Dietary antioxidant intake in women with facial melasma: a case-control study
Ana Cláudia Cavalcante Espósito, Carla Rakoski Ribas, Gracielli Ferreira Barbosa, Julia Dias Bendini, Rita Gisele Biffi Medeiros, Carolina Nunhez da Silva, Tatiana Cristina Figueira, Hélio Amante Miot

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
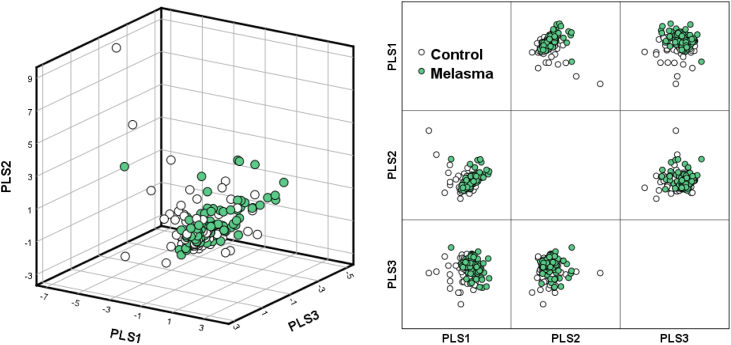 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDermatologic Treatments and Research · Acne and Rosacea Treatments and Effects · melanin and skin pigmentation
Dear Editor,
Melasma is a chronic, multifactorial pigmentary dermatosis that exclusively affects sun-exposed areas (with lesions predominantly on the face) and is more prevalent in women in the period between menarche and menopause. Genetic predisposition, exposure to ultraviolet radiation (UVR), and hormonal stimuli are its main triggers. However, other factors, such as exposure to environmental pollution, heat, sleep deprivation, and chronic conditions such as depression, can aggravate systemic oxidative stress, potentially contributing to the genesis and progression of melasma.1
Systemic oxidative stress is prominent in patients with melasma. Concurrently, the administration of oral antioxidants, such as pycnogenol, enhances the clearing effect of topical treatment.2
Chronic exposure to UVR, especially type A, induces both cell and systemic oxidative stress, contributing to the sustained melanogenesis observed in melasma.1 There is a negative correlation between the clinical severity of melasma and plasma glutathione (GSH) levels, as well as increased levels of components of the intracellular antioxidant defense enzyme system, such as superoxide dismutase (SOD) and GSH-peroxidase.3 Furthermore, individuals with melasma have higher plasma concentrations of malondialdehyde, a byproduct of lipid peroxidation that is a marker of cell damage.4
In the context of antioxidant defense mechanisms, in addition to the enzyme system (such as SOD and GSH-peroxidase), the importance of non-enzymatic antioxidants obtained through diet stands out. These include compounds present in foods rich in beta-carotene, vitamins C and E, ellagic acid, bioflavonoids, catechins, isoflavones, lycopene, omega-3 fatty acids, polyphenols, resveratrol, selenium, zinc, and cysteine.
To date, no study has systematically evaluated dietary aspects in individuals with melasma. To fill this gap, a cross-sectional study was conducted to investigate dietary patterns, with a specific focus on the intake of antioxidant-rich foods, in women with facial melasma compared to those without the condition.
After approval by the institutional ethics committee (CAAE 26390419.7.0000.5515), 194 adult women of childbearing age (aged 18 to 49) were included and divided into two groups: 97 with facial melasma (diagnosed by a dermatologist) and 97 controls. Participant recruitment occurred from September 2023 to January 2024. Matching was performed by age, and women with concomitant facial dermatoses were excluded. Sampling was consecutive, among patients treated at the Presidente Prudente Regional Hospital, and was conducted after informed consent was obtained.
The main study outcome measure was the adapted Food Frequency Questionnaire (FFQ), which was administered to participants to assess their weekly consumption of 41 types of foods (Supplementary Material). The data obtained were converted to grams, and from this, energy, macronutrient, and micronutrient values were calculated using the Nutritional Data System for Research (NDSR) software. Dietary patterns were analyzed based on their components, extracted using the PLS (Partial Least Squares) method, using data scaled by standard deviations.5 All dietary intake assessments were processed and analyzed by a nutritionist (TCF).
In addition, demographic data, adherence to photoprotection, smoking status, and oral antioxidant supplementation were collected. Nutrients were compared between groups using the Mann-Whitney (exact) test, with significance set at p ≤ 0.01. Sample size was calculated to detect a minimum difference of 20% in nutrient intake between groups, with an alpha of 0.01 and a beta of 0.1.
