Early Outcomes of Transcatheter Aortic Valve Implantation for Severe Aortic Stenosis With Myval Versus Edwards Sapien 3 Valve: A Systematic Review and Meta-Analysis
Dinkar Bhasin, Ankita Bhasin, Tsering Sangdup, Arun Sharma, Prashant Panda, Yash Paul Sharma

TL;DR
This study compares two heart valve systems for treating severe aortic stenosis and finds similar safety outcomes but better performance with one valve.
Contribution
A systematic review and meta-analysis comparing clinical and hemodynamic outcomes of two balloon-expandable transcatheter heart valves.
Findings
No significant difference in mortality, pacemaker implantation, or vascular complications between Myval and Edwards Sapien 3 valves.
Myval showed better hemodynamic performance with lower mean gradient and larger effective orifice area.
Myval was associated with higher rates of moderate to severe aortic regurgitation and new-onset atrial fibrillation.
Abstract
The Edwards Sapien (Edwards Lifesciences, Irvine, CA, USA) transcatheter heart valves (THVs) and the Myval THVs (Meril Life Sciences, Vapi, Gujarat, India) are two balloon-expandable valve systems used for transcatheter aortic valve implantation (TAVI). This systematic review and meta-analysis aimed to compare the clinical and hemodynamic outcomes at 30 days after TAVI using the Myval versus the Edwards Sapien 3 valve in patients with severe aortic stenosis (AS). We conducted a systematic search of PubMed, Embase, Cochrane Library, and clinicaltrials.gov up to June 21, 2025. The inclusion criteria were observational studies or interventional trials comparing Myval or Myval Octacor with Edwards Sapien 3 or Sapien 3 Ultra in patients with severe AS undergoing TAVI. The risk of bias was assessed using the Cochrane Risk of Bias Tool 2 for randomized controlled trials (RCTs) and the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
