Facial Burn Healing With a Polylactic Acid Dermal Matrix: A Case Report on Wound Modulation and Graft-Free Epithelialization
Mario Aurelio Martínez-Jiménez, Ana Lorena Novoa-Moreno, Rodolfo Ariel Miranda-Altamirano, Olga Johnson-Ponce, Eleazar Samuel Kolosovas-Manchuca, Victor Manuel Loza-González

TL;DR
A new synthetic material helped heal a deep facial burn without needing a skin graft, showing promise for future burn treatments.
Contribution
This is the first reported use of a polylactic acid dermal matrix for deep facial burns without grafting.
Findings
The PLA matrix provided rapid pain relief and early vascularization in a facial burn case.
Full epithelialization occurred within 5 weeks without the need for skin grafting.
Histology and thermography showed improved healing and perfusion with the matrix.
Abstract
Due to their functional and aesthetic implications, facial burns pose significant clinical challenges. Alkali burns can further complicate these injuries by causing deep tissue necrosis, which complicates healing and increases the risk of scarring. Traditional management involves early excision and autografting, but challenges such as donor site morbidity and poor aesthetic integration remain. SUPRA SDRM, a fully synthetic, polylactic acid (PLA)-based resorbable dermal matrix, has demonstrated efficacy in different wound types but has not been previously reported in deep burn management. Here, we present the case of a 53-year-old male with deep alkali facial burns managed with SUPRA SDRM. Initially applied as a bridge to grafting, rapid pain relief, and early vascularization led to an alternative treatment course. The matrix formed an adherent synthetic wound barrier, modulating the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1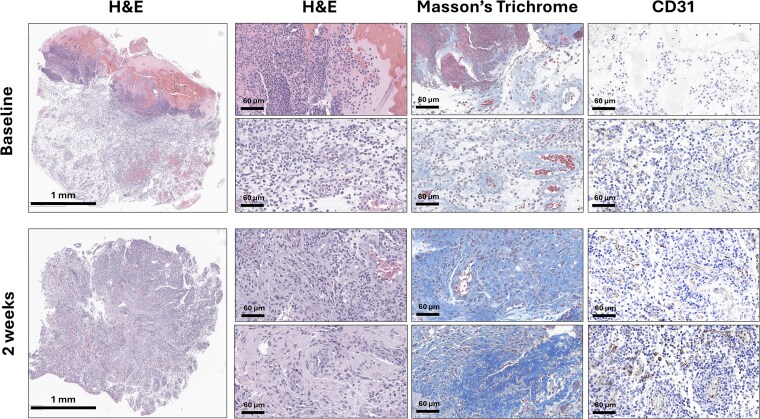 Figure 2
Figure 2 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsWound Healing and Treatments · Dermatologic Treatments and Research · Corneal Surgery and Treatments
INTRODUCTION
Facial burns present a unique clinical challenge due to their functional, aesthetic, and psychological consequences. These injuries can cause contractures and disfigurement that impair essential functions such as vision, speech, mastication, facial expression, and communication; factors that significantly impact quality of life and are major sources of distress among survivors.1 Although the rich vascularity of facial tissue supports rapid healing, it also predisposes patients to excessive inflammation, hypertrophic scarring, and pigmentation abnormalities. Thus, minimizing disfigurement and preserving function are key goals in facial burn management.2
Injuries caused by alkalis are particularly severe, as they induce liquefaction necrosis with deep tissue penetration and ongoing cellular damage, often resulting in more extensive injury than other burn types. Alarmingly, alkalis have recently emerged as agents of assault, increasing the prevalence of these burns in facial trauma.3 Standard treatment for deep facial burns includes early excision and autografting to reduce infection risk, scarring, and delayed healing. However, it poses challenges such as donor site morbidity, color mismatch, and visible textural differences.4 Skin substitutes have shown promise in enhancing wound healing, scar quality, and patient comfort, although they may slightly delay early re-epithelialization.5
Here, we present the case of a patient with a full-thickness alkali facial burn treated with SUPRA SDRM, a synthetic, biodegradable polylactic acid (PLA) matrix (Polymedics Innovations, Kirchheim unter Teck, Germany),6 to optimize wound bed preparation. Following the patient’s refusal of autografting, reapplication of the PLA matrix resulted in complete wound closure without the need for grafting.
CASE PRESENTATION AND RESULTS
A 53-year-old man experiencing homelessness presented to our burn unit 48 h after an alkali-based chemical assault to the face. He received initial decontamination at a community hospital before transfer for specialized care. On admission, he was hemodynamically stable but reported severe pain (9/10). Examination revealed complete epidermal and dermal loss, sparing the eyes but involving the right upper eyelid; the left eye had a prior enucleation (Figure 1).
Clinical Progression of a Facial Chemical Burn Following Treatment• Top Row (Left to Right): Initial Appearance Immediately After Surgical Debridement, Followed by Application of a Polylactic Acid Matrix on the Same Day. Then, Wound Progression at 1 and 2 Weeks Postapplication• Middle Row (Left to Right): Continued Healing at 3 Weeks and 4 Weeks, With the Latter Demonstrating Full Wound Closure. Next, Follow-Up Images at 6 and 12 Months, Highlighting Long-Term Outcomes• Bottom Row (Left to Right): Lateral View of the Wound, Beginning With the Initial Presentation, Progression at 4 Weeks, and Concluding With 6- and 12-Month Follow-Up Images
Tangential excision using the Versajet hydrosurgery system was performed for wound bed optimization. Histology confirmed mixed partial and full-thickness burns with necrosis, edema, and vascular injury (Figure 2). Digital planimetry (Swift Medical, Toronto, Canada) measured the burnt area at 38.5 cm^2^, affecting functionally and cosmetically critical facial regions. Infrared thermography (IRT) scan using a FLIR T600 camera (Teledyne FLIR, Wilsonville, OR) showed ΔT > −3.5°C compared to adjacent skin, indicating poor healing potential and supporting histopathologic findings (Figure 3).7–9
Left Eyebrow Biopsies Taken at Baseline (Pretreatment) and 2 Weeks Posttreatment Low-Magnification Views of 3 mm Punch Biopsies Stained With Hematoxylin and Eosin (H&E), Massons’s Trichrome, and CD31 for Endothelium Confirm a Full-Thickness Alkali Burn Characterized by Extensive Liquefaction Necrosis, Dense Inflammatory Infiltrates, Disrupted Collagen Architecture, and Capillary Microthrombosis With Endothelial Wall DestructionTwo Weeks Posttreatment; H&E Staining Reveals Reduced Inflammatory Infiltrates, on Masson’s Trichrome Staining Abundant Extracellular Matrix Deposition, With Randomly Oriented Collagen Fibrils, Indicative of Early Neo-dermis Formation. CD31 Staining Highlights a Robust Neo-angiogenic Response.
Infrared Thermographic AssessmentAt Baseline, Thermography Shows Hypothermic Regions (ΔT < −3.5°C) in Burned Areas. By 2 Weeks, ΔT Narrows to ≈ −2°C With Emerging Hotspots at Wound Margins, Suggesting Improved Vascularization and Active Epithelialization. At 3 Weeks, Thermal Asymmetry Continues to Decrease. By Week 5, Thermograms Resemble Uninjured Skin, No Hotspots or Coldspots, Indicating Resolved Inflammation and Restored Microvascular Function.
SUPRA SDRM was applied intraoperatively to optimize the wound bed for autologous split-thickness skin grafting (STSG) at day 14 postinjury. Due to the strong integration of SDRM into the wound bed and the development of a dry, adherent protective layer, the matrix was left uncovered. Pain reduced rapidly to 2/10 within 24 h, allowing discontinuation of opioids.
At 2 weeks, advancing epithelial margins and complete epithelialization of the right upper eyelid without contracture were observed. Infrared thermography imaging showed reduced ΔT values, and histopathological analysis revealed new collagen deposition, reduced inflammatory infiltrate with macrophage predominance, and increased angiogenesis evidenced by CD31-positive endothelial cells forming capillary structures (Figure 2). Despite a scheduled STSG, the patient declined further surgery due to minimal symptoms. Instead, a second SDRM application was performed at bedside.
By week 3, 50% of the wound was epithelialized, with the PLA matrix detaching from the fully healed areas and a third SDRM application was performed. By week 4, 80% of the burn was re-epithelialized, prompting discharge into the general ward. On the fifth and final week, a complete epithelialization and temperature symmetry with the IRT, showed a complete healing10 (Figure 2). Due to these findings the patient was discharged from the hospital with instructions for outpatient follow-up.
At a 3-, 6-, and 12-month follow-up posttreatment, the patient showed stable healing with mild hypopigmentation, preserved facial mobility, no inflammation, and no signs of contracture or hypertrophic scarring (Figure 1).
DISCUSSION
This case highlights the successful use of a PLA-based dermal matrix in managing a full-thickness chemical facial burn, achieving full healing without autografting, while also providing effective pain relief and reducing inflammation. The decision to use SUPRA SDRM was based on prior studies demonstrating favorable outcomes with PLA-based membranes.6^,^11^,^12
The clinical efficacy observed can be attributed to the matrix’s dual role as a physical scaffold and a bioactive modulator. It integrated into the wound bed, forming a synthetic barrier that retained moisture, reduced contraction, and protected exposed nerve endings. Concurrently, lactate released from the matrix lowered local pH, providing antimicrobial effects,13^,^14 and promoted wound healing through pro-angiogenic, anti-inflammatory, and ECM-stimulating pathways.15–17 Histopathologic findings at 2 weeks supported this hypothesis, showing neo-dermis–like structures, collagen deposition, reduced inflammation, and robust capillary formation, suggesting active participation of the matrix in tissue regeneration.
Another novel aspect of this case was the use of IRT as an objective assessment tool, enabling real-time evaluation of tissue perfusion and healing progression.7^,^9^,^10
While the outcomes are promising, this report is inherently limited by its single-patient design. Further studies are needed to evaluate reproducibility, compare efficacy with conventional treatments and assess long-term durability of the regenerated tissue. Outcomes such as scar maturation and resilience to re-injury over time remain to be fully understood. Nonetheless, based on serial follow-up, the regenerative effects appear sustained.
CONCLUSION
This case highlights the potential of alloplastic skin substitutes to shift the paradigm in burn care by offering a non-invasive alternative to traditional multi-stage reconstruction. The successful use of a fully synthetic dermal matrix to achieve deep burn healing without grafting opens new possibilities for resource-limited settings, mass casualty incidents, or when surgical options are declined, balancing effective healing with minimal intervention. Looking ahead, integrating bio-inductive materials, real-time perfusion tools, and patient-centered models may help redefine standards in burn and complex wound care.
Patient gave written consent of using his clinical case to be shown in this study.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Clark C, Ledrick D, Moore A. Facial burns. In:Stat Pearls [Internet]. Stat Pearls Publishing editors. Treasure Island (FL): Stat Pearls Publishing, 2025. Available from: http://www.ncbi.nlm.nih.gov/books/NBK 559290/.32644716 · pubmed ↗
- 2Greenhalgh DG . Management of facial burns. Burns Trauma. 2020;8:tkaa 023.10.1093/burnst/tkaa 023PMC 733618332665953 · doi ↗ · pubmed ↗
- 3Van Hoy TB, Metheny H, Patel BC. Chemical burns. In:Stat Pearls [Internet]. Stat Pearls Publishing editors. Treasure Island (FL): Stat Pearls Publishing, 2025 Accessed February 4, 2025. Available from: http://www.ncbi.nlm.nih.gov/books/NBK 499888/29763063 · pubmed ↗
- 4Abubakar ML, Ibrahim A. Management of facial burns: an update. Curr Opin Otolaryngol Head Neck Surg 2021;29:299–303.34183560 10.1097/MOO.0000000000000723 · doi ↗ · pubmed ↗
- 5Van den Bosch AS, Verwilligen RAF, Pijpe A et al. Outcomes of dermal substitutes in burns and burn scar reconstruction: a systematic review and meta-analysis. Wound Repair Regen 2024;32:960–978.39435560 10.1111/wrr.13226 PMC 11584356 · doi ↗ · pubmed ↗
- 6Barbachowska A, Korzeniowski T, Surowiecka A et al. Alloplastic epidermal skin substitute in the treatment of burns. Life (Basel) 2023;14:43.38255658 10.3390/life 14010043 PMC 10821452 · doi ↗ · pubmed ↗
- 7Martínez-Jiménez MA, Ramirez-Garcia Luna JL, Kolosovas-Machuca ES et al. Development and validation of an algorithm to predict the treatment modality of burn wounds using thermographic scans: prospective cohort study. P Lo S One 2018;13:e 0206477.30427892 10.1371/journal.pone.0206477 PMC 6235294 · doi ↗ · pubmed ↗
- 8Jaspers MEH, Maltha I, Klaessens JHGM et al. Insights into the use of thermography to assess burn wound healing potential: a reliable and valid technique when compared to laser Doppler imaging. J Biomed Opt 2016;21:96006.27623232 10.1117/1.JBO.21.9.096006 · doi ↗ · pubmed ↗