Overlooked and Underdiagnosed: Cardiac Sarcoidosis and Unexplained Ventricular Tachycardia and Fibrillation
Aaron A. Sifuentes, Ghazaleh Goldar, Usamah M. ElBakkush, Kaushik Gokul, Mohammed Mhanna, Peter Farjo, Paari Dominic

TL;DR
This study finds that cardiac sarcoidosis is underdiagnosed in patients with unexplained heart rhythm issues, despite existing guidelines for testing.
Contribution
The study quantifies the underutilization of guideline-based diagnostics for cardiac sarcoidosis in patients with unexplained VT/VF.
Findings
Only 1.4% of patients were diagnosed with sarcoidosis despite guidelines suggesting higher prevalence.
Cardiac MRI was performed in 19.9% of patients, while PET imaging was used in just 2.3%.
The low diagnostic rate suggests significant underdiagnosis of cardiac sarcoidosis.
Abstract
Cardiac sarcoidosis (CS) often manifests as unexplained ventricular tachycardia (VT) and ventricular fibrillation (VF) but remains significantly underdiagnosed. Although guidelines recommend advanced diagnostics, many clinicians may not pursue this in patients presenting with unexplained VT/VF. The objective of the study was to assess the proportion of patients with unexplained VT/VF who underwent guideline-based evaluation for CS. Using TriNetX data, we conducted a retrospective cohort study of patients aged 18 years or older who presented with unexplained VT/VF requiring implantable cardioverter defibrillator device implantation over the past 5 years. We evaluated the use of cardiac diagnostic modalities; including cardiac magnetic resonance imaging, positron emission tomography imaging, chest computed tomography, and myocardial biopsy, and monitored subsequent diagnoses of CS over…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
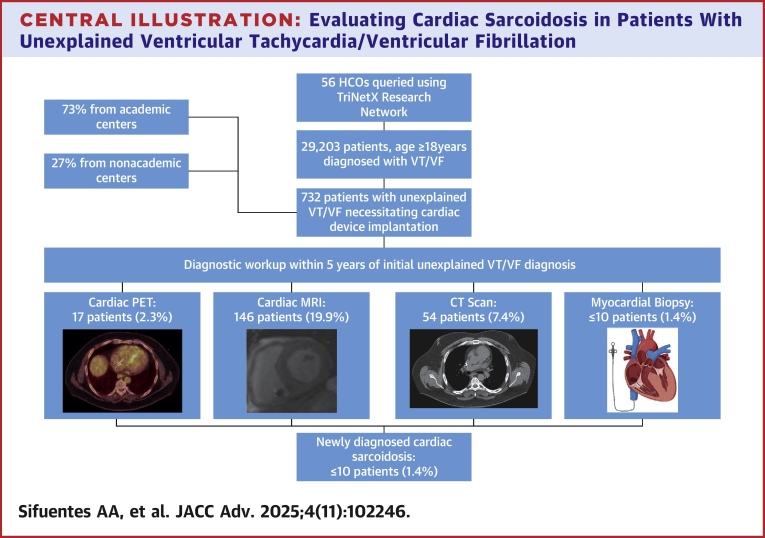 Figure 1
Figure 1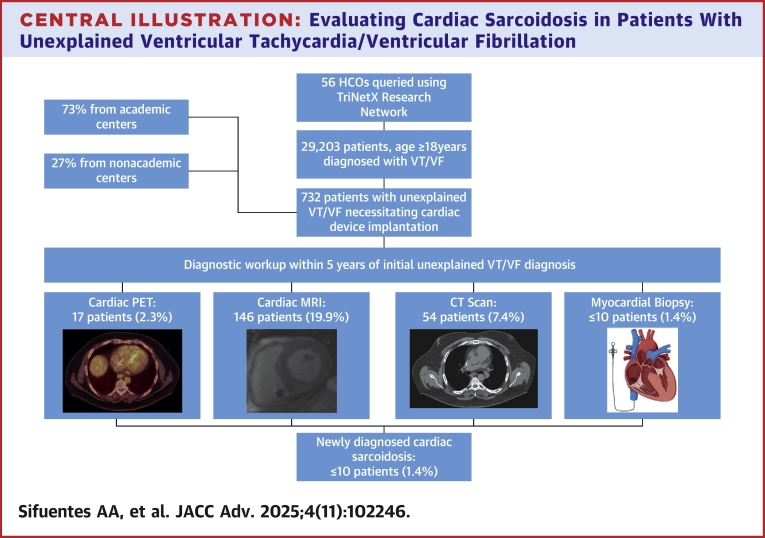 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFibromyalgia and Chronic Fatigue Syndrome Research · Vestibular and auditory disorders · Autoimmune Neurological Disorders and Treatments
Sarcoidosis is a multisystem granulomatous disorder that can lead to life-threatening conditions, including high-grade atrioventricular block, ventricular arrhythmias, and heart failure.1, 2, 3 Cardiac involvement, the leading cause of death related to sarcoidosis, is clinically apparent in only 5% of patients with sarcoidosis, although myocardial lesions are detected at autopsy in 20% to 60% of cases.4 Per prior reports approximately 17% to 28% of patients with unexplained ventricular tachycardia (VT) or ventricular fibrillation (VF) potentially have underlying cardiac sarcoidosis (CS), yet it is often missed in clinical practice.1^,^3^,^5
