2 (ERBB2/HER2), ALK, KIT, MET proto-oncogene (MET), and B-Raf proto-oncogene (BRAF) genes are associated with the largest numbers of therapeutic evidence (Figure 5a). Lung carcinoma is the largest proportion of therapeutic evidence by tumor type, due to its association with the largest number of therapeutic strategies (Figure 5b).
Distribution of therapeutic evidence. (a) Distribution of therapeutic evidence for genes in OKAIN knowledge base when ranked by the number of interpretations in the database. (b) Distribution of therapeutic evidence for different tumor types in OKAIN knowledge base when ranked by the number of interpretations in the clinical data.
Clinically actionable variations in Chinese patients
3.4
To quantify the potential clinical impact of prospective broad tumor genomic testing, we annotated the variants in a publicly available dataset of 10,194 solid tumors with China Pan-cancer cohort (OrigiMed, Nature 2022) using the OKAIN knowledge base (Version 1.0, 2024) and the OncoKB (http://oncokb.org/, v4.13) knowledge base, respectively [34]. As shown in Figure 6, Tables S2 and S3, the proportions of OKAIN and OncoKB actionability were 74.1% of patients (N = 7,555 harbored at least one gene variant with a variable highest level of clinical evidence, Level A, 34.7%; Level B, 0.8%; Level C, 20.5%; Level D, 18.2%) and 67.8% (N = 6,911, Level 1, 34.5%; Level 2, 1.0%; Level 3, 19.4%; Level 4, 12.9%), respectively. Complete concordance in clinical actionability annotations was observed, with all 6,911 OncoKB-annotated actionable cases similarly classified as actionable by OAKIN. McNemar’s test was used to assess inter-system differences. Relative to OncoKB, the OKAIN knowledge base demonstrated significantly broader patient coverage (74.1 vs 67.8%; P < 0.001) for targeted or immunotherapeutic eligibility, reflecting its systematic evidence aggregation framework for genomic aberration-specific efficacy data.
Clinical actionability of somatic variants in the China Pan-cancer cohort. Variants were assigned to different levels of clinical actionability according to OKAIN knowledge base. (a) Distribution of the highest level of actionable variants across all patients. (b) Distribution of highest level of actionable variants across tumor types.
Discrepancies between OncoKB and OKAIN in identifying patients for therapies and drug sensitivities to actionable variants are highlighted by differences in their clinical assessment and evidence integration (Tables S4, S5 and S6). These variations may stem from OKAIN’s inclusion of additional clinical factors, such as hormone receptor (HR) and HER2 status, in its assessment criteria. The FDA’s approval of capivasertib, in combination with fulvestrant for adult patients with HR-positive, HER2-negative locally advanced or metastatic breast cancer with PIK3CA/AKT1/PTEN-alterations post-progression on endocrine therapy, underscores the significance of these factors. When a patient’s HR or HER2 status is either unknown or not HR-positive and HER2-negative, the evidence level assigned to capivasertib for treating breast cancer is adjusted to Level C. Additionally, it may stem from the inclusion of drugs approved in China and recommended by the Chinese Society of Clinical Oncology (CSCO) guidelines (https://www.csco.org.cn/) in OKAIN, which are not listed in OncoKB, such as almonertinib. Moreover, OKAIN’s consideration of a broader evidence base may explain these differences. For example, based on clinical trial data, patients with renal cell carcinoma who have Von Hippel-Lindau tumor suppressor (VHL) alterations may benefit from treatments like sunitinib, sorafenib, bevacizumab, or axitinib [35]. Concurrently, preclinical findings indicate that GISTs harboring the KIT A502_Y503dup mutation may be less responsive to imatinib therapy [36].
Discussion
4
The adoption of NGS in clinical genetic testing has become widespread, leading to the discovery of numerous genetic variants that may impact clinical decision-making. This highlights the significance and advantages of standardized interpretation of these variants [9]. There are several resources available to aid in the clinical interpretation of genetic alterations, such as CIViC [4], OncoKB [5], COSMIC [37], the JAX Clinical Knowledge base [38], the Cancer Driver Log [39], and the Precision Medicine Knowledge Base [40]. These databases offer either the final clinical annotation results or multiple pieces of clinical interpretation evidence related to the alterations. However, until now, there has been a lack of databases published specifically to interpret genetic variants in China. In this context, OKAIN emerges as the first precision oncology knowledge base published in China. This resource offers physicians detailed and structured interpretations of cancer mutations found in patient tumors, along with evidence of therapeutic efficacy through a weighted analysis system. Its potential to enhance precision oncology practice in China is significant.