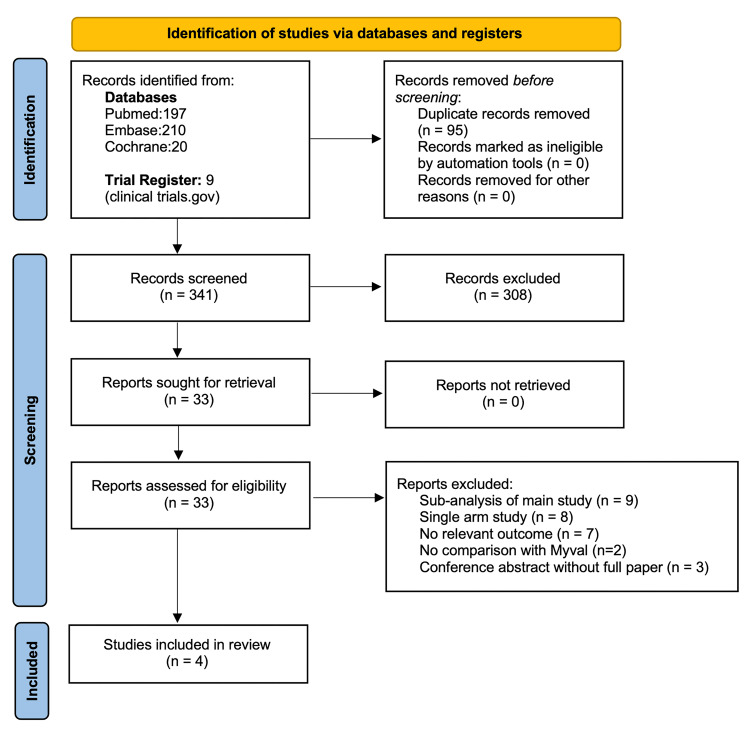 Figure 1
Figure 1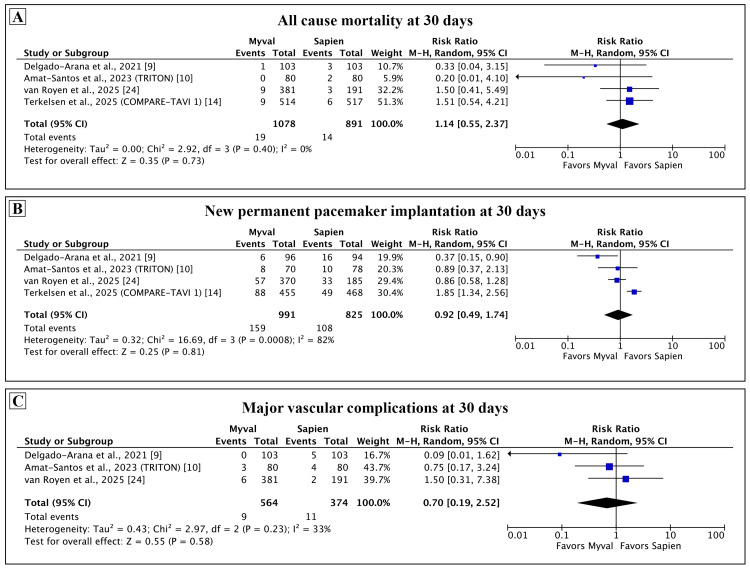 Figure 2
Figure 2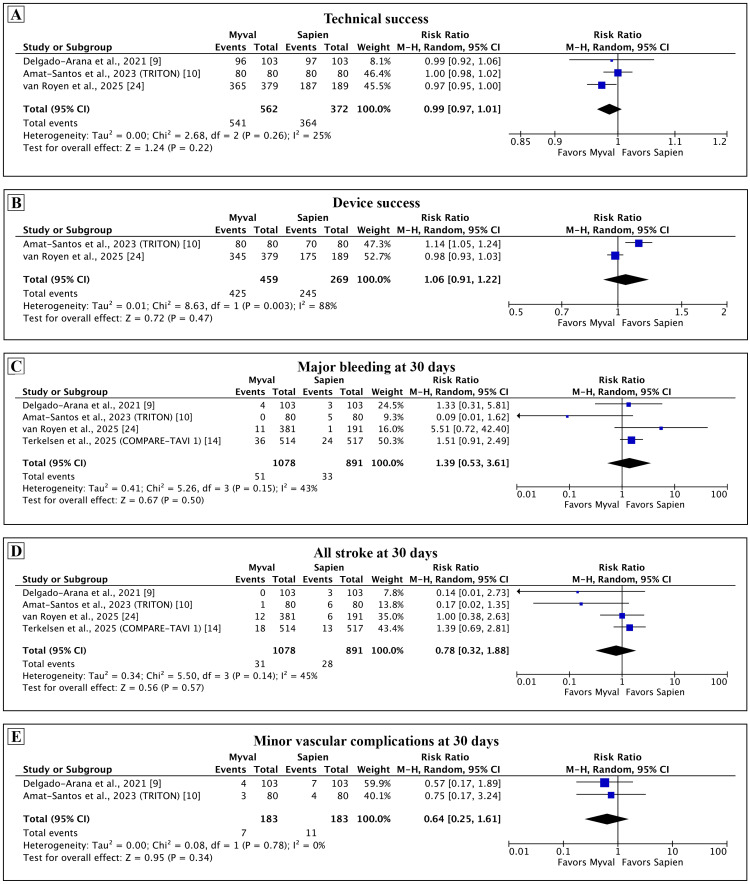 Figure 3
Figure 3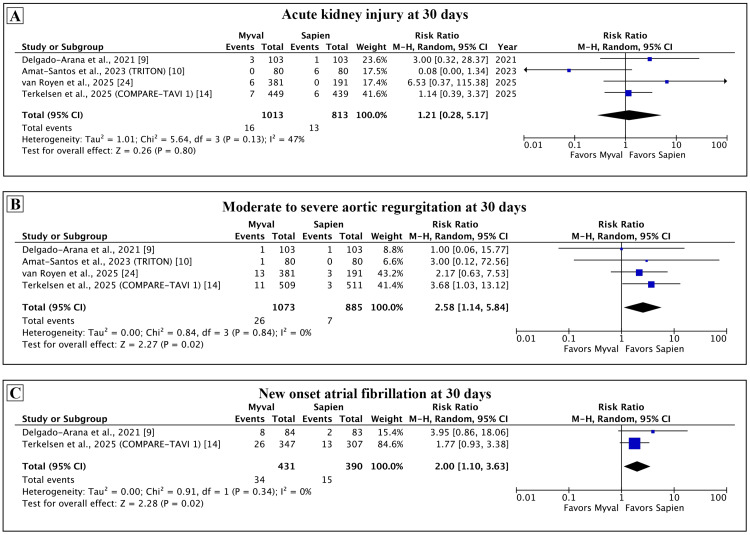 Figure 4
Figure 4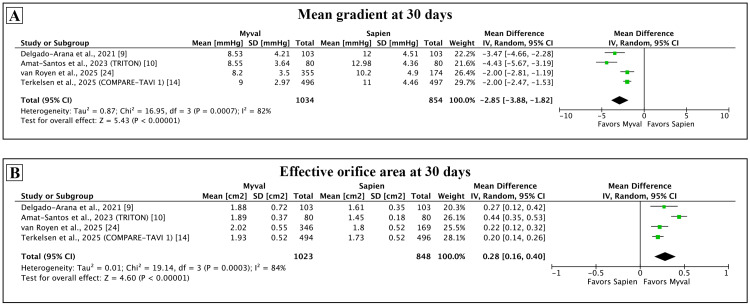 Figure 5
Figure 5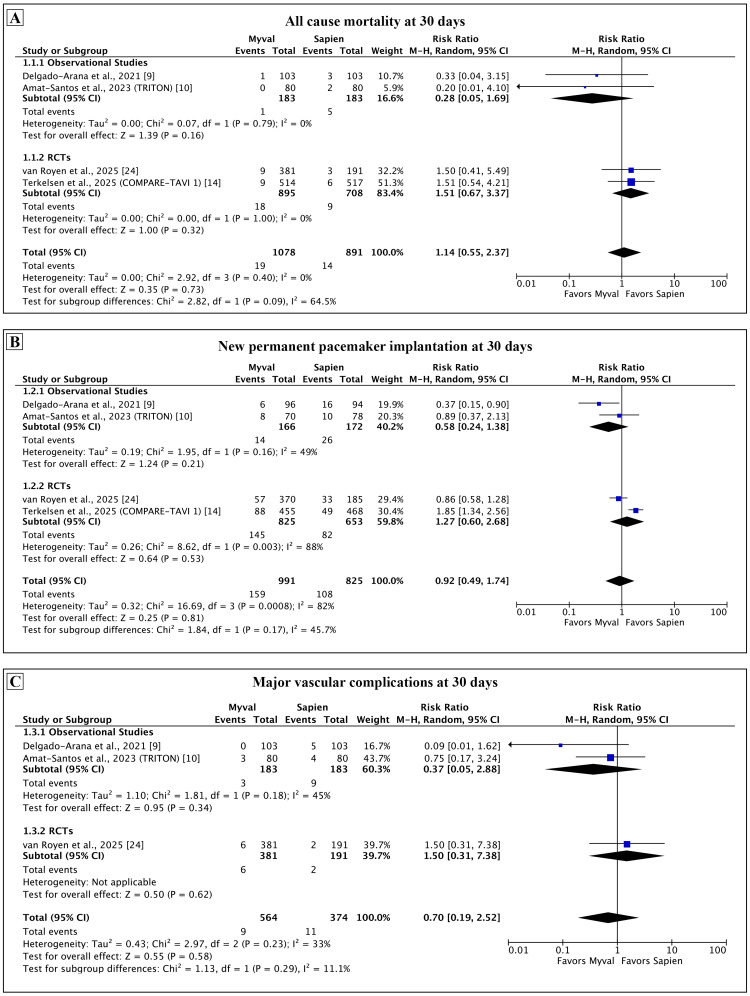 Figure 6
Figure 6| Study authors and year | Year | Location | Centers | Study design | Intervention | Comparator | VARC criteria | Myval (n) | Sapien 3 (n) | Follow-up |
| Delgado-Arana et al. 2021 [ | 2021 | Europe | Muticentric | Observational; matched retrospective cohort | Myval | Edwards Sapien 3 | 2 | 103 | 103 | 30 days |
| Amat-Santos et al. 2023 (TRITON) [ | 2023 | Europe | Multicentric | Observational; matched retrospective registry-based cohort | Myval | Edwards Sapien 3 | 3 | 80 | 80 | 30 days |
| van Royen et al. 2025 (LANDMARK study) [ | 2025 | Europe, Brazil, New Zealand | Multicentric | Randomized, open-label trial | Myval (91.3%) and Myval Octacor (8.7%) | Edwards Sapien 3 (55.4%) or Edwards Sapien 3 Ultra (44.6%) | 3 | 384 | 192 | 30 days |
| Terkelsen et al. 2025 (COMPARE-TAVI 1) [ | 2025 | Denmark | Multicentric | Randomized, open-label trial | Myval (36%) and Myval Octacor (63%) | Edwards Sapien 3 and Sapien 3 Ultra | 3 | 514 | 517 | 30 days, one year |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Valve Diseases and Treatments · Aortic Disease and Treatment Approaches · Cardiovascular Function and Risk Factors
Introduction and background