Diagnosing CS can be challenging due to nonspecific symptoms and overlap with other cardiac conditions, such as ischemic heart disease and myocarditis.1^,^2 Moreover, the standard diagnostic tools such as echocardiography are often insufficient to detect the subtle myocardial involvement seen in CS.2 Recent advancements in cardiac imaging, particularly cardiac magnetic resonance imaging (cMRI) and positron emission tomography (PET), have greatly improved the ability to detect CS in its early stages. Chest computed tomography (CT), although not part of the guideline recommended workup, can provide insight into potential extra-CS, especially at centers where more advanced imaging techniques are unavailable. Myocardial biopsy is the gold standard for confirming CS by visualizing noncaseating granulomas.1^,^2 However, this is often reserved for cases of inconclusive imaging, due to its invasiveness and associated risks.2 Even with biopsy, sensitivity is low at 20% due to the patchy nature of the disease and the potential sampling of unaffected areas. However, sensitivity can increase to 40% to 50% when guided by voltage mapping.2 The American Heart Association recommends considering CS in patients with unexplained VT/VF, particularly when other causes of VT/VF have been excluded.2 These guidelines emphasize the importance of immunosuppressive/antiarrhythmic therapy to prevent progression and cardiac complications.1, 2, 3 Treatment may enhance conduction in cases of atrioventricular block, but their effects on ventricular arrhythmias, left ventricular dysfunction, and mortality are not yet firmly established.2 Treatment of the latter 2 is inferred from smaller studies that show left ventricular dysfunction, and ventricular arrhythmias respond to treatment, but there is currently a lack of robust high-powered studies.2^,^3^,^6, 7, 8, 9 Although clear guidelines exist, a substantial disconnect is believed to persist between clinical recommendations and real-world practice. This study aims to assess the use of diagnostic testing for CS in unexplained VT/VF.
Methods
Study design
This study is a retrospective cohort analysis seeking to identify the number of patients presenting with unexplained VT/VF who received guideline-recommended workup of CS.
Data source
This study used data from the TriNetX Global Health Research Network (TriNetX, Inc), a federated health data platform that aggregates deidentified electronic health records from over 90 health care organizations (HCOs) across the world. The TriNetX platform provides access to data on patient demographics, diagnoses, procedures, medications, and outcomes, allowing for large-scale epidemiological analyses. As a federated network, TriNetX received a waiver from Western Institutional Review Board as only aggregated counts and statistical summaries of deidentified information are received, no protected health information is received, and no study-specific activities are performed in retrospective analyses. This query was run in May 2025 on the network research (with natural language processing) with data provided from 56 HCOs. The natural language processing functionality was available within the network but was not usede for patient selection or outcome assessment in this analysis. Our study relied exclusively on structured data derived from International Classification of Diseases, Tenth Revision (ICD-10) and Current Procedural Terminology (CPT) codes.