Like other classification systems [5,9], OKAIN divides the sensitivity evidence into four levels for each mutation, based on the available clinical and preclinical data that support the use of the mutation as a predictive biomarker. The evidence sensitivity levels, ranked from highest to lowest, are A, B, C, and D. Therapeutic implications approved by FDA/NMPA or recommended by clinical professional guidelines for specific tumors are classified as level A. All other therapeutic implications are classified as levels B, C, and D, respectively. The significance of the latter lies in its potential to offer new therapeutic strategies for cancer patients, including off-label use of cancer drugs and enrollment in appropriate clinical trials. However, we do not recommend using cancer drugs off-label for different tumor types due to the limited evidence supporting their efficacy. It is important to consider the safety profile and accessibility of these medications as well as the variability in their effectiveness across different tumors. For example, the results of a phase II trial (NCT00903175) demonstrate the variability of patient outcomes when treated with everolimus for renal cell carcinoma. Patients who retained PTEN expression had a median PFS of 5.3 months, while those who lost PTEN expression experienced a significantly longer median PFS of 10.5 months (P < 0.001) [41]. This finding suggests that PTEN status may have predictive value in this context. In contrast, data from another study on transitional cell carcinoma suggest that PTEN loss may be associated with resistance to everolimus. This indicates that the efficacy of this drug is not consistent across different tumor types and that molecular profiles should be carefully considered before off-label application [42].
Although clinical and preclinical studies suggest that certain gene mutations may respond to specific targeted drugs, it is important to note that the gene may not actually be the target of the drug. Currently, there is insufficient research to explain this phenomenon adequately. For example, biomarker analyses of the BERIL-1 trial showed that patients with squamous cell carcinoma of the head and neck, who also had TP53 alterations, benefited from the combination of buparlisib and paclitaxel in terms of survival [43]. However, further investigation is required to establish a definitive link between TP53 alterations and improved outcomes with this drug combination. Therefore, although TP53 alterations are not currently considered agents in OKAIN, they are still recorded for reference.
OKAIN continuously records new clinical data, including updates to NMPA/FDA labels, professional guidelines, and scientific literature, ensuring that the weighted level of evidence remains current. For example, RET rearrangement was not considered as level A in thyroid cancer until December 1, 2020, when the FDA approved pralsetinib for the treatment of adult and pediatric patients (12 years of age and older) with advanced or metastatic RET fusion-positive thyroid cancer who require systemic therapy and are radioactive iodine-refractory. This timely inclusion of new clinical data enhances the utility of OKAIN for making informed therapeutic decisions.
OKAIN plans to conduct weighted analyses for complex variants, including multiple genetic variants, rather than solely focusing on single-gene alterations. Additionally, they aim to establish a platform where physicians can engage in discussions and provide comments on variant annotations, aiding in their accurate understanding of these alterations.
OKAIN has entered clinical practice across multiple settings, supporting critical oncology workflows including: (1) interpretation of NGS reports to deliver clinically actionable results, (2) genetic counseling sessions, and (3) Molecular Tumor Board discussions by providing evidence for therapeutic decision-making. Ongoing real-world studies are quantitatively assessing OKAIN’s implementation fidelity, impact on therapeutic recommendations, and broader utility in precision oncology pathways.
Conclusions
5
OKAIN is a knowledge base for cancer genomics and precision treatment, including therapies approved in China and those recommended by Chinese clinical guidelines. OKAIN presents an extensive array of evidence, enhanced by a specialized weighting system, facilitating precision treatment for clinicians and patients with complex variations. Analyzing patient variants with OKAIN reveals more actionable targeted therapy or immunotherapy options, potentially improving treatment outcomes.
Supplementary Material
Supplementary Table