The Cardio-Biliary Reflex in Gallbladder Disease: A Case Report and Literature Review
Rafat Shehata, Amr Anos, Mohammed Fathy Kandil Mohammed, Mostafa Hekal, Mohamed Elatiky

TL;DR
A case report shows how gallbladder issues can cause heart rhythm changes, highlighting the importance of recognizing this connection in diagnosis.
Contribution
This case report adds to the understanding of the cardio-biliary reflex in gallbladder disease and its clinical implications.
Findings
Biliary colic can induce significant cardiac rhythm changes via the cardio-biliary reflex.
Pain management alone can resolve bradycardia linked to gallbladder pathology.
Clinicians should consider the cardio-biliary reflex in diagnosing bradyarrhythmia with abdominal pain.
Abstract
This case report describes an elderly female presenting with simultaneous biliary colic and symptomatic sinus bradycardia. The resolution of her bradycardia with pain management alone suggested Cope’s sign, or the cardio-biliary reflex (CBR), as the underlying cause. This reflex is a well-recognized physiological response in which gallbladder pathology triggers vagal nerve signals, potentially causing significant alterations in cardiac rhythm and often mimicking primary heart conditions. This case illustrates that even uncomplicated biliary colic can induce this effect and emphasizes the importance for clinicians to consider this reflex in the differential diagnosis of bradyarrhythmia accompanied by abdominal pain. Recognizing CBR is crucial for directing management toward the correct biliary pathology and avoiding unnecessary cardiac investigations or interventions.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
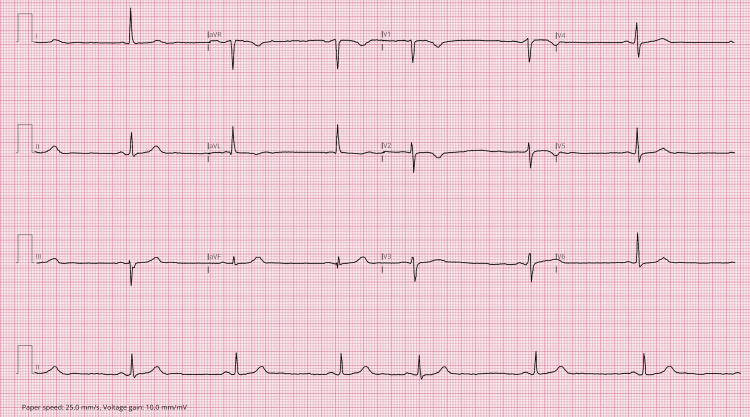 Figure 1
Figure 1| Test | Result | Reference range |
| Serum amylase | ||
| Amylase | 2955 | 28-100 U/L |
| C-reactive protein | 4 | 0-5 mg/L |
| Full blood count | ||
| Hemoglobin | 145 | 120-160 g/L |
| Leucocytes | 10 | 4-11 × 10⁹/L |
| Platelets | 256 | 150-450 × 10⁹/L |
| Red blood cell count | 4.44 | 3.8-5.8 × 10¹²/L |
| Hematocrit | 0.41 | 0.36-0.47 L/L |
| Neutrophils | 8.9 | 1.5-8 × 10⁹/L |
| Lymphocytes | 0.8 | 1.3-4 × 10⁹/L |
| Monocytes | 0.3 | 0.2-1 × 10⁹/L |
| Eosinophils | 0 | 0-0.8 × 10⁹/L |
| Basophils | 0 | 0-0.3 × 10⁹/L |
| Liver function tests | ||
| Bilirubin | 20 | 0-21 µmol/L |
| Alanine aminotransferase | 73 | 0-35 U/L |
| Aspartate aminotransferase | 101 | 0-34 U/L |
| Alkaline phosphatase | 106 | 30-130 U/L |
| Albumin | 41 | 34-50 g/L |
| Urea and electrolytes | ||
| Sodium | 141 | 133-146 mmol/L |
| Potassium | 3.8 | 3.5-5.3 mmol/L |
| Urea | 6.2 | 2.5-7.8 mmol/L |
| Creatinine | 71 | 45-84 µmol/L |
| Estimated glomerular filtration rate | 72 | 60-150 mL/min |
| Calcium | 2.5 | 2.15-2.6 mmol/L |
| Corrected calcium | 2.49 | 2.15-2.62 mmol/L |
| Thyroid function tests | ||
| Thyroid-stimulating hormone | 2.12 | 0.27-4.2 mU/L |
| Other biochemistry | ||
| Triglyceride | 0.89 | 0-1.7 mmol/L |
| Lactate dehydrogenase | 295 | 135-214 U/L |
| Study | Cases | GB presentation | Cardiac presentation | ECG changes | Complete resolution | Vagolytic | Temporary PM | PPM |
|
O’Reilly and Krauthamer (1971) [ | 2 | Acute calculous cholecystitis | Chest pain in Case 1 | SB | Cholecystectomy | Atropine in Case 1 | No | No |
|
Iftikhar et al. (2022) [ | 1 | Acute calculous cholecystitis | Asymptomatic | SB | Conservative Rx | Not reported | No | No |
|
Mainali et al. (2022) [ | 1 | Acute calculous cholecystitis | Lightheadedness | SB | Cholecystectomy | Atropine | No | No |
|
Kumar et al. (2020) [ | 1 | Acute calculous cholecystitis | Symptomatic bradycardia | Bradycardia with pauses | Analgesia and ABX | No | Yes | No |
|
Franzen et al. (2009) [ | 1 | Acute cholecystitis | Syncope | Complete AV block | Cholecystectomy | Not reported | No | No |
|