Patient selection
We used the ICD-10 diagnosis and procedure codes, and the Centers for Medicare and Medicaid CPT codes (Supplemental Table 1) to identify patients. This study included patients aged ≥18 years who were diagnosed with unexplained VT/VF necessitating placement of an implantable cardioverter defibrillator within 30 days, followed over a 5-year period (2020-2025). Unexplained VT/VF was defined as VT/VF without any known underlying cause. For the inclusion and exclusion criteria please see Table 1.Table 1. Inclusion and Exclusion CriteriaInclusion criteria Age ≥18 Diagnosis of VT or VF Implantable cardioverter-defibrillator device insertion within 30 days of being diagnosed with VT or VFExclusion criteria Previously diagnosed sarcoidosis or sarcoid myocarditis Acute myocardial infarction Ischemic heart diseases Cardiomyopathy (eg, dilated cardiomyopathy, hypertrophic cardiomyopathy, restrictive cardiomyopathy, substance induced cardiomyopathy) Long QT syndrome Other cardiac ion channelopathies (eg, Brugada syndrome, long QT syndrome, short QT syndrome catecholaminergic polymorphic ventricular tachycardia (CPVT)) Left ventricular ejection fraction ≤35% Prior diagnosis of amyloidosis Pre-excitation/accessory pathway syndromes Thyrotoxicosis (thyrotoxic crisis or storm) Infective myocarditisVF = ventricular fibrillation; VT = ventricular tachycardia.
Index event
In our study, the index event was defined as the date on which a patient was diagnosed with VT/VF.
Time window
Our analysis started on the first day of the index event and continued until 5 years after the first occurrence of the index event. Our cohort includes patients between the years 2020 and 2025.
Outcome
The primary outcome measure was the proportion of patients who underwent diagnostic testing for CS, including cMRI, PET scans, chest CT, and myocardial biopsy. The secondary outcome measure was the diagnosis of sarcoidosis during the follow-up period. Cardiac MRI, PET scan, chest CT, myocardial biopsy, and sarcoidosis diagnosis were identified using CPT codes shown in Supplemental Table 1.
Statistical analysis
Analyses were conducted using the TriNetX Analytics platform and no external statistical software was used. Continuous variables were summarized as mean ± SD or median with IQR, and categorical variables as counts and percentages. For proportions, 95% CIs were calculated using the Wilson score method, the default approach within TriNetX. Analyses were descriptive in nature; no propensity score matching or hypothesis testing was performed.
Results
TriNetX identified 732 patients diagnosed with VT/VF which met the inclusion and exclusion criteria across 56 HCOs. Among them, 534 patients (73%) were from academic centers (38 HCOs). Baseline clinical characteristics and geographical details of the cohort are summarized in Tables 2 and 3, respectively. The mean age of patients was 53 ± 19 years, with an age range of 18 to 90, 61% were male and 73% were White, whereas 8% were African American. Over a median follow-up of 827 days (IQR: 0-1,167 days), cMRI was performed in 146 patients (19.9%; 95% CI: 17.21%-22.99%), cardiac PET in 17 patients (2.3%; 95% CI: 1.45%-3.69%), chest CT in 54 patents (7.4%; 95% CI: 5.70%-9.50%), and myocardial biopsy in < 10 patients (1.4%; 95% CI: 0.74%-2.50%). Overall, only 26% of patients underwent advanced testing (MRI, PET, chest CT, or biopsy), with an ultimate CS diagnosis rate of ≤1.4% (95% CI: 0.74%-2.50%) (Table 4). Characteristics and geographical details specific to patients who underwent any of the diagnostic evaluations and those without any evaluation are detailed in Table 5. Study design and results are demonstrated in the Central Illustration.Table 2. Baseline Characteristics of the Cohort (N = 732)Age (y)53 ± 19Sex Male446 (61%) Female278 (38%)Ethnicity White534 (73%) Black58 (8%) Asian29 (4%) American Indian or Alaska10 (1.4%) Native Hawaiian or other Pacific Islander10 (1.4%) Other or unknown race95 (13%)Comorbid conditions SVT190 (26%) Essential (primary) hypertension322 (44%) Atrial fibrillation or flutter271 (37%) First degree atrioventricular block80 (11%) Advanced heart block124 (17%) Premature ventricular contractions248 (34%) Premature atrial contractions80 (11%) Left bundle branch block44 (6%) Right bundle branch block139 (19%) Sick sinus syndrome102 (14%) Type 2 diabetes mellitus95 (13%) Chronic kidney disease51 (7%)Values are mean ± SD or n (%).SVT = supraventricular tachycardia.Table 3. Geographic Distribution of Patients in the Cohort (N = 732)Northeast273 (37%)Midwest95 (13%)South229 (31%)West117 (16%)Unknown18 (2%)Values are n (%).Table 4. Summary of Prevalence of Outcomes (N = 732)cMRI146 (19.9%) [95% CI: 17.21–22.99]Cardiac PET17 (2.3%) [95% CI: 1.45–3.69]Myocardial biopsy≤10∗ (≤1.4%) [95% CI: 0.74–2.50]Patient with at least 1 of the following: cMRI, cardiac PET, myocardial biopsy158 (21.6%) [95% CI: 18.76–24.71]Chest CT54 (7.4%) [95% CI: 5.70–9.50]Any of: cMRI, cardiac PET, biopsy, or chest CT194 (26.5%∗) [95% CI: 23.43–29.82]Diagnosis of sarcoidosis≤10∗ (≤1.4%) [95% CI: 0.74–2.50]cMRI = cardiac magnetic resonance imaging; CT = computed tomography; PET = positron emission tomography.∗To protect patient privacy, numbers are rounded up to 10 in the TriNetX database.Table 5. Characteristics and Geographic Distribution of Patients Who Did Versus Did Not Undergo Any Diagnostic EvaluationPatients With at Least 1 Diagnostic Testing (n = 171)Patients Without Any Diagnostic Evaluation (n = 557)P ValueCharacteristics Age (years)51 ± 1853 ± 19<0.001 Sex Male111 (65%)334 (60%)0.284 Female56 (33%)212 (38%)0.242 Unknown4 (2%)11 (2%)1.000Ethnicity White126 (74%)401 (72%)0.738 Black17 (10%)45 (8%)0.544 Asian8 (5%)22 (4%)0.842 American Indian or Alaska0 (0%)11 (2%)0.135 Native Hawaiian or other Pacific Islander8 (5%)11 (2%)0.096 Other or unknown race10 (6%)67 (12%)0.031U.S. region Northeast61 (36%)200 (36%)0.895 Midwest31 (18%)73 (13%)0.129 South44 (26%)178 (32%)0.247 West25 (15%)95 (17%)0.787 Unknown10 (6%)11 (2%)0.017Comorbid conditions SVT51 (30%)134 (24%)0.157 Essential (primary) hypertension82 (48%)245 (44%)0.410 Atrial fibrillation or flutter60 (35%)212 (38%)0.540 First degree atrioventricular block22 (13%)61 (11%)0.581 Advanced heart block29 (17%)95 (17%)1.00 Premature ventricular contractions68 (40%)178 (32%)0.072 Premature atrial contractions22 (13%)58 (10%)0.449 Left bundle branch block8 (5%)33 (6%)0.668 Right bundle branch block39 (23%)106 (19%)0.331 Sick sinus syndrome18 (11%)83 (15%)0.186 Type 2 diabetes mellitus32 (19%)61 (11%)0.011 Chronic kidney disease12 (7%)39 (7%)1.000Abbreviations as in Table 2.
Discussion
Our findings indicate that only a small proportion of patients presenting with unexplained VT/VF underwent evaluation for CS, which is inconsistent with the major clinical guidelines.1^,^2 Ultimately around 1.4% of patients in our cohort were diagnosed with sarcoidosis, a rate much lower than the reported prevalence of CS in patients with unexplained VT/VF. A review by Ribeiro Neto et al. estimated that the prevalence of CS in patients presenting with unexplained VT/VF was between 17% to 28%.1 The lower-than-expected prevalence of sarcoidosis in our study may, in part, reflect the racial composition of our cohort, as sarcoidosis is more common in African American populations and our study population was predominantly White. In addition, the low diagnostic yield seen in this cohort is likely not a reflection of true disease prevalence, but suggests possible gaps in the diagnostic process, based on the low rate of CS evaluations seen in our study.
Beyond CS, our findings highlight a broader issue in the evaluation of patients with unexplained VT/VF. Many patients did not undergo any diagnostic testing, suggesting that underevaluation may lead to missed diagnoses across a spectrum of potentially serious cardiac conditions beyond sarcoidosis. This underscores the importance of implementing systematic and comprehensive diagnostic pathways to ensure that all possible underlying causes are considered.
The demands of busy clinical practice may restrict the ability to prioritize the necessary diagnostic steps for evaluating CS. The nonspecific nature of CS symptoms makes it difficult to diagnose without specialized testing. Although patients with CS may present with symptoms such as syncope, palpitations, nonspecific conduction abnormalities, or heart failure, these symptoms are more commonly attributed to other cardiac conditions. When cardiac dysfunction is the only manifestation of sarcoidosis, the diagnosis is seldom considered.5 The diagnostic workup of CS relies on advanced imaging techniques, such as cMRI and PET, which are expensive and may not be accessible in all clinical settings, especially in resource-limited areas.5 Furthermore, cMRI is generally contraindicated within the first 6 weeks following device placement. In addition, although myocardial biopsy is considered the gold standard for diagnosing CS, it is an invasive procedure that carries inherent risks and is generally reserved for cases where imaging results are inconclusive.1^,^2 This hesitancy to perform invasive tests may contribute to the low diagnostic rates observed in this study. In addition, given the accessibility challenges associated with guideline-recommended diagnostics such as cMRI and PET, we also explored the use of chest CT, even though it is not formally included in the recommended workup for CS. Nevertheless, only 7.4% of patients underwent chest CT, highlighting a persistent underutilization of even more readily available imaging modalities. Although these barriers may not indicate a lack of awareness, they can contribute to the underdiagnosis of CS in patients presenting with unexplained VT/VF.
The consequences of failing to diagnose CS are substantial, as untreated CS patients face an elevated risk of life-threatening arrhythmias, progressive heart failure, and sudden cardiac death.1, 2, 3^,^5 A study conducted by Ekström et al. showed that sudden cardiac death, including both fatal and aborted cases, accounts for approximately 11% to 14% of the presenting manifestations of CS.10^,^11 A study from Padala et al. showed early treatment with immunosuppressive therapies may improve outcomes in VT and left ventricular dysfunction, further highlighting the clinical importance of maintaining a high index of suspicion for evaluating CS in patients presenting with unexplained VT/VF.8 These findings highlight the need to improve clinician awareness of diagnostic indicators and ensure early referral to appropriately equipped centers for timely evaluation and management of suspected CS.
Strengths
The use of the TriNetX research network enabled access to a large, geographically diverse cohort of patients across 56 HCOs, enhancing the generalizability of this study’s findings. This study focused specifically on patients presenting with unexplained VT/VF, a critical clinical scenario where timely identification of underlying CS is essential. By targeting this high-risk subset, the study addresses a key knowledge gap regarding the prevalence of guideline-recommended diagnostic evaluations for CS.
Study Limitations
As a retrospective observational study, it is inherently prone to biases in data collection and interpretation, including the potential for selection bias. Furthermore, the TriNetX database primarily reflects data from the United States, potentially limiting the external validity of our findings to populations or health care systems outside this region. The study uses ICD-10 and CPT codes for patient identification and outcome assessment, making the quality and completeness of the data dependent on the accuracy of coding practices. Any inaccuracies or omissions in coding could lead to bias or misclassification. To protect patient privacy, numbers are rounded up to 10 in the TriNetX database and therefore exact number of patients in those groups are unclear. This may impact results, particularly for small cohorts and infrequent outcomes. Another very important limitation is that although CS was identified in a small portion of patients (1.4%); the diagnostic method could not be verified, as the TriNetX database lacks patient-level clinical detail due to privacy constraints. In addition, although prior studies have established that CS, particularly as the initial or sole manifestation, is associated with poor outcomes, we were unable to analyze long-term clinical outcomes for the small subset of patients diagnosed with CS due to the inherent limitations of the TriNetX database, which does not provide detailed longitudinal follow-up for rare subgroups.
Conclusions
CS remains significantly underdiagnosed in patients presenting with unexplained VT/VF, as highlighted by the notably low utilization of advanced diagnostic testing observed in this study. This underdiagnosis carries significant risks, including delayed treatment and the potential for adverse clinical outcomes such as heart failure or sudden cardiac death. Bridging this diagnostic gap with greater clinician awareness and guideline adherence is the key for timely and appropriate diagnostic testing for CS, particularly in younger patients with unexplained VT/VF. Future studies are needed to further identify underlying barriers to guideline adherence and to explore strategies for improving the diagnosis and management of CS, with the goal of improving care and outcomes for this high-risk population.PerspectivesCOMPETENCY IN MEDICAL KNOWLEDGE: CS should be considered in all patients with unexplained VT/VF, and clinicians should use appropriate imaging techniques, such as MRI, PET, or biopsy, to enhance diagnostic accuracy. A high degree of clinical suspicion and timely diagnosis of CS is essential, as it directly influences management decisions and improves patient outcomes, reducing the risk of cardiac complications.TRANSLATIONAL OUTLOOK: This study highlights the low rate of diagnostic testing for CS in patients with unexplained VT/VF, with only a small fraction undergoing cardiac MRI, PET scans, or myocardial biopsy. This study is the first, to our knowledge, to report on the prevalence of sarcoidosis diagnosis in this population, revealing that it is significantly underdiagnosed, with only 1.4% of patients receiving a diagnosis, far below the expected prevalence of 17% to 28%.Central IllustrationEvaluating Cardiac Sarcoidosis in Patients With Unexplained Ventricular Tachycardia/Ventricular Fibrillation
Funding support and author disclosures
The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ribeiro Neto M.L.Jellis C.L.Joyce E.Callahan T.D.Hachamovitch R.Culver D.A.Update in cardiac sarcoidosis Ann Am Thorac Soc 161120191341135010.1513/Annals ATS.201902-112CME 31322914 · doi ↗ · pubmed ↗
- 2Cheng R.K.Kittleson M.M.Beavers C.J.Diagnosis and management of cardiac sarcoidosis: a scientific statement from the American heart association Circulation 149212024 e 1197 e 121610.1161/CIR.000000000000124038634276 · doi ↗ · pubmed ↗
- 3Sekhri V.Sanal S.De Lorenzo L.J.Aronow W.S.Maguire G.P.Cardiac sarcoidosis: a comprehensive review Arch Med Sci 74201154655410.5114/aoms.2011.24118 PMC 325876622291785 · doi ↗ · pubmed ↗
- 4Patel M.R.Cawley P.J.Heitner J.F.Detection of myocardial damage in patients with sarcoidosis Circulation 1202020091969197710.1161/CIRCULATIONAHA.109.85135219884472 PMC 2778859 · doi ↗ · pubmed ↗
- 5Sharma O.P.Diagnosis of cardiac sarcoidosis: an imperfect science, A hesitant art Chest 12312003181910.1378/chest.123.1.1812527597 · doi ↗ · pubmed ↗
- 6Cacoub P.Chapelon-Abric C.Resche-Rigon M.Saadoun D.Desbois A.C.Biard L.Cardiac sarcoidosis: a long term follow up study P Lo S One 1592020 e 023839110.1371/journal.pone.0238391 PMC 750061832946452 · doi ↗ · pubmed ↗
- 7Fazelpour S.Sadek M.M.Nery P.B.Corticosteroid and immunosuppressant therapy for cardiac sarcoidosis: a systematic review J Am Heart Assoc 10172021 e 02118310.1161/JAHA.121.021183 PMC 864924434472360 · doi ↗ · pubmed ↗
- 8Padala S.K.Peaslee S.Sidhu M.S.Steckman D.A.Judson M.A.Impact of early initiation of corticosteroid therapy on cardiac function and rhythm in patients with cardiac sarcoidosis Int J Cardiol 227201756557010.1016/j.ijcard.2016.10.10127836297 · doi ↗ · pubmed ↗