Aortic stenosis (AS) is a progressive, degenerative disease of the aortic valve [1]. In elderly patients with symptomatic severe AS, transcatheter aortic valve implantation (TAVI) is the preferred treatment modality in those with suitable anatomy and acceptable procedural risk [2]. TAVI is less invasive than surgical aortic valve replacement and has demonstrated comparable clinical outcomes [3,4]. Various transcatheter heart valves (THVs) have been developed and approved for TAVI, being broadly categorized into balloon-expandable and self-expanding valves.
Among balloon-expandable valves, Edwards Sapien valve series (Edwards Lifesciences, Irvine, CA, USA) is widely used with extensive clinical data [5,6]. Myval THV (Meril Life Sciences, Vapi, Gujarat, India) is a newer balloon-expandable valve that received its CE-mark in 2019 [7]. It has gained attention due to its catheter design with the valve pre-mounted on the balloon and its availability in intermediate sizes [7].
Clinical endpoints for TAVI, as defined by the Valve Academic Research Consortium, provide a standardized framework for evaluating procedural success and clinical outcomes of the TAVI procedure [8]. Comparative evaluation of different THVs using these endpoints is crucial for guiding evidence-based valve selection in clinical practice. Multiple observational studies and at least two major randomized controlled trials have compared the newer Myval valve with contemporary THVs, including Sapien and Evolut [9-14].
The existing studies have limited sample sizes, were powered for composite outcomes, and employed varying endpoint definitions. Hence, we conducted a systematic review and meta-analysis to pool the available evidence comparing early clinical and hemodynamic outcomes in patients undergoing TAVI for severe AS with Myval versus Edwards Sapien 3 THVs.
Review
Methods
This study was conducted in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines [15]. The protocol was prospectively registered in the INPLASY database (INPLASY202560110).
Literature Search
The search was conducted on 21st June 2025, on PubMed, Embase, and Cochrane Central Register of Controlled Trials (CENTRAL) through the Cochrane Library. The trial register, clinicaltrials.gov, was also searched. The search comprised of the broad terms: ‘TAVI,’ “trans-catheter aortic valve implantation,” “transcatheter aortic valve replacement,” “TAVR,” “Myval,” and “Myval valve,” “Myval Octacor,” and “aortic stenosis.” The search string was generated by utilizing controlled vocabulary, such as MeSH and Emtree, free text keywords, and synonyms without any restrictions. The elaborative search strategy is presented in the Appendix (see Table 2).
Eligibility Criteria
Eligible studies included either observational studies or interventional trials comparing Myval or Myval Octacor valve with the Edwards Sapien 3 valve series (Sapien 3 or Sapien 3 Ultra) in patients with severe AS undergoing TAVI. To be eligible, the study should have been published in peer-reviewed journal and evaluated at least one of the primary or secondary outcomes.
Outcomes
The primary outcomes were assessed at 30 days and included all-cause mortality, new permanent pacemaker implantation (PPI), and major vascular complications. The secondary outcomes were technical success, device success, major bleeding, all strokes, minor vascular complications, significant acute kidney injury (AKI), moderate to severe aortic regurgitation (AR), new-onset atrial fibrillation (AF), and hemodynamic parameters, including mean gradient and effective orifice area (EOA), with all outcomes being assessed at 30 days. Outcomes were defined as per the Valve Academic Research Consortium (VARC) criteria [8]. In addition, as an exploratory analysis, we also compared the procedural outcomes of procedural death, annular rupture, coronary occlusion, valve malposition, and tamponade by pooling data from eligible studies.
Study Selection and Data Extraction
The results yielded by the search strategy were collated and duplicates removed. Full texts of the shortlisted studies were retrieved. The deduplicated reports were independently screened using the title and abstract. Relevant data from the eligible reports were extracted in a predefined data entry form. This included study identifiers, study and baseline patient characteristics, procedural details, and outcome data of three primary, ten secondary, and procedural outcomes. All steps were independently performed by two reviewers (A.B. and D.B.). Discrepancies were resolved through discussion with a third reviewer (T.S.).
Risk of Bias Assessment
Assessment for risk of bias was done independently by two reviewers (A.B. and D.B.) using the Cochrane Risk of Bias Tool 2 (RoB 2) for randomized controlled trials (RCTs) and the Newcastle-Ottawa Scale (NOS) for observational studies [16,17]. Any disagreements were resolved through discussion with a third reviewer (T.S.).
Data Synthesis and Analysis
For dichotomous variables, effect estimates were calculated as risk ratios (RRs) with 95% confidence intervals (CI), and continuous data were represented using mean difference and standard deviation. Pooled estimates were derived using a random-effects model and summarized in the forest plot with 95% CI. Wherever the original study reported median with interquartile range, it was converted into mean ± standard deviation using recommended formulas [18,19]. Heterogeneity between the studies was analyzed using the Cochran's Q test and expressed as the I² statistic. The interpretation of I² values was done as recommended by the Cochrane Handbook [20]. If the value of I^2^ was between 0% and 40% heterogeneity may not be important; between 30% and 60% may suggest a moderate degree of heterogeneity; 50% and 90% suggest a presence of substantial heterogeneity; and 75% and 100% suggest a considerable degree of heterogeneity [20].
A predefined subgroup analysis was performed by grouping RCTs and observational studies separately. The analysis was performed where at least two studies were present in either subgroup. Sensitivity analysis was performed for the primary outcome using a leave-one-out approach [21].
The software and online tools used at various stages of the review included Rayyan, EndNote (Clarivate, Philadelphia, PA), and Review Manager from the Cochrane Collaboration [22]. Data synthesis was performed by using RevMan 5 (Review Manager (RevMan), (Computer program), Version 5.4, The Cochrane Collaboration, 2020). The RoB 2 plots were generated using the online robvis tool [23].
Results
Search Results
The database search yielded 436 results. Ninety-five duplicates were removed. Titles and abstracts of 341 reports were screened against the eligibility criteria, and 308 reports were excluded. The full texts of 33 reports were reviewed, yielding four eligible studies for the systematic review [9,10,14,24]. The flow is summarized in the PRISMA flow diagram in Figure 1. Two other studies, Santos-Martinez et al. and Ubben et al., compared in-hospital outcomes between Myval and Sapien 3 but did not report any 30-day outcomes [11,12]. Hence, they were excluded from the systematic review. Details of excluded studies are provided in the Appendix (see Table 3).
PRISMA flow diagram.PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Study and Baseline Patient Characteristics
A total of four studies, two RCTs and two retrospective cohort studies, involving 1973 patients, were included in the review [9,10,14,24]. Two RCTs contributed 1607 patients (81.4%) while the observational studies contributed 366 patients (18.6%). Of the entire patient pool, 1081 (54.8%) received Myval and 892 (45.2%) received Sapien 3. All studies were multicentric with predominant participation of European centers. All studies were published between 2021 and 2025.