There were no differences between the groups in age, phototypes, age at menarche, smoking status, number of children, adherence to sunscreen, contraceptive use, or oral antioxidant supplementation (Table 1).Table 1. Main demographic data of women with melasma and controls.Table 1. VariablesMelasmaControlp-valuean9797‒Age (years) – mean (sd)38 (7)37 (9)0.162Phototype (Fitzpatrick) – n (%)0.035 I‒II37 (38)50 (52) III44 (45)39 (40) IV‒V16 (17)8 (8)Family member with melasma – n (%)58 (60)20 (21)<0.001Regular use of sunscreen – n (%)73 (75)63 (65)0.158Age at menarche (years) – mean (sd)12 (1)12 (1)0.916Time of melasma (years) – median (p25–p75)8 (5–15)‒‒Number of children – median (p25–p75)1 (0–2)1 (0–2)0.243Uses oral contraceptive– n (%)33 (34)39 (40)0.458Current smoker– n (%)9 (9)2 (2)0.058Use of oral antioxidant– n (%)18 (19)10 (10)0.152aBivariate analysis.
The diet in both groups was monotonous, and the most commonly consumed foods per week in both groups were milk, cheese, oranges, tomatoes, coffee, and white meat. No celiac disease or vegetarians were found in the sample. Extraction of three PLS components based on the dietary patterns formed by the 41 foods studied explained the variance of only 20% of the groups, without implying adequate separation between the melasma group and controls (Fig. 1). Furthermore, no differences were observed between the two groups regarding the consumption of macro and micronutrients, including dietary antioxidants (Table 2).Fig. 1. Dietary patterns of participants regarding the 41 foods investigated. Loading according to the three PLS (parcial least squares) components (n = 194).Fig. 1. Table 2Nutritional data of participants' diets, reported in one week (n = 194).Table 2. NutrientsMelasmaControlp-valueaMedianp25p75Medianp25p75Energy(kcal)18,16412,39625,83621,11013,30929,0830.208Protein (g)9206351,4181,2047151,8780.023Carbohydrate (g)2,3921,2923,6182,3321,3653,2240.608Lipids (g)4413286665983359520.021Saturated lipids (g)16371311223864070.053Monounsaturated Lipids (g)11661168173812820.024Polyunsaturated Lipids (g)533210061331240.258Cholesterol (mg)2,4271,5644,8153,2401,7997,1570.063Fiber (g)4382357453842517350.924Sodium (mg)13,8177,73630,34119,38311,86433,5220.039Calcium (mg)13,7447,57520,33814,3688,83223,6940.205Iron (mg)10763207133752170.213Zinc (mg)9563140124701560.055Vitamin A (mcg)11,6175,25923,80010,5424,81824,5180.967Vit. B1 (mg)2011282113340.273Vit. C (mg)4,5861,8959,7933,6781,5237,9170.220Vitamin E (mg)8245166105451820.467Vitamin B6 (mg)2920463421440.419Vitamin D (mg)23965349980.103Potassium (mg)52,57332,82677,67455,82835,77678,2890.675Magnesium (mg)4,7742,9877,3185,4913,1427,9810.257Selenium (mg)8785081,5701,0445682,2340.086Folate (mg)4,3882,0996,6653,8992,3236,1630.627aBivariate analysis.
Despite the oxidative microenvironment in the upper dermis, the causes of systemic oxidative imbalance in melasma patients are not understood, and the results of this study demonstrated no differences in dietary antioxidant consumption in these patients.
The eating habits of the urban Brazilian population are unbalanced, characterized by low food variability, high caloric intake of carbohydrates such as rice and pasta, and consumption of ultraprocessed foods, but low intake of fiber and micronutrients.6 The study participants did not exhibit eating habits that differed from those of the urban Brazilian population.
Research on dietary patterns and their association with health outcomes is important but has been little explored systematically in the dermatological literature. It is also important to highlight that understanding the nutritional components of a diet influences not only the body's nutritional aspects but also the composition of the intestinal microbiome, the effects of xenobiotics, and the overall epigenetic control exerted by certain foods.7
There are no robust studies in the literature that have investigated the increased consumption of antioxidant-rich foods in other dermatoses. Specifically in rosacea, studies with zinc supplementation have shown conflicting results and methodological limitations, resulting in insufficient evidence to recommend its clinical use. A review of the literature on dietary supplements showed that, in patients with vitiligo, only oral vitamin D replacement is recommended in cases of proven deficiency, although there is still no consensus on the ideal dose to promote repigmentation. The use of Polypodium leucotomos is also indicated, as long as it is combined with phototherapy, and shows evidence of increased repigmentation, especially in exposed areas. Supplementation with vitamins C and B12, vitamin E, antioxidant mixtures, and Ginkgo biloba still has insufficient evidence for routine recommendation.8
A Chinese study involving 150 cases and 150 controls identified alcohol intake as a risk factor (Odds Ratio = 20.5) and soft drink consumption as a protective factor (Odds Ratio = 0.04) for the development of melasma. However, these factors have not been adequately investigated from a pathophysiological perspective.9 And, despite being a common demand of patients, there are still no validated associations between dietary aspects and the onset of melasma. In this study, no differences in dietary patterns were identified when comparing women with melasma and the control group.
To date, evidence suggests oral supplementation with antioxidants (such as pycnogenol) as an adjunct to treatment.10 In the context of specific dietary intake, it is hypothesized that soy may exacerbate melasma due to its "estrogen-like" action; however, there is no data on a critical amount for this outcome.11
Studies related to dietary patterns have limitations related to participant recall, food recall, and the monotony of urban populations' diets. However, sample homogeneity, such as that of these participants from a single center, strengthens internal validity when exploring factors linked solely to diet. The lack of observational association does not mean that dietary interventions are ineffective; however, different study designs are required to confirm this. Finally, studies exploring the intestinal microbiome may suggest dietary interventions for melasma.
In conclusion, neither dietary patterns nor dietary antioxidant consumption is associated with the development of melasma in Brazilian women.
Authors' contributions
Ana Cláudia Cavalcante Espósito: Design and planning of the study; analysis and interpretation of data; drafting and editing of the manuscript; critical review of the literature; critical review of the manuscript; approval of the final version of the manuscript.
Carla Rakoski Ribas: Design and planning of the study; analysis and interpretation of data; drafting and editing of the manuscript; critical review of the literature; critical review of the manuscript; approval of the final version of the manuscript.
Gracielli Ferreira Barbosa: Design and planning of the study; analysis and interpretation of data; drafting and editing of the manuscript; critical review of the literature; critical review of the manuscript; approval of the final version of the manuscript.
Julia Dias Bendini: Design and planning of the study; analysis and interpretation of data; drafting and editing of the manuscript; critical review of the literature; critical review of the manuscript; approval of the final version of the manuscript.
Rita Gisele Biffi Medeiros: Design and planning of the study; analysis and interpretation of data; drafting and editing of the manuscript; critical review of the literature; critical review of the manuscript; approval of the final version of the manuscript.
Carolina Nunhez da Silva: Design and planning of the study; analysis and interpretation of data; drafting and editing of the manuscript; critical review of the literature; critical review of the manuscript; approval of the final version of the manuscript.
Tatiana Cristina Figueira: Analysis and interpretation of data; drafting and editing of the manuscript; collection of data; approval of the final version of the manuscript.
Hélio Amante Miot: Design and planning of the study; analysis and interpretation of data; statistical analysis; drafting and editing of the manuscript; critical review of the literature; critical review of the manuscript; approval of the final version of the manuscript.
Approval by the Ethics Committee
This project was approved by the Ethics Committee of Universidade do Oeste Paulista CAAE: 26390419.7.0000.5515 (UNOESTE).
Financial support
None declared.
Availability of research data
The entire dataset supporting the results of this study was published in this article.
Conflicts of interest
None declared.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Espósito A.C.C.Cassiano D.P.da Silva C.N.Lima P.B.Dias J.A.F.Hassun K.Update on melasma-part I: pathogenesis Dermatol Ther 1220221967198810.1007/s 13555-022-00779-x PMC 946427835904706 · doi ↗ · pubmed ↗
- 2Lima P.B.Dias J.A.F.Esposito A.C.C.Miot L.D.B.Miot H.A.French maritime pine bark extract (pycnogenol) in association with triple combination cream for the treatment of facial melasma in women: a double-blind, randomized, placebo-controlled trial J Eur Acad Dermatol Venereol 3520215025083284143310.1111/jdv.16896 · doi ↗ · pubmed ↗
- 3Wiraguna A.A.G.P.Hari E.D.Praharsini I.G.A.A.Correlation between glutathione plasma with degree severity of melasma in balinese women Clin Cosmet Investig Dermatol 13202045545910.2147/CCID.S 258834 PMC 736792032765038 · doi ↗ · pubmed ↗
- 4Choubey V.Sarkar R.Garg V.Kaushik S.Ghunawat S.Sonthalia S.Role of oxidative stress in melasma: a prospective study on serum and blood markers of oxidative stress in melasma patients Int J Dermatol 5620179399432868138210.1111/ijd.13695 · doi ↗ · pubmed ↗
- 5Yang T.C.Aucott L.S.Duthie G.G.Macdonald H.M.An application of partial least squares for identifying dietary patterns in bone health Arch Osteoporos 1220176310.1007/s 11657-017-0355-y PMC 550650828702941 · doi ↗ · pubmed ↗
- 6Mendonça R.D.Lopes M.S.Freitas P.P.Campos S.F.de Menezes M.C.Lopes A.C.S.Monotony in the consumption of fruits and vegetables and food environment characteristics Rev Saude Publica 532019633148300510.11606/S 1518-8787.2019053000705 PMC 6707622 · doi ↗ · pubmed ↗
- 7Lindell A.E.Zimmermann-Kogadeeva M.Patil K.R.Multimodal interactions of drugs, natural compounds and pollutants with the gut microbiota Nat Rev Microbiol 2020224314433510230810.1038/s 41579-022-00681-5PMC 7615390 · doi ↗ · pubmed ↗
- 8Jamgochian M.Alamgir M.Rao B.Diet in dermatology: review of diet’s influence on the conditions of rosacea, hidradenitis suppurativa, herpes labialis, and vitiligo Am J Lifestyle Med 1720231521603663638910.1177/15598276211026592 PMC 9830249 · doi ↗ · pubmed ↗