Meyer et al. (2024) [ | 1 | Acute cholecystitis | Chest pain | Inferolateral STE | Cholecystectomy | No | No | No |
|
Patel et al. (2011) [ | 1 | Acute calculous cholecystitis | Chest pain | SB + STE | Cholecystectomy | No | No | No |
|
Ola et al. (2020) [ | 1 | Acute calculous cholecystitis | Syncope | Complete AV block | Cholecystectomy | No | Yes | No |
|
Lau et al. (2015) [ | 1 | Acute acalculous cholecystitis | Not reported | SB/pause | Cholecystectomy | Not reported | No | No |
|
Papakonstantinou et al. (2018) [ | 1 | Biliary colic | Asymptomatic | SB + 7 S CHB | Analgesia | No | No | No |
|
Scott et al. (2021) [ | 1 | GB torsion | Chest pain & syncope | Bradycardia, No ECG | No | Not reported | No | No |
|
Soric et al. (2015) [ | 1 | Acute calculous cholecystitis | Asymptomatic | Intermittent CHB | Cholecystectomy | No | Yes | No |
|
Daliparty et al. (2021) [ | 1 | Calculous cholecystitis | Chest pain | Mobitz I AV block | Cholecystectomy | No | No | No |
|
Fang et al. (2021) [ | 1 | Cholecystitis and cholangitis | Dyspnea | Complete AV block | Delayed | No | Yes | Yes |
|
Furuhashi et al. (2003) [ | 1 | Acute cholecystitis | ECG changes | RBBB + STE | Cholecystectomy | No | No | No |
|
Ozeki et al. (2015) [ | 16 | Acute cholecystitis | Chest pain in four cases | Three ST-T ischemic changes | Three surgeries/drains and one ABX | Not reported | No | No |
|
Drachman et al. (2017) [ | 1 | Acute cholecystitis | Chest pain | Infero-antero-lateral STE | Surgical drain | No | No | No |
|
Patell et al. (2021) [ | 1 | Acute cholecystitis | Chest pain and diaphoresis | SB | Cholecystectomy | Not reported | No | No |
|
Vloka et al. (1999) [ | 2 | Gangrenous GB | Syncope in one case | SB | Cholecystectomy | Not clear | Yes | No |
|
Akyel et al. (2011) [ | 1 | Acute calculous cholecystitis | Asymptomatic | Idioventricular rhythm | Conservative | No | No | No |
| Our case | 1 | Biliary colic and cholelithiasis | Dizziness | SB | Analgesia | No | No | No |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac pacing and defibrillation studies · Cardiac Arrhythmias and Treatments · Cardiovascular Syncope and Autonomic Disorders
Introduction
The clinical presentation of acute gallbladder disease, including biliary colic, cholecystitis, and cholelithiasis, typically comprises right upper quadrant pain, fever, nausea, and vomiting. The cardio-biliary reflex (CBR) represents a well-documented yet underrecognized manifestation of acute gallbladder disease, presenting with profound cardiovascular symptoms [1,2]. First described in the early 20th century, this reflex is triggered by afferent stimuli from an inflamed or distended biliary tract, leading to an efferent parasympathetic surge via the vagus nerve [3]. The resulting clinical manifestations include significant bradyarrhythmias, hypotension, syncope, and ECG changes [4,5]. These symptoms often mimic primary cardiac diseases, creating diagnostic challenges and frequently prompting extensive, and sometimes unnecessary, cardiac investigations while the underlying biliary pathology remains undiagnosed [6].
Although most commonly reported in the context of acute cholecystitis, CBR can also be triggered by uncomplicated biliary colic. This scenario is less emphasized in the literature, contributing to its underrecognition in clinical practice [7,8]. Herein, we present an illustrative case of symptomatic sinus bradycardia secondary to uncomplicated biliary colic, which resolved completely with analgesia and conservative management. Through this case and a contemporary review of the literature, we aim to clarify the pathophysiology, expand the clinical spectrum beyond cholecystitis, and reinforce the management principles of this intriguing reflex. We highlight the critical importance of considering CBR in the differential diagnosis of any patient presenting with unexplained bradyarrhythmia concurrent with abdominal pain.
Case presentation
A 75-year-old woman presented to our hospital with acute epigastric pain radiating to the right upper quadrant, which had begun 24 hours prior to admission. The pain was persistent and unrelieved by paracetamol. She subsequently developed nausea and dizziness.
On initial assessment, she was noted to have bradycardia at 40 beats per minute; the remainder of her vital signs were unremarkable. Abdominal examination revealed a soft abdomen with localized tenderness in the right upper quadrant and epigastrium. There were no signs of peritoneal irritation, and Murphy’s sign was negative. Chest and cardiovascular examinations were normal.
Her medical history was significant for hypercholesterolemia, known cholelithiasis, and elevated body mass index. She had no history of thyroid disease and was not taking any rate-controlling medications.
Initial laboratory investigations revealed normal inflammatory markers, markedly elevated serum amylase, and deranged liver function tests (Table 1). Thyroid function tests were within normal limits. Electrocardiography confirmed sinus bradycardia at 41 beats per minute, with an atrial ectopic beat (Figure 1).
ECG showing sinus bradycardia at 41 bpm with an atrial ectopic beat
Thirty minutes after administration of analgesia, her heart rate improved, and her associated dizziness resolved completely. Abdominal ultrasound revealed a solitary gallstone with no evidence of cholecystitis. A magnetic resonance cholangiopancreatography was initially planned to further evaluate the biliary tree; however, the scan was aborted due to patient claustrophobia.
She was subsequently admitted under the surgical team and managed conservatively with analgesia and intravenous fluids. She was later discharged with a plan for elective laparoscopic cholecystectomy, which was performed successfully several weeks later without immediate postoperative complications or recurrence of bradycardia.
Discussion
Definition and nomenclature
The term “Cope’s sign” originates from Sir Zachary Cope, who in 1970 described his personal experience with gallbladder disease, initially mistaking the associated epigastric pain and symptoms for cardiac ischemia [1]. Shortly thereafter, O’Reilly and Krauthamer formally reported the association between reflex bradycardia and acute cholecystitis in two patients, coining the term “Cope’s sign” in the medical literature [2]. It is important to distinguish this from the other “Cope’s sign” (psoas test) used in diagnosing appendicitis [5]. The phenomenon is more accurately described as the CBR, a vagally mediated neural arc capable of inducing a spectrum of cardiac disturbances in response to biliary tract pathology [3,6,7].
Pathophysiological mechanism
The accepted mechanism of CBR involves a neural reflex arc. Afferent signals arise from mechanoreceptors and chemoreceptors in the gallbladder wall and biliary tract, stimulated by distension, inflammation, or calculi [8,9]. These impulses ascend via the vagus nerve to the nucleus tractus solitarius in the medulla oblongata, which then sends efferent signals back through vagal cardiac branches, increasing parasympathetic tone. This results in negative chronotropy (bradycardia), dromotropy (atrioventricular conduction delays or blocks), and vasodilation (hypotension) [10,11].
Additionally, the heart and gallbladder share autonomic innervation from spinal levels T4-T6, with intermediate neurons connecting these pathways, facilitating this cross-talk [12]. Animal studies have also demonstrated that gallbladder distension can trigger reflex coronary vasoconstriction, potentially explaining ST-segment changes observed in some cases [9,13,14].
Gallbladder diseases triggering the reflex
CBR is most commonly reported in acute calculous cholecystitis, as documented in numerous case reports [2,4,15]. However, it has also been described in acalculous cholecystitis [16], biliary colic without overt inflammation (as in our case) [17], and even rare entities such as gallbladder torsion [18]. Furthermore, iatrogenic triggers, such as intraoperative gallbladder manipulation, can initiate the reflex arc [19], suggesting that neural irritation, rather than inflammation alone, is the primary stimulus.
Cardiac presentations and ECG changes
The cardiac manifestations of CBR are diverse (Table 2). Sinus bradycardia is the most common presentation, but more severe arrhythmias have been reported, including various degrees of atrioventricular block, from first-degree to complete heart block [6,7,15,17,20-22], as well as sinus pauses or arrest [6,16]. Beyond arrhythmias, chest pain and ECG changes can mimic acute coronary syndrome (ACS), including ST-segment deviations and T-wave inversions, particularly in the inferior leads [13,23-25]. Our patient’s presentation with significant sinus bradycardia falls squarely within this recognized spectrum of rhythm disturbances.
Assessment and workup
Diagnosing CBR requires exclusion of primary cardiac causes. Serial ECGs typically do not show dynamic changes consistent with ischemia, and high-sensitivity troponin levels are usually normal, helping distinguish CBR from myocardial infarction [3,4,25]. Echocardiography is essential for assessing cardiac structure and function, particularly to rule out wall motion abnormalities suggestive of ACS. Ambulatory monitoring may be needed to capture hemodynamically significant bradyarrhythmias, guiding the decision for temporary interventions such as atropine or temporary pacing.
Ultrasonography remains the cornerstone imaging modality for identifying cholelithiasis, gallbladder wall thickening, pericholecystic fluid, and sonographic Murphy’s sign. The most critical diagnostic clue is the temporal association between biliary pain or manipulation and the onset of cardiac symptoms, along with symptom resolution following treatment of the biliary disease [2,6,26].
Management and resolution
Management of CBR involves both acute arrhythmia control and definitive treatment of the underlying biliary pathology. Symptomatic bradycardia can be rapidly reversed with vagolytic agents such as atropine, which may serve both diagnostic and therapeutic purposes [2,4,10]. Analgesia is crucial to remove the nociceptive stimulus triggering the reflex, and in some cases, as demonstrated in our patient, it may be sufficient to reverse bradycardia [6,17]. Emerging evidence suggests that esketamine, an N-methyl-D-aspartate receptor antagonist, may suppress the vagal reflex arc when administered preemptively during surgery, thereby reducing the incidence of CBR [19]. Temporary pacing is indicated for persistent bradyarrhythmia with hemodynamic compromise, providing circulatory support until the reflex abates [6,15,20,22,27,28]. Definitive resolution requires removal of the stimulus, with cholecystectomy being curative; arrhythmias typically resolve postoperatively. As illustrated in our case, conservative management with analgesia and antibiotics can resolve the reflex by reducing inflammation and distension, but surgery remains the definitive preventive measure for recurrence. Permanent pacemakers are rarely required and should only be considered if intrinsic, irreversible sinus node, or atrioventricular node dysfunction persists after treatment of the biliary pathology [22,29].
Conclusions
This case illustrates a classic presentation of CBR, in which acute gallbladder disease manifested with significant sinus bradycardia that resolved with conservative management. Although rare, CBR is clinically important and can mimic primary cardiac conditions. A high index of suspicion is essential to avoid misdiagnosis and unnecessary cardiac interventions. The cornerstone of management involves recognizing the connection between biliary pathology and cardiac manifestations, providing immediate symptomatic support with analgesics, vagolytic agents, or pacing if needed, and pursuing definitive treatment of the underlying biliary disease. This report reinforces the importance of a holistic diagnostic approach in patients presenting with abdominal pain and concomitant bradyarrhythmia.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1A sign of gall-bladder disease Br Med J Cope Z 14714831970543108610.1136/bmj.3.5715.147PMC 1702308 · doi ↗ · pubmed ↗
- 2"Cope's sign" and reflex bradycardia in two patients with cholecystitis Br Med J O'Reilly MV Krauthamer MJ 14621971558149410.1136/bmj.2.5754.146PMC 1795584 · doi ↗ · pubmed ↗
- 3Acute calculous cholecystitis with sinus bradycardia: Cope's sign encountered Cureus Iftikhar H Khan FS Al-Marri ND Zaki HA Masood M 014202210.7759/cureus.21187 PMC 883783035165631 · doi ↗ · pubmed ↗
- 4Symptomatic sinus bradycardia in a patient with acute calculous cholecystitis due to the cardio-biliary reflex (Cope’s sign): a case report Cureus Mainali A Adhikari S Chowdhury T Shankar M Gousy N Dufresne A 014202210.7759/cureus.25585 PMC 924905735785008 · doi ↗ · pubmed ↗
- 5Clarifying misconceptions about Cope's sign J Family Med Prim Care Yale SH Tekiner H 337833791120223611918810.4103/jfmpc.jfmpc_83_21PMC 9480782 · doi ↗ · pubmed ↗
- 6Cope’s sign and complete heart block secondary to acute cholecystitis: a case report J Acute Dis Kumar N Kumar P Dubey PK Kumar A Kumar A 17617892020
- 7Complete atrioventricular block in a patient with acute cholecystitis: a case of cardio-biliary reflex?Eur J Emerg Med Franzen D Jung S Fatio R Brunckhorst CB 34634716200910.1097/MEJ.0b 013e 32832 baed 819904083 · doi ↗ · pubmed ↗
- 8Electrocardiographic changes in cardiac patients with acute gallbladder disease Ann Surg Krasna MJ Flancbaum L 541543521986 https://pubmed.ncbi.nlm.nih.gov/3767139/3767139 · pubmed ↗