Among the observational studies, Delgado-Arana et al. excluded bicuspid aortic valves, while the TRITON study only included patients with bicuspid aortic valves [9,10]. The RCTs, COMPARE-TAVI 1 trial, and the LANDMARK substudy comparing Sapien 3 and Myval as reported by van Royen et al., included patients with tricuspid and bicuspid aortic valves, with the proportion of the latter being <10% [14,24]. The COMPARE-TAVI 1 being an all-comers RCT also included patients undergoing valve-in-valve procedures, amounting to 4% of the population [14].
Three out of the four studies used the VARC-3 criteria for assessing outcomes, except for Delgado-Arana et al., which reported the outcomes according to the VARC-2 criteria [25]. Basic study characteristics are summarized in Table 1. Other details, including endpoints and inclusion criteria, are presented in the Appendix (see Table 4).
Table 1: Characteristics of included studies.VARC: Valve Academic Research Consortium.
<table><tbody><tr><td rowspan="1" colspan="1">Study authors and year</td><td rowspan="1" colspan="1">Year</td><td rowspan="1" colspan="1">Location</td><td rowspan="1" colspan="1">Centers</td><td rowspan="1" colspan="1">Study design</td><td rowspan="1" colspan="1">Intervention</td><td rowspan="1" colspan="1">Comparator</td><td rowspan="1" colspan="1">VARC criteria</td><td rowspan="1" colspan="1">Myval (n)</td><td rowspan="1" colspan="1">Sapien 3 (n)</td><td rowspan="1" colspan="1">Follow-up</td></tr><tr><td rowspan="1" colspan="1">Delgado-Arana et al. 2021 [<xref>9</xref>]</td><td rowspan="1" colspan="1">2021</td><td rowspan="1" colspan="1">Europe</td><td rowspan="1" colspan="1">Muticentric</td><td rowspan="1" colspan="1">Observational; matched retrospective cohort</td><td rowspan="1" colspan="1">Myval</td><td rowspan="1" colspan="1">Edwards Sapien 3</td><td rowspan="1" colspan="1">2</td><td rowspan="1" colspan="1">103</td><td rowspan="1" colspan="1">103</td><td rowspan="1" colspan="1">30 days</td></tr><tr><td rowspan="1" colspan="1">Amat-Santos et al. 2023 (TRITON) [<xref>10</xref>]</td><td rowspan="1" colspan="1">2023</td><td rowspan="1" colspan="1">Europe</td><td rowspan="1" colspan="1">Multicentric</td><td rowspan="1" colspan="1">Observational; matched retrospective registry-based cohort</td><td rowspan="1" colspan="1">Myval</td><td rowspan="1" colspan="1">Edwards Sapien 3</td><td rowspan="1" colspan="1">3</td><td rowspan="1" colspan="1">80</td><td rowspan="1" colspan="1">80</td><td rowspan="1" colspan="1">30 days</td></tr><tr><td rowspan="1" colspan="1">van Royen et al. 2025 (LANDMARK study) [<xref>24</xref>]</td><td rowspan="1" colspan="1">2025</td><td rowspan="1" colspan="1">Europe, Brazil, New Zealand</td><td rowspan="1" colspan="1">Multicentric</td><td rowspan="1" colspan="1">Randomized, open-label trial</td><td rowspan="1" colspan="1">Myval (91.3%) and Myval Octacor (8.7%)</td><td rowspan="1" colspan="1">Edwards Sapien 3 (55.4%) or Edwards Sapien 3 Ultra (44.6%)</td><td rowspan="1" colspan="1">3</td><td rowspan="1" colspan="1">384</td><td rowspan="1" colspan="1">192</td><td rowspan="1" colspan="1">30 days</td></tr><tr><td rowspan="1" colspan="1">Terkelsen et al. 2025 (COMPARE-TAVI 1) [<xref>14</xref>]</td><td rowspan="1" colspan="1">2025</td><td rowspan="1" colspan="1">Denmark</td><td rowspan="1" colspan="1">Multicentric</td><td rowspan="1" colspan="1">Randomized, open-label trial</td><td rowspan="1" colspan="1">Myval (36%) and Myval Octacor (63%)</td><td rowspan="1" colspan="1">Edwards Sapien 3 and Sapien 3 Ultra</td><td rowspan="1" colspan="1">3</td><td rowspan="1" colspan="1">514</td><td rowspan="1" colspan="1">517</td><td rowspan="1" colspan="1">30 days, one year</td></tr></tbody></table>The average age of patients in all the studies was over 80 years, with the exception of the TRITON study, where the mean age was 77 years, possibly because it only recruited patients with bicuspid aortic valve who present at a younger age [10]. Over 40% of patients had a functional class of New York Heart Association (NYHA) class III or IV in three of the four studies that reported it. The mean Society of Thoracic Surgeons (STS) score was less than 4% in all four studies, suggesting an overall intermediate-risk population. Relevant baseline characteristics of the study patients, including clinical, echocardiographic, and computed tomography parameters, have been summarized in the Appendix (see Tables 5-7).
Procedural characteristics were similar across the studies except for some differences. Three of the four studies used only transfemoral access, except for van Royen et al., in which alternative access was used in <2% of patients [24]. Predilation was done more often in the Myval group, in almost 40% of the patients, except for the TRITON study, where it was done in over 70% patients [10]. Intermediate sizes were used in over 40% of the patients receiving Myval in individual studies, except for the TRITON study, where the figure was 25% [10]. The procedural characteristics across the studies are presented in the Appendix (see Table 8).
Risk of Bias Assessment
The RoB 2 tool was used at the outcome level. There were some concerns with regards to the risk of bias for both studies across all outcomes. The LANDMARK trial had some concerns due to deviation from the intended intervention, as 4% of patients in the Myval group received Sapien 3 [24]. The COMPARE-TAVI 1 study had some concerns in the selection of reported results, as there was no predefined protocol and statistical analysis plan for the study [14]. The RoB 2 assessment for various outcomes is presented in the Appendix (see Figure 7). Both the observational studies, Delgado-Arana et al. and the TRITON study were of high quality as assessed using the NOS. The NOS score for various domains is summarized in the Appendix (see Table 9).
Quantitative Synthesis
Primary outcomes: The findings of the meta-analysis for the primary outcome at 30 days are presented in Figure 2. There was no statistical difference in the pooled estimate of all-cause mortality (RR: 1.14, 95% CI: 0.55-2.37; p = 0.73; I² = 0%). The finding was consistent across all studies, and heterogeneity for this comparison was low. Three out of four studies reported the rate of PPI as a proportion of all patients in each arm and did not exclude those with pre-existing PPI. We calculated the rate of new PPI in each study as a proportion of patients without pre-existing PPI that received PPI after TAVI. The pooled estimate of new PPI at 30 days was similar between the two groups (RR: 0.92, 95% CI: 0.49-1.74; p = 0.81; I² = 82%). Sensitivity analysis for this outcome was performed by using the originally reported rates of new PPI in the individual studies and showed similar findings (see Appendix, Figure 8). The rate of major vascular complications was comparable with low levels of heterogeneity (RR: 0.70, 95% CI: 0.19-2.52; p = 0.58; I² = 33%).
Comparison of primary outcomes between Myval and Sapien 3 at 30 days.Meta-analysis of the primary outcomes of all-cause mortality (A), new permanent pacemaker implantation (B), and major vascular complications (C).
Secondary outcomes: Among the secondary outcomes assessed at 30 days (Figures 3, 4), there was no difference between Myval and Sapien in the technical success (RR: 0.99, 95% CI: 0.97-1.01; p = 0.22; I² = 25%), device success (RR: 1.06, 95% CI: 0.91-1.22; p = 0.47; I² =88%), major bleeding (RR: 1.39, 95% CI: 0.53-3.61; p = 0.50; I² = 43%), all stroke (RR: 0.78, 95% CI: 0.32-1.88; p = 0.57; I² = 45%), minor vascular complications (RR: 0.64, 95% CI: 0.25-1.61; p = 0.34; I² = 0%), and AKI (RR: 1.21, 95% CI: 0.28-5.17; p = 0.80; I² = 47%). Moderate to severe AR (RR: 2.58, 95% CI: 1.14-5.84; p = 0.02; I² = 0%) and new-onset AF (RR: 2.0, 95% CI: 1.10-3.63; p = 0.02; I² = 0%) were more common with Myval as compared with the Sapien.
Comparison of secondary outcomes between Myval and Sapien 3 at 30 days.Meta-analysis of the secondary outcomes of technical success (A), device success (B), major bleeding (C), all stroke (D), and minor vascular complications (E).Major bleeding in COMPARE TAVI-1 and van Royen et al. was Valve Academic Research Criteria (VARC) 3, 4 bleeding. The TRITON trial reported VARC 2 or higher bleeding.TAVI: transcatheter aortic valve implantation.
Comparison of secondary outcomes between Myval and Sapien 3 at 30 days.Meta-analysis of the secondary outcomes of acute kidney injury (A), moderate to severe aortic regurgitation (B), and new-onset atrial fibrillation (C).The rate of new-onset atrial fibrillation for Delgado-Arana et al. was calculated by excluding the patients with pre-existing atrial fibrillation.
Among the hemodynamic outcomes (Figure 5), the mean gradient was lower (mean difference: -2.85 mmHg, 95% CI: -3.88 to -1.82 mmHg; p < 0.001; I² = 82%) and the EOA was larger with the Myval (mean difference: 0.28 cm^2^, 95% CI: 0.16-0.40 cm^2^; p < 0.001; I² = 84%). These findings were consistent across all individual studies.
Comparison of hemodynamic outcomes between Myval and Sapien 3 at 30 days.Meta-analysis of the hemodynamic outcomes of mean gradient (A) and effective orifice area (B).
The exploratory analysis of procedural outcomes is presented in the Appendix (see Figure 9). There was no difference in any outcome with similar rates of procedural death (RR: 0.62, 95% CI: 0.12-3.22; p = 0.57; I² = 0%), annular rupture (RR: 0.20, 95% CI: 0.03-1.15; p = 0.07; I² = 0%), coronary occlusion (RR: 0.52, 95% CI: 0.08-3.30; p = 0.49; I² = 18%), valve malposition (RR: 0.62, 95% CI: 0.08-5.06; p = 0.66; I² = 0%) and tamponade (RR: 0.50, 95% CI: 0.19-1.27; p = 0.14; I² = 0%).
Subgroup Analysis and Sensitivity Analysis
A predefined subgroup analysis was conducted by grouping RCTs and observational studies separately. The findings of the subgroup analysis for the primary outcomes are presented in Figure 6. There were no significant differences in any primary outcome among the subgroups. The subgroup analysis for the secondary outcomes is presented in the Appendix (see Figures 10-12). We observed inconsistency in outcomes of all strokes at 30 days and moderate to severe AR between the two subgroups, but this difference could be explained by the low event rates and small sample size in the observational studies.
Subgroup analysis for the primary outcomes.Subgroup analysis of the primary outcome based on study type.
A sensitivity analysis for the primary outcomes was performed using the leave-one-out approach (see Appendix, Figures 13-15). The findings remained consistent, suggesting no individual study unduly influenced the results.
Publication Bias
As only four studies were included in the review, a funnel plot could not be utilized to assess for publication bias [26].
Discussion
The present systematic review compared the early clinical outcomes between Myval and Sapien 3 THVs. There was no difference in the primary outcomes of all-cause mortality, permanent pacemaker implantation, and major vascular complications assessed at 30 days. Among the secondary outcomes, moderate to severe AR and new-onset AF were more common with Myval. The mean gradient was lower and EOA larger in Myval as compared to Sapien 3.
Both valves are balloon expandable but with different valve and delivery catheter designs [7]. Myval utilizes a nickel-cobalt alloy frame, whereas the Sapien 3 series features a frame of cobalt-chromium alloy. Furthermore, unlike the Sapien valve, the Myval catheter system does not employ a pusher, and the valve is directly crimped on the balloon. While this permits the undeployed valve to be removed from the body if required, the absence of a pusher may result in less pushability of the device. Hence, there is a trend towards more valve predilation when using the Myval as compared to the Sapien 3. Both valves use proprietary expandable sheaths. Myval's Python sheath has a fixed 14F size for all devices, while the Sapien Sheath comes in 14F and 16F sizes, depending upon the valve size.
Despite differences between the valve systems, the findings of our meta-analysis suggest that important early outcomes between Myval and Sapien 3 are comparable. Moderate to severe AR was more frequent after the Myval, but this appears to be driven by an unusually low rate of AR in the Sapien group (0.8%). The absolute pooled incidence in the Myval group at 2.4% is similar to the previously reported rates of clinically relevant paravalvular leak with Sapien 3 valves [5,27,28]. The rate of new-onset AF in the Myval group was nearly double that of Sapien 3; however, the possible reasons for this finding and its clinical significance remain unclear.
A notable finding from the present review is the superior hemodynamic performance of the Myval at 30 days. The pooled estimate of the mean difference in EOA was 0.28 cm^2^, with the lower limit of the CI being 0.16 cm^2^. This effect was consistent across all studies. While there is no well-established minimal clinically important difference for EOA, any increment in valve area provides a hemodynamic head start and may be associated with improved valve longevity. Medium and long-term follow-up data with the Myval are limited; however, the COMPARE-TAVI 1 study showed that at one year of follow-up, the Myval group continued to have a lower mean gradient and larger EOA [14]. The superior hemodynamic performance may be explained by the availability of intermediate sizes in the Myval valve size matrix, which were employed in over 40% of the Myval group in three of the four included studies [29]. It remains to be studied, if this hemodynamic benefit observed at the study level and attributable to the use of intermediate Myval sizes, will extend at individual patient level when comparing corresponding sizes of Myval and Sapien 3.
Of the four studies included in meta-analysis for new PPI at 30 days, all except the COMPARE-TAVI 1 reported the rates of PPI as a proportion of the entire study group. This contrasts with the VARC 3 recommendation, which advises for excluding patients with existing PPIs from the denominator when calculating the rate of new PPIs [8]. We computed the pooled result by excluding patients with existing PPI in the individual studies and found no difference in the rates of PPI at 30 days.
To our knowledge, the present systematic review is the first one that directly compares two commercially available balloon-expandable valves. Two previous systematic reviews have compared Myval to contemporary valves, including Evolut and Sapien [30,31]. These systematic reviews had broad research questions. Quantitative synthesis was performed by pooling outcomes from both self-expanding and balloon-expanding valves in the control group, leading to significant clinical heterogeneity that dilutes any inference from the pooled estimates [32]. This may explain the contrasting findings in our meta-analysis as compared to the previous ones, which reported lower rates of PPI and higher procedural success with Myval based on a pooled comparison with all other types of contemporary valves. Furthermore, these meta-analyses calculated the PPI rates as a proportion of the total study size, without excluding patients with pre-existing PPIs as required by the VARC-3 definitions [8]. Additionally, the recently published COMPARE-TAVI 1 trial was not included in these systematic reviews.
The strengths of the present review include a robust methodology, prospective protocol registration, and execution in accordance with the PRISMA guidelines. The search strategy was comprehensive, and the inclusion criteria were well-defined. All crucial steps were independently performed by two reviewers. A predefined subgroup analysis was performed, and the ROB 2 tool was used at the outcome level to assess risk of bias.
Limitations of this review include significant methodological, clinical, and statistical heterogeneity among the included studies. There were two observational studies and two RCTs, resulting in methodological heterogeneity. We accounted for this by performing subgroup analysis for the observational studies and RCTs with consistent results for the primary outcome. There was significant clinical heterogeneity among the studies, including differences in the populations studied, operator expertise, and the types of valves used. The TRITON study only included patients with bicuspid aortic valves, while Delgado-Arana et al. excluded patients with bicuspid aortic valves. COMPARE-TAVI was an all-comers study, which also included prosthetic heart valves, while all other studies excluded PHVs. Both first-generation Myval and Myval Octacor were used in LANDMARK and COMPARE TAVI, whereas the other studies utilized the first-generation Myval. The LANDMARK and COMPARE TAVI 1 study also used Sapien 3 Ultra in addition to the Sapien 3 valve. Further, the proportion of intermediate sizes used in the Myval group varied among the studies. All these variables can account for the significant heterogeneity that may not be captured by statistical tests. Nonetheless, despite these factors, we believe a quantitative synthesis was essential to provide pooled estimates of outcomes.
The risk of bias assessment was challenging due to use of different scales for observational studies and RCTs. The observational studies with matched comparison were adjudged to be of high quality according to the NOS; however, a retrospective study design can result in several biases that may not be captured by the NOS [33]. Among the RCTs, both had some concerns with regards to the risk of bias. The LANDMARK trial had some concerns due to deviation from the intended intervention, while the COMPARE-TAVI 1 study had some concerns arising out of risk of bias in the selection of reported results [14,24].
Our study carries implications for future research. A medium and long-term follow-up of patients undergoing TAVI with Myval is necessary. A recent retrospective analysis demonstrated that the latest iteration of the Sapien 3 Ultra Resilia valve has similar hemodynamic outcomes compared to the Myval [34]. Likewise, the second-generation Myval Octacor also has certain advantages, including larger skirt size, decreased foreshortening, and the option for commissural alignment, which may theoretically improve hemodynamic performance over the long term [35,36]. Hence, a direct comparison between Myval Octacor and Sapien 3 Ultra Resilia may be relevant to inform future practice. As both THV systems have significant design differences and, therefore, likely costs, a cost-effectiveness analysis of Myval versus Sapien 3 is also warranted.
Conclusions
To conclude, in this systematic review and meta-analysis, we report early outcomes with Myval compared to the Sapien 3 valve for TAVI in severe AS. There was no difference in the primary clinical outcomes at 30 days, with comparable rates of all-cause mortality, new PPI, and major vascular complications between the two valve systems. Moderate to severe AR and new-onset AF were lower with Sapien 3. Myval had a better hemodynamic performance with a lower mean gradient and higher effective orifice area at 30 days.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Aortic-valve stenosis--from patients at risk to severe valve obstruction N Engl J Med Otto CM Prendergast B 74475637120142514096010.1056/NEJ Mra 1313875 · doi ↗ · pubmed ↗
- 22025 ESC/EACTS Guidelines for the management of valvular heart disease: developed by the task force for the management of valvular heart disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS)Eur Heart J Praz F Borger MA Lanz J 0672025
- 3Five-year outcomes of transcatheter or surgical aortic-valve replacement N Engl J Med Makkar RR Thourani VH Mack MJ 79980938220203199568210.1056/NEJ Moa 1910555 · doi ↗ · pubmed ↗
- 4Transcatheter or surgical treatment of aortic-valve stenosis N Engl J Med Blankenberg S Seiffert M Vonthein R 1572158339020243858802510.1056/NEJ Moa 2400685 · doi ↗ · pubmed ↗
- 5Transcatheter or surgical aortic-valve replacement in intermediate-risk patients N Engl J Med Leon MB Smith CR Mack MJ 1609162037420162704032410.1056/NEJ Moa 1514616 · doi ↗ · pubmed ↗
- 6Transcatheter aortic-valve replacement with a balloon-expandable valve in low-risk patients N Engl J Med Mack MJ Leon MB Thourani VH 16951705380201910.1056/NEJ Moa 181405230883058 · doi ↗ · pubmed ↗
- 7Myval: a novel transcatheter heart valve for the treatment of severe aortic stenosis Interv Cardiol Seth A Kumar V Singh VP Kumar D Varma P Rastogi V 018202310.15420/icr.2020.32PMC 1031140137398875 · doi ↗ · pubmed ↗
- 8Valve Academic Research Consortium 3: updated endpoint definitions for aortic valve clinical research J Am Coll Cardiol 9 2025 Généreux P Piazza N Alu MC 2717274677202110.1016/j.jacc.2021.02.03833888385 · doi ↗ · pubmed